-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(7): 2143-2146
doi:10.5923/j.ajmms.20251507.12
Received: Jun. 4, 2025; Accepted: Jun. 29, 2025; Published: Jul. 8, 2025

Impact of Scar Localization on the Clinical Course of the Disease and Functional State of the Heart in Patients with Myocardial Infarction
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. L. Alyavi1, A. Ya. Latipov2
1Bukhara Branch of the Republican Research Center of Emergency Medicine, Bukhara, Uzbekistan
2Bukhara State University, Bukhara, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

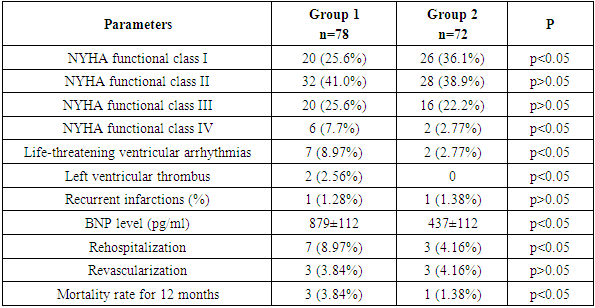
The aim of the study was to evaluate the impact of scar localization on the clinical course of the disease and functional state of the heart in patients with myocardial infarction. Background. Cicatricial changes inevitably lead to myocardial remodeling, a decrease in its contractile function and the development of chronic left ventricular dysfunction. Myocardial infarction of anterior localization has more severe manifestations than myocardial infarction of posterior localization, clinical complications are observed more often. At myocardial infarction of anterior localization of LV, a wider zone of necrosis was accompanied by a significant decrease in myocardial deformation properties and their rate in comparison with posterior infarction. Material and methods. 150 patients who underwent myocardial infarction and were under observation in the cardiology department (mean age was 51±8 years) were included in the study. Patients were divided into two groups depending on scar localization: group 1 (anterior wall myocardial scar (n=78)), group 2 (posterior wall myocardial scar (n=72)). Results. The most significant left ventricular dysfunction was revealed in patients with anterior wall scar. The most severe clinical course of heart failure was observed in patients with the presence of an anterior wall scar. Functional class III-IV according to NYHA was noted in 33% of patients. In the group with scars on the posterior walls, these figures were 24.9%, respectively. Conclusion. Patients with anterior myocardial wall scar are characterized by more severe course of the disease, including high functional classes according to NYHA, frequency of hospital admissions, increased NTproBNP level and high risk of lethal outcome. At the same time, patients with posterior myocardial scarring have a less severe course of chronic heart failure.
Keywords: Myocardial infarction, Chronic heart failure, Anterior wall myocardial scar, Posterior wall myocardial scar
Cite this paper: A. L. Alyavi, A. Ya. Latipov, Impact of Scar Localization on the Clinical Course of the Disease and Functional State of the Heart in Patients with Myocardial Infarction, American Journal of Medicine and Medical Sciences, Vol. 15 No. 7, 2025, pp. 2143-2146. doi: 10.5923/j.ajmms.20251507.12.
Article Outline
1. Introduction
- Chronic heart failure (CHF) after infarction remains one of the main problems of modern cardiology and ranks among the leading causes of death, disability of patients with cardiovascular diseases [1]. The importance of studying postinfarction CHF is associated with a high morbidity rate: in 20-40% of patients after myocardial infarction (MI), CHF is developed within the first year, which significantly worsens their quality of life and prognosis. One of the main factors determining the clinical course and outcome of postinfarction CHF is scar localization in the myocardium [2]. Scarring changes inevitably lead to myocardial remodeling, reduction of its contractile function and development of chronic left ventricular dysfunction. However, in spite of clear differences in pathophysiological processes depending on the zone of myocardial lesion, the impact of scar localization on the course of CHF is still insufficiently studied [3]. According to the results of previous experimental and clinical studies it was noted that MI of anterior localization has more severe manifestations than MI of posterior localization, clinical complications are more often observed [4]. In the research of Golubeva A. V. V. et al. (2020) the heart biomechanics at different localizations of myocardial infarction was studied. Patients were performed speckle-tracking echocardiography. In myocardial infarction of anterior localization of LV, a wider zone of necrosis was accompanied by a significant decrease in myocardial deformation properties and their rate compared to posterior infarction [5]. These differences indicate the need to study scar localization as an independent prognostic factor that can be taken into account when planning an individual treatment. Modern diagnostic methods, including echocardiography, allow to assess the localization, volume and characteristics of scar tissue with high accuracy [6]. As a result, it will create additional opportunities to develop more accurate predictive models that can help clinicians to choose optimal treatment tactics. Besides, the use of these methods contributes to the early identification of patients with high risk of complications and improves their management [7]. The relevance of the study is also determined by the need to improve treatment methods of post-infarction CHF. Considering the importance of scar localization, there is a prospect of developing new approaches to rehabilitation and drug therapy for preventing the development of CHF in patients with scars of different localization [8]. Thus, studying the impact of post-infarction scar localization on the clinical course of heart failure is important for improving the life quality of patients, as well as optimizing treatment and improving prognosis in patients with coronary heart disease [9].The aim of the study was to evaluate the impact of scar localization on the clinical course of the disease and functional state of the heart in patients with myocardial infarction.
2. Material and Methods
- The study included 150 patients who underwent myocardial infarction and were under observation in the cardiology department (mean age was 51±8 year). Inclusion criteria were the presence of post-infarction heart failure (PAHF) confirmed by clinical data, echocardiography and NYHA classification, and patient consent to participate in the study. Exclusion criteria were as follows: patients with comorbidities impacting prognosis (oncology, severe liver and kidney disease). Patients were divided into two groups depending on scar localization: Group 1 (anterior wall myocardial scar (n=78)), Group 2 (posterior wall myocardial scar (n=72)). Echocardiographic parameters were used to evaluate the functional state of the heart: left ventricular ejection fraction, myocardial mass index and the degree of remodeling. Clinical evaluation included determination of the functional class of CHF according to NYHA, hospitalization and frequency of complications (arrhythmias, recurrent infarctions). Additionally, blood tests were performed to determine the level of biomarkers: NTproBNP (sodium uretic peptide type B). Data were collected during the hospitalization phases, after 6 months of follow-up. The obtained data were subjected to statistical processing using Windows XP (Excel) statistical programs by determining Student's criterion.
3. Results
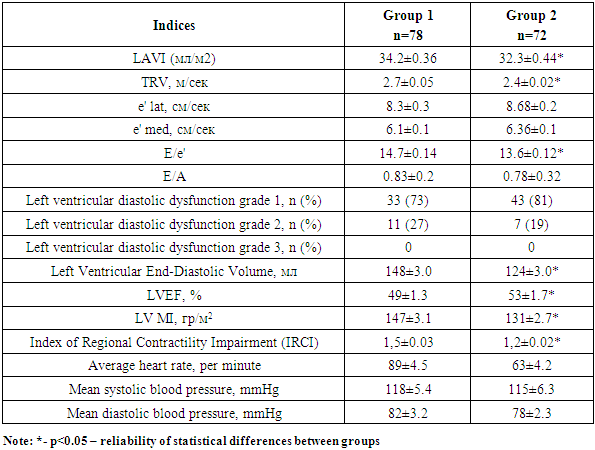
- The performed analyses revealed significant differences between the groups in echocardiographic parameters, clinical manifestations, and disease outcome. The most pronounced left ventricular dysfunction was found in patients with anterior wall scar. The mean ejection fraction was 49%, which was significantly lower than in patients with posterior wall scar (53%). Left ventricular myocardial mass index was significantly higher in the group with previous scarring (132 g/m2 versus 150), indicating significant myocardial remodeling. The index of impaired regional left ventricular contractility was 1.2 versus 1.5, indicating severe myocardial lesion with previous localization. When analyzing the diastolic function of the left ventricle, the average E/A values for the anterior and posterior wall localization groups were 0.83±0.2 and 0.78±0.32, respectively. When comparing the initial E/A values, no significant intergroup differences were found (p>0.05). The values of tissue Doppler velocity (e' lat and e' med) were also significantly lower in the group of patients with previous MI (p>0.05). Grade 1 left ventricular diastolic dysfunction was more frequently recorded in Group 2 (73% versus 81%). Grade 2 left ventricular diastolic dysfunction was more frequently recorded in Group 1 (19% versus 27%) (Tab. 1).
|
|
4. Conclusions
- The results of the study showed that the localization of post-infarction scar has a significant impact on the clinical course and prognosis of heart failure in patients who underwent myocardial infarction. Patients with anterior myocardial wall scarring are characterized by a more severe course of the disease, including high NYHA functional classes, frequency of hospitalizations, elevated NT proBNP levels, and a high risk of death. At the same time, patients with posterior myocardial wall scars have a relatively mild course of CHF.
Conflict of Interests’ Statement
- The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.
ACKNOWLEDGEMENTS
- The authors express their gratitude to the management of the multidisciplinary clinic of Bukhara branch of the Republican Research Center of Emergency Medicine for the material provided for our study.
Ethical Approval and Consent to Participate
- The Research Ethics Board of our institution does not require review or approval of case reports. Our research was carried out in accordance with the World Medical Association Code of Ethics (Declaration of Helsinki).
Source of Funding
- Each of the authors has reviewed and approved this manuscript. None of the authors has a conflict of interest, financial or otherwise. This manuscript is original, no part of it has been previously published and is not being considered for publication elsewhere. The corresponding author agrees to accept full responsibility for authorship at the submission and review stages of the manuscript.