-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(6): 1983-1987
doi:10.5923/j.ajmms.20251506.77
Received: May 22, 2025; Accepted: Jun. 11, 2025; Published: Jun. 21, 2025

Assessment of the Effectiveness of Cognitive Dysfunction Recovery After External Carotid Artery Plasty in Patients with Internal Carotid Artery Occlusion
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShavkat Ibragimovich Karimov1, 2, Abdurasul Abdujalilovich Yulbarisov1, 2, Khojiakbar Kashipovich Alidjanov1, 2, Olimjon Mustapokulovich Akhmatov1, Bunyodbek Tulkinjon ugli Nosirjonov1
1Republican Specialized Center of Surgical Angioneurology, Tashkent, Uzbekistan
2Tashkent Medical Academy, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The purpose of the study was to evaluate the effectiveness of restoration of cognitive dysfunction in patients with occlusion of the internal carotid artery after plastic surgery of the external carotid artery (with traditional and extended patch). From 2010 to 2015, while undergoing treatment in the departments of surgical angioneurology and vascular surgery of the 2nd clinic of the Tashkent Medical Academy (now the multidisciplinary clinic Tashkent Medical Academy), they took part in our study. The average age of the patients was 60.8±7.3 years. The patients were divided into 2 groups depending on treatment tactics: Group 1 - patients with occlusion of the internal carotid artery and plastic surgery of the external carotid artery, with hemodynamically insignificant stenosis on the opposite side (126 people); As shown in Table 4, the mean MMSE scores in both groups after BMQASE treatment were 25.7 ± 0.25 before treatment in the surgical group and 23.0 ± 0.22 in the conservative group. It was detected in patients treated surgically, and in patients treated conservatively - a mild degree of dementia. MMSE scores improved significantly at different times after practice. That is, after 6 months, 57 (53.3%) cognitive impairments remained in a pre- dementia state, 33 (30.8%) had mild cognitive impairment, and 17 (15.9%) had moderate dementia. The MMSE scale scores were positive even after conservative treatment procedures, but from the initial treatment period to 6 months this figure averaged 24.6±0.31 points. After 12 months of follow-up, 25 (40.9%) patients were diagnosed with dementia, and 36 (59.1%) patients were diagnosed with mild cognitive impairment. The results showed that in the postoperative period, in most cases, the mental state of patients changed for the better. Thus, the results of the MMSE test confirmed that the moderate level of dementia changed to a mild level, and the amount of cognitive impairment in the long-term period returned to normal. This once again confirmed that timely surgical intervention on the carotid artery has a positive effect on the recovery of cognitive impairment in patients who have suffered an ischemic stroke. At the same time, in patients of group 2 after conservative treatment, no significant increase in MMSE scores was observed. Thus, the results of the analysis proved its effectiveness in regressing cognitive dysfunction in patients with occlusion of the internal carotid artery at different times after plastic surgery of the external carotid artery. In contrast, practice had no positive effect on the regression of cognitive deficits in the group of patients who did not perform. Research results have shown that the recovery of cognitive dysfunction in the immediate and long term after plastic surgery of the external carotid artery increases in significant percentages.
Keywords: Aterosclerosis, Cognitive disfunction, Occlusion internal carotid artery, Stenosis external carotid artery
Cite this paper: Shavkat Ibragimovich Karimov, Abdurasul Abdujalilovich Yulbarisov, Khojiakbar Kashipovich Alidjanov, Olimjon Mustapokulovich Akhmatov, Bunyodbek Tulkinjon ugli Nosirjonov, Assessment of the Effectiveness of Cognitive Dysfunction Recovery After External Carotid Artery Plasty in Patients with Internal Carotid Artery Occlusion, American Journal of Medicine and Medical Sciences, Vol. 15 No. 6, 2025, pp. 1983-1987. doi: 10.5923/j.ajmms.20251506.77.
Article Outline
1. Introduction
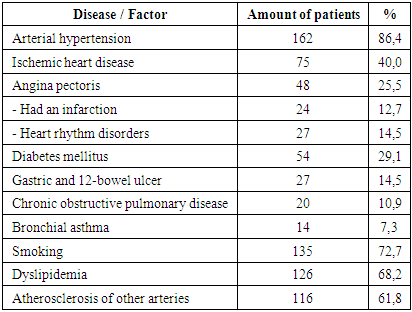
- Annually, more than 6 million cases of ischemic stroke are registered worldwide. Over half a million of these cases occur in Central Asia. In terms of mortality, cerebrovascular diseases rank second after ischemic heart disease (25.7% vs 21.5%). According to leading specialists, the mortality rate after the first stroke is 37%, and after a recurrent stroke, it can rise to 65%. Furthermore, the risk of recurrent stroke within the first five years can reach 42% [1,2]. According to some studies, 6 months after an ischemic stroke, only 29% of patients maintain normal neurological function, while 71% experience cognitive disorders of varying severity or continue to suffer from severe neurological deficits [6,9]. Currently, ischemic cerebrovascular accidents account for approximately 85% of all strokes. According to various sources, more than half of all ischemic strokes are due to atherosclerotic changes in the brachiocephalic arteries [4,5].The effectiveness of surgical treatment for stenotic and occlusive lesions of the internal carotid artery (ICA) in the prevention of primary and recurrent strokes, as well as the restoration of cognitive functions after surgery, has been confirmed by several major studies conducted in the USA and Europe (NASCET, ACAS, ECST) [11,14,16].Cognitive dysfunction impairs the social adaptation of patients, leading not only to a deterioration in quality of life but also to reduced control over the underlying disease and coexisting conditions such as arterial hypertension, atherosclerosis, and diabetes mellitus.In the pathogenesis of cognitive impairment in atherosclerosis of the ICA, two main mechanisms are identified: embolism and brain hypoperfusion. Additionally, occlusive-stenotic lesions of the ICA cause cognitive dysfunction regardless of the presence or absence of white matter damage, as detected by brain MRI. The relationship between carotid revascularization and cognitive function has not been fully established due to the influence of numerous factors: heterogeneity of the clinical picture in patients, the initial state of cerebral perfusion, the time between symptom onset and revascularization; the presence of comorbidities [13,17,20].Purpose of the study. To evaluate the effectiveness of cognitive function recovery in different terms after external carotid artery plasty (traditional and extended with patch placement) in patients with internal carotid artery occlusion.
2. Materials and Methods of the Study
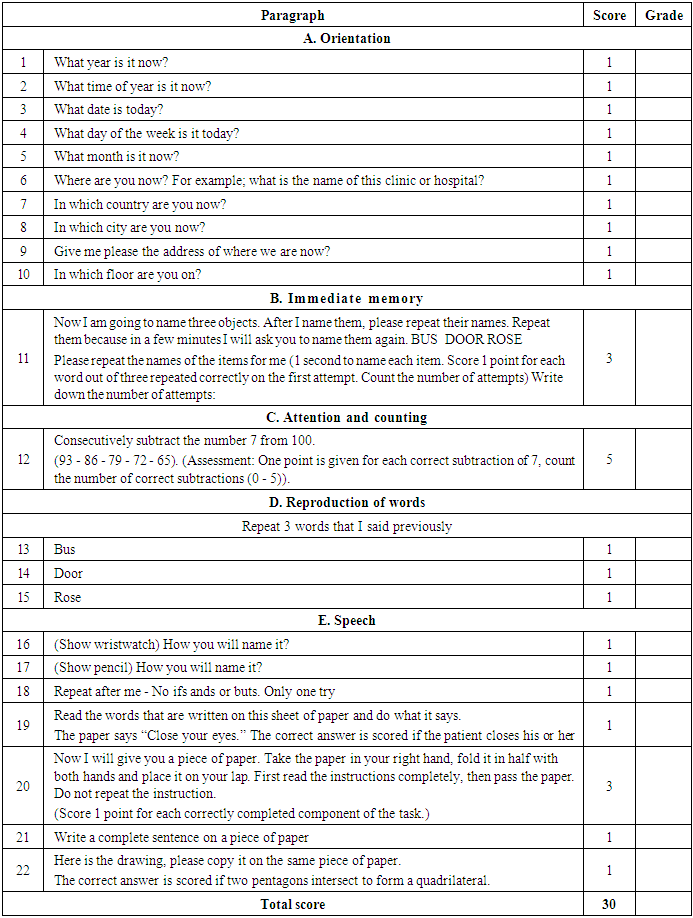
- The study included 187 patients (106 men and 81 women) with atherosclerotic occlusion of the internal carotid artery treated in the departments of surgical angioneurology and vascular surgery of the 2nd clinic of the Tashkent Medical Academy (currently TMA multidisciplinary clinic) during the period from 2010 to 2015. The mean age of the patients was 60.8±7.3 years.Patients were divided into two groups according to the treatment tactics: Group 1 – 126 patients with VCA occlusion who underwent plasty of the external carotid artery, with hemodynamically insignificant stenosis on the opposite side; Group 2 – 61 patients with VCA occlusion who did not undergo surgery for various reasons, and only conservative treatment was used.In all patients cognitive functions were evaluated preoperatively, 6 months and 12 months after surgery using the MMSE scale and other neurological tests.Patients with severe somatic and cardiac pathologies, severe stroke, and psychiatric disorders were excluded.To diagnose atherosclerotic changes in the carotid arteries, an algorithm approved by the ESCT was applied using a Samsung H ultrasound device and MSCT-angiography of the extracranial and intracranial arteries. Cognitive function was assessed using the following methods: the Mini-Mental State Examination (MMSE), the 10-word memory test, the clock-drawing test for assessing frontal dysfunction, the Wechsler digit span test, the Schulte test, and dynamic prosody. The choice of cognitive function assessment methods was based on their ability to functionally reflect cognitive potential.To assess the degree of cognitive impairment, the MMSE – a brief mental state examination scale – was used, consisting of several sections. The final result was determined by summing the scores obtained for completing tasks in each section (Table 1).
|
|
|
|
3. Results of the Study
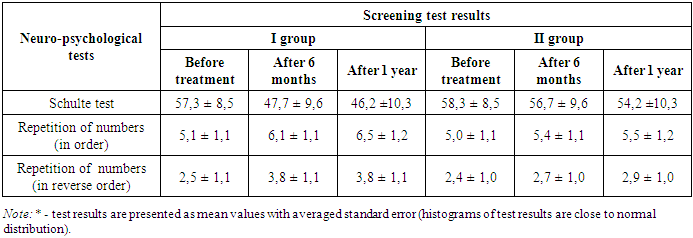
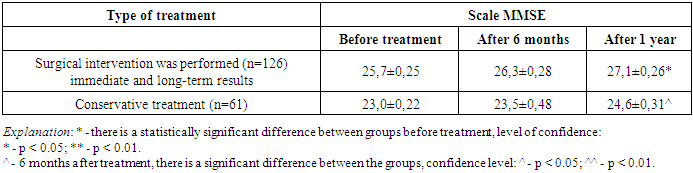
- Table 4 shows that the mean MMSE scores in patients of both groups after treatment differed: in the group of patients who underwent surgery, the pre-treatment score was 25.7±0.25 points, and in the group receiving conservative therapy – 23.0±0.22 points. This indicates a pre-dementia state in patients after surgical treatment and a mild degree of dementia in patients with conservative treatment. MMSE scores improved significantly at various times after surgery: after 6 months, 57 patients (53.3%) still had a pre-dementia state, 33 (30.8%) had mild cognitive impairment, and 17 (15.9%) had moderate dementia.Positive dynamics was also observed after the course of conservative treatment, but after 6 months the average score amounted to 24.6±0.31 points. After 12 months, 25 patients (40.9%) still had dementia, and 36 (59.1%) had mild cognitive impairment. Thus, in the majority of cases after surgical intervention the mental state of patients improved. The MMSE results confirmed the transition of moderate dementia to a milder form and stabilization of cognitive impairment in the long term. This once again proves the positive impact of timely carotid surgery in patients with ischemic stroke on cognitive recovery. At the same time, in the group of patients who received only conservative therapy, there was no significant increase in MMSE scores in different terms.Table 3 also shows the results of other neuropsychological tests used to assess the recovery of cognitive function in patients with CNMC. Thus, according to the Schulte test, the average pre- treatment performance time was 57.3±8.5 sec in the first group and 58.3±8.5 sec in the second group. At 6 months after surgery in the first group, this index improved to 47.7±9.6 sec, and after one year - to 46.2±10.3 sec. In the second group after 6 months and 1 year, the results were 56.7±9.6 sec and 54.2±10.3 sec, respectively. Analysis of the results showed that the patients who underwent surgery had significantly more pronounced positive changes compared to those treated conservatively. In addition, the number repetition tests (forward and reverse order) in the first group after 6 months and a year also showed significant positive results. Before treatment, the result in the forward test was 5.1±1.1; afterward, the results were 6.1±1.1 and 6.5±1.2, respectively. There were no significant improvements in the conservative group. No significant improvement was noted in the conservative group.
4. Discussion
- In our study, patients with internal carotid artery occlusion showed regression of cognitive dysfunction at various times after surgical treatment. The data obtained were confirmed in several ways. A number of authors claim that the regression of cognitive impairment after external carotid artery plasty is not significantly dependent on the technique of its performance. Others, on the contrary, believe that the recovery of cognitive function after surgery is slow. There are studies in the literature devoted to the influence of external carotid plasty in case of occlusion of the internal carotid artery on the degree of cognitive dysfunction. In particular, the efficacy of eversion and classical carotid endarterectomy has been proved with regard to regression of cognitive impairment in the immediate and distant postoperative period. At the same time, temporary use of intraarterial shunt during carotid endarterectomy has no positive effect on the regression of cognitive impairment.In the early postoperative period, the degree of cognitive dysfunction increases significantly, but returns to baseline values within a year. This may be associated with a high risk of middle cerebral artery embolization during temporary shunt placement, especially in the presence of soft embologenic atherosclerotic plaques. At the same time, different techniques of carotid endarterectomy (classical or eversion) do not statistically significantly differ in the incidence of complications, the rate of regression of cognitive dysfunction and improvement of patients' quality of life in the immediate and distant period.The assessment of cognitive function in the remote period after reconstructive surgeries on carotid arteries with occlusive lesions may differ depending on the neuropsychological methods used. Compared to the initial data, an increase in the total MMSE score was observed after 6-9 months. Various memory and attention tests revealed directional changes. No significant changes in cognitive function were observed in the majority of patients. At the same time, the development of asymptomatic ischemic foci in the brain after surgery did not lead to statistically significant differences in the results of neuropsychological tests.
5. Conclusions
- Thus, the analysis of the results showed that in the group of patients with internal carotid artery occlusion the efficacy of cognitive function regression after external carotid artery plasty at different terms after surgery was proved. On the contrary, no positive effect on the regression of cognitive deficit was observed in the group of patients without surgical intervention. The study showed that in the short- and long-term after external carotid artery plasty, recovery of cognitive function occurred in a significant percentage of patients.