Ruziyev Oybek Avlayevich1, Teshayev Shukhrat Jumayevich2
1Termez University of Economics and Service, Termez, Uzbekistan
2Bukhara State Medical Institute named after Abu Ali ibn Sino, Bukhara, Uzbekistan
Correspondence to: Ruziyev Oybek Avlayevich, Termez University of Economics and Service, Termez, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The article examines changes in orchidometric parameters in school-age boys with diabetes mellitus type 1. A comparative analysis of testicular volume changes against orchidometric indicators of healthy children was conducted and relevant conclusions were drawn.
Keywords:
Orchidometry, Testicular volume, Diabetes mellitus, Boys
Cite this paper: Ruziyev Oybek Avlayevich, Teshayev Shukhrat Jumayevich, Comparative Analysis of Testicular Morphometric Parameters in Healthy Boys and Boys with Diabetes Mellitus Type 1, American Journal of Medicine and Medical Sciences, Vol. 15 No. 6, 2025, pp. 1975-1979. doi: 10.5923/j.ajmms.20251506.75.
1. Introduction
Currently, the progressive growth of the world's population is causing an increase in the number of chronic diseases caused by metabolic disorders [1]. One of these diseases is diabetes mellitus (DM), which today is recognized by the WHO as one of the most pressing multidisciplinary problems and is considered a pandemic of non-communicable diseases [12]. According to official data from the International Diabetes Federation (IDF) for 2024, the growth in the incidence of diabetes mellitus type 1 among children and adolescents continues rapidly in all countries of the world, the number of new cases of diabetes mellitus type 1 at the age of 0-14 years increased from 98,200 to 108,300 and at the age of 0-19 years from 128,900 to 149,500 The highest growth was recorded in Africa and the Middle East [2,3]. In all countries of the world, large-scale scientific research is being conducted on the study of diabetes mellitus and its complications. In this regard, the scope of work aimed at the scientific substantiation of changes in all organs and systems of the body, damage to target organs, and the determination of the features of the course of metabolic disorders is quite wide [6]. Modern research is dedicated to studying the prevalence of type 1 diabetes mellitus (DM), the immunological status of children with DM, and the specific features of cardiovascular pathologies, as well as metabolic and endocrine disorders in this population. However, certain aspects remain insufficiently studied, particularly those related to physical development parameters, changes in body composition, and genomic studies in children with type 1 DM [4,5].Numerous studies have also been conducted on the study of reproductive system disorders and testicular morphometry in patients with type 1 DM [9]. In their works, the influence of damage to Leydig and Sertoli cells on testicular development (Dr. Rodolfo Ray, 2021), the influence of mineral metabolism on testicular volume (Ken Ong, 2020), changes in testicular volume in childhood cerebrospinal paralysis, M. Cools et al., 2020), age-related characteristics of testicular growth and development (Jesús Argente, 2022), (comparative analysis of testicular volume and blood testosterone levels in different ethnic groups (Hiromitsu Negishi, 2022) were scientifically studied. Among domestic scientists in the study of orchidometry, one can cite the research of scientists of the Republican Specialized Endocrinology Center named after Y. Turakulov (Z.I. Ismailova, 2021), Samarkand State Medical University (S.A. Ten et al., 2005), Bukhara State Medical Institute (Sh.J. Teshaev et al., 2007) heir works reflect morphometric changes in the testicles in various diseases, the effects of pesticides and other chemical substances on testicular development [14].The size and dimensions of the testes are an important criterion for assessing the male reproductive system, since the effectiveness of spermatogenesis is directly related to them. The testicular volume of men living in different ecological zones has specific regional and ethnic characteristics [7,8]. Various chronic diseases of childhood also have a significant influence on their development. Type 1 diabetes mellitus (DM), when accompanied by metabolic disorders, inevitably affects testicular size and, consequently, the process of spermatogenesis [10,13]. These metabolic disorders also significantly influence indicators of physical development in children, including anthropometric parameters and changes in body composition.These circumstances call for a more in-depth approach by the scientific community to address reproductive system issues in children with type 1 diabetes mellitus, supported by scientifically grounded research closely linked to clinical medicine [11].The purpose of the study is to study the orchidometric parameters of school-age boys with type 1 DM and compare them with healthy children.
2. Materials and Methods
The study involved 212 adolescents, including 112 boys aged 7–17 years diagnosed with type 1 diabetes mellitus (under "D" control at the Bukhara regional branch of the Republican Specialized Scientific and Practical Medical Center of Endocrinology) and 100 healthy boys of the same age group attending Secondary School No. 17 in Bukhara.Testicular size in all participants was measured using an orchidometer developed by the Japanese scientist H. Takihara in 1983. The results were then compared between the healthy group and those with type 1 diabetes mellitus.
3. Research Results and Their Analysis
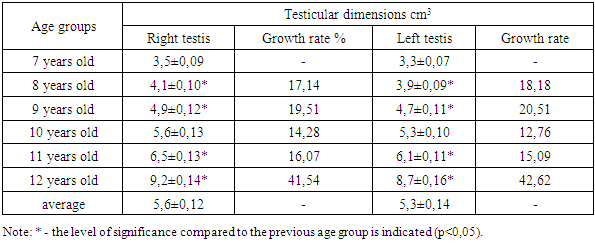
In our study, we investigated testicular developmental delays in boys aged 7–17 years with type 1 diabetes mellitus (DM) using orchidometry. As a baseline, we first assessed orchidometric data from healthy boys in the same age group, then performed a comparative analysis with data from boys diagnosed with type 1 DM.To better understand the nature of these developmental delays, we divided the participants into two age groups: the first group included boys aged 7–12 years (corresponding to the second period of childhood), and the second group included those aged 13–17 years (adolescence). The results of this analysis are presented in Table 1.Table 1. Indicators of testicular size in healthy children aged 7-12 years living in the city of Bukhara (n=53)
 |
| |
|
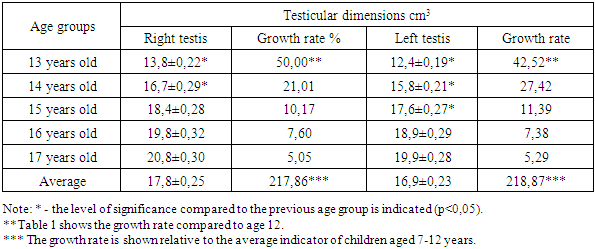
According to the table data, consistent growth in testicular volume is observed in healthy children aged 7 to 12 years. This growth is associated with the process of physiological growth and preparation for sexual maturity. In healthy children aged 7-12 years, the volume of the right testicle increased from 3 to 13 cm3, averaging 5,6±0,12 cm3, and the volume of the left testicle increased from 3 to 12 cm3, averaging 5,3±0,14 cm3.The size of the right testicle averaged 3,5±0,09 cm3 at the age of 7 years and increased almost steadily every year. At 8 years – 4,1±0,10 cm3 (growth rate 17,14%), at 9 years – 4,9±0,12 cm3 (19.51%), and at 10 years – 5,6±0,13 cm3 (14,28%). At the age of 11, this indicator reached 6,5±0,13 cm3 (16,07%) and at the age of 12, it sharply increased to 9,2±0,14 cm3, with an increase of 41,54%.We observed a similar increase in the left testicle: at 7 years 3,3±0,07 cm3, at 8 years 3,9±0,09 cm3 (18,18%), at 9 years 4,7±0,11 cm3 (20,51%), at 10 years 5,3±0,10 cm3 (12,76%), at 11 years 6.1±0.11 cm3 (15.09%) and at 12 years 8,7±0,16 cm3 (42,62%).It should be noted that the increase in testicular volume at ages 8, 9, 11, and 12 years was statistically significant (p < 0.05), indicating the onset of active gonadal development during this period. The average testicular volume in the 7–12 age group was 5.6 ± 0.12 cm³ for the right testis and 5.3 ± 0.14 cm³ for the left testis.An analysis of the results obtained for the second age group (13–17 years) is presented in Table 2.Table 2. Indicators of testicular size in healthy 13–17-year-old children living in the city of Bukhara (n=47)
 |
| |
|
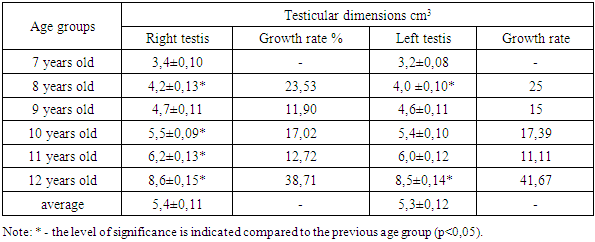
According to the table data, consistent and to a certain extent stable growth in testicular volume was observed in children aged 13 to 17 years. This is explained by growth, endocrine changes during puberty, and activation of the gonads.In healthy children aged 13-17, the volume of the right testicle increased from 11 to 23 cm3, averaging 17,8±0,25 cm3, and the volume of the left testicle increased from 10 to 22 cm3, averaging 16,9±0,23 cm3.At the age of 13, the volume of the right testicle was 13,8±0,22 cm3, and the volume of the left testicle was 12,4±0,19 cm3. This is a very large increase compared to the age of 12, with an increase of 50,00% in the right testicle and 42,52% in the left testicle (p<0,05). This growth indicates the beginning of adolescence and the active period of puberty.At the age of 14, the right testicle increased to 16,7±0,29 cm3 (21,01%), the left testicle to 15,8±0,21 cm3 (27,42%). At the age of 15, the growth rate slowed down, the right testicle was 18,4±0,28 cm3 (10,17%), the left testicle was 17,6±0,27 cm3 (11,39%).At 16 and 17 years of age, testicular volumes stabilized, and the growth rate decreased: at 16 years of age, the right testicle was 19,8±0,32 cm3 (7,60%), the left testicle – 18,9±0,29 cm3 (7,38%), and at 17 years of age, respectively, 20,8±0,30 cm3 and 19,9±0,28 cm3 (avg. 5%).Average indicators in the age range of 13-17 years:• Right testis: 17,8±0.25 cm3, which is 217,86% higher than the average age of 7-12 years.• Left testis: 16,9±0,23 cm3, which is also 218,87% growth.A marked increase in testicular volume at age 13 indicates the onset of adolescence. In the following years, the growth rate stabilizes, and by age 17, testicular volume typically reaches the level characteristic of adult males. This progression represents a natural physiological aspect of puberty and holds significant value in both clinical and demographic research.Our results show that testicular volume grows gradually and steadily, with an average growth rate of about 15-20% per year. In analyzing the extent of testicular growth within the 7–12-year age group, we observed that the volume of the right testis increased from 3,5 cm³ to 9,2 cm³, while the left testis grew from 3,3 cm³ to 8.7 cm³.A significant growth spurt was observed in 12-year-old children, with the growth rate reaching 41-42%. These changes are indicative of the onset of puberty. The 13-year-old growth spurt (active phase of puberty) during the transition from 12 to 13 years of age showed the following: right testicle: +50% growth (9,2 → 13,8 cm3), left testicle: +42,5% growth (8,7 → 12,4 cm3). This marks the beginning of adolescence and is associated with an increase in the activity of testosterone and gonadotropic hormones.Stable growth was observed at ages 14 and 15. At 14 years, the average increase in testicular volume was approximately 20–25%, while at 15 years, the growth rate slowed to around 10–11%. This decline may indicate a transition into the late stages of puberty.In our study, we observed a slowdown and slight stabilization in testicular growth at ages 16–17. During this period, the growth rate decreased to approximately 5–7%, with testicular volume approaching its maximum level. By this stage, testicular volume typically stabilizes between 20–25 cm³ and remains within this range up to the age of 20.Analysis of the average testicular growth at the age of 7-17 years showed that the testicular volume averaged 5,5 cm3 in the right testicle at the age of 7-12 years, 5,3 cm3 in the left testicle, and averaged 17.8 cm3 in the right testicle and 16,9 cm3 in the left testicle at the age of 13-17.When analyzing the growth coefficient, an increase of 3.2 times was observed in the average indicator of 13-17 years compared to the average indicator in the age range of 7-12 years (right 5,6 → 17,8 cm3, left 5,3 → 16,9 cm3). Almost 70-75% of this growth occurs in the 3rd year after the age of 12.Based on the results, it can be concluded that a significant increase in testicular volume occurs between the ages of 12 and 13, clearly marking the onset of puberty. The active growth phase from 13 to 15 years corresponds to the peak of hormonal activity. Growth slows down at ages 16 to 17, indicating the completion of fertility potential development. Throughout this period, the right testicle consistently has a larger volume than the left, reflecting normal anatomical asymmetry.In our study, we also examined orchidometric parameters in 112 boys of the same age group diagnosed with type 1 diabetes mellitus, residing in various districts of the Bukhara region and monitored at the Bukhara Regional Dispensary of the Republican Specialized Scientific and Practical Medical Center of Endocrinology. The aim was to assess the impact of type 1 DM on the sexual growth and development of these children.During sexual development, children experience significant physical and physiological changes driven by the sex glands and their associated hormonal fluctuations. An increase in testicular volume is a key indicator of the activation of testosterone production and gonadal maturation. However, chronic endocrine conditions, such as type 1 diabetes mellitus, can adversely affect this growth process. The results of our analysis are presented in Table 3.Table 3. Indicators of testicular size in children aged 7-12 years with type 1 DM living in the Bukhara region (n=45)
 |
| |
|
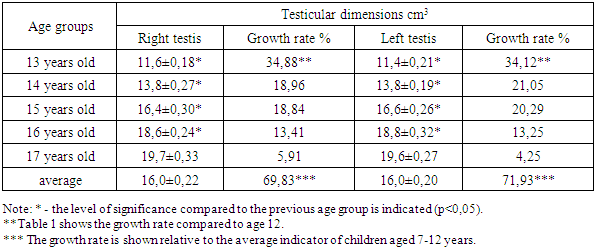
As shown by the data in the table, testicular volume increased steadily and regularly with age:In children with type 1 DM aged 7-12 years, the volume of the right testicle increased from 3 to 12 cm3, averaging 5,4±0.11 cm3, and the volume of the left testicle increased from 3 to 12 cm3, averaging 5,2±0,12 cm3.At 7 years of age, the right testicle was 3,4±0,10 cm3, the left testicle 3,2±0,08 cm3. This was taken as an initial indicator. Significant growth was observed at the age of 8 years - right testicle 4,2±0,13 cm3 (growth rate 23,53%), left testicle 4,0±0,10 cm3 (25%). This increase is statistically significant (p<0.05). At the age of 9 years, growth slowed somewhat – 11,90% (right) and 15% (left), and at the age of 10 years, another significant increase was noted – 5,5±0,09 cm3 (right) and 5,4±0,10 cm3 (left) (p<0,05).At the age of 11, the growth rate is relatively low – 12,72% and 11,11%, respectively, but there is a steady increase in volume. At the age of 12, a very large jump was also observed: 8,6±0,15 cm3 (right, 38,71%) and 8,5±0,14 cm3 (left, 41,67%). This increase is also statistically significant (p<0,05). Average values: right testicle – 5,4±0,11 cm3, left testicle – 5,3±0,12 cm3.These results indicate that a traditional increase in testicular volume can also be observed in children with type 1 DM during puberty. Especially high growth rates at the age of 12 indicate the activation of testosterone secretion and the development of the gonads in children. However, the slowdown in growth rates at the ages of 9 and 11 may be associated with hormonal imbalance or the effects of metabolic stress against the background of DM.In children with type 1 diabetes living in the Bukhara region, an age-appropriate increase in testicular volume is observed. Although growth rates vary across different ages, increases at 8, 10, and especially 12 years are statistically significant, indicating that sexual development is generally proceeding without delay. This confirms that pubertal changes can occur in children with diabetes mellitus; however, regular clinical monitoring is essential to ensure healthy development.In the subsequent age group of boys with type 1 diabetes mellitus (aged 13–17 years), the dynamics of orchidometric growth were studied. It was observed that their testicular development lags behind that of healthy peers in the same age group. The results are presented in Table 4.Table 4. Testicular size indicators in children aged 13-17 years with type 1 diabetes mellitus living in the Bukhara region (n=67)
 |
| |
|
Analysis of the results showed that in children with type 1 DM aged 13-17 years, the volume of the right testicle increased from 10 to 21 cm3, averaging 16,0±0.22 cm3 and the volume of the left testicle increased from 10 to 20 cm3, averaging 16,0±0,20 cm3. The overall growth rate is around 70%.The age of 13 is considered the initial stage of puberty. In the right testicle, an increase of 34,88% was observed, and in the left testicle – 34,12% compared to 12 years. This growth is at a high rate, reflecting the recent onset of puberty. A statistically significant difference was revealed.At the age of 14, the average volume of the right and left testes was equal to 13,8 cm3, and an increase of 18,96% and 21,05% was noted, respectively, compared to the age of 13. At this stage, although the growth rate is lower, it is observed that it continues steadily.At the age of 15, the right testicle had an average volume of 16,4 cm3, and the left testicle – 16,6 cm3. Compared to the previous age group, the growth was 18,84% and 20,29%, respectively. The increase in testicular volume is still actively continuing, during which the middle stage of the pubertal process is observed.By age 16, the testicular volume reached 18,6 cm3 on the right and 18,8 cm3 on the left. However, the growth rate slowed to 13,41% and 13,25%, respectively. This indicates reaching the highest stage of puberty.At the age of 17, the right testicle grew to 19,7 cm3, the left testicle to 19,6 cm3. But the growth rate is very low – 5,91% and 4,25%, respectively. This indicates that the pubertal process is almost complete. No statistically significant growth was recorded.The results show that children with type 1 diabetes mellitus experience a gradual and consistent increase in testicular volume during puberty. The most significant increase occurs at age 13, marking the onset of puberty. In the following years, the growth rate slows down, and by age 17, testicular volume appears to be approaching the final stage of pubertal development.Factors such as insulin therapy and the level of blood glucose control can be considered among the main causes of delayed puberty. The fact that most of the annual increases are statistically significant (p < 0.05) indicates that puberty is not delayed but is progressing more slowly than normal. In adolescents with type 1 diabetes mellitus (DM), testicular volume gradually increases from 13 to 17 years of age. Although this growth is slow, the pubertal process does not stop completely. In such children, it is very important to regularly monitor hormonal growth indicators and, if necessary, provide endocrinological assistance.
4. Conclusions
In boys aged 7-12 years with type 1 DM in orchidementia, the right testicle lagged behind by 0,2 cm3, while in the left testicle, this difference was not noticeable. In the 13-17 age group, the lag in children with type 1 DM was 1,8 cm3 in the right testicle and 0,9 cm3 in the left testicle. The testicular growth rate from 7 to 17 years of age was 21,8% in healthy children and an average of 70% in children with type 1 DM. It has been proven that testicular growth retardation is most pronounced after 13 years of age.
References
| [1] | American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021 // Diabetes Care. 2021. Vol. 44, No. Supplement 1. P. S15–S33. |
| [2] | World Health Organization. Classification of diabetes mellitus. 2023. |
| [3] | World Health Organization, International Diabetes Federation. Definition and diagnosis of diabetes mellitus and intermediate hyperglycaemia: report of a WHO/IDF consultation. 2019. |
| [4] | Insel R.A. et al. Staging Presymptomatic Type 1 Diabetes: A Scientific Statement of JDRF, the Endocrine Society, and the American Diabetes Association // Diabetes Care. 2015. Vol. 38, No. 10. P. 1964–1974. |
| [5] | Ziegler A.G. et al. Seroconversion to Multiple Islet Autoantibodies and Risk of Progression to Diabetes in Children // JAMA. 2013. Vol. 309, No. 23. P. 2473. |
| [6] | International Diabetes Federation. IDF Diabetes Atlas, 10th edn. Brussels, Belgium: International Diabetes Federation, 2021. |
| [7] | Mayer-Davis E.J. et al. ISPAD Clinical Practice Consensus Guidelines 2018: Definition, epidemiology, and classification of diabetes in children and adolescents // Pediatr. Diabetes. 2018. Vol. 19. P. 7–19. |
| [8] | Torbey, P., Haddad, M., et al. Normative data of testicular volume in children and adolescents: A multicenter study. Journal of Pediatric Urology, 2021, 17(3), 350.e1–350.e6. DOI: 10.1016/j.jpurol.2020.12.018. |
| [9] | Ismail, I. M., et al. "Ultrasound assessment of testicular volume in children: Accuracy and standardization." Pediatric Radiology, 2020, 50(4), 516–523. DOI: 10.1007/s00247-019-04561-z. |
| [10] | Ramos, L., et al. (2022). Relationship between testicular volume and pubertal development in boys aged 6 to 17 years. Hormone Research in Paediatrics, 2022, 95(2), 100–106. DOI: 10.1159/000520034. |
| [11] | Eldeeb, M. M., et al. Testicular size as a marker of delayed puberty in boys with chronic diseases. Clinical Pediatrics, 2023, 62(1), 43–50. DOI: 10.1177/00099228221129086. |
| [12] | Cho, H. W., et al. Longitudinal changes in testicular volume in Korean boys: A prospective cohort study. Annals of Pediatric Endocrinology & Metabolism, 2020, 25(4), 222–228. DOI: 10.6065/apem.2040140.070. |
| [13] | Dedov I.I., Kuraeva T.L., Peterkova V.A. Diabetes mellitus in children and adolescents. Moscow: GEOTAR-Media, 2013. 271 p. |
| [14] | Taranushenko T.E., Proskurina M.V. Modern view on the issues of epidemiology and manifestation of type 1 diabetes mellitus in pediatrics, Doctor. Ru Vol. 23, No. 3, 2024; DOI: 10.31550/1727-2378-2024-23-3-55-61. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML