-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(6): 1941-1945
doi:10.5923/j.ajmms.20251506.67
Received: May 25, 2025; Accepted: Jun. 13, 2025; Published: Jun. 20, 2025

Morphological and Immunohistochemical Studies of Adenomyosis in Women of Fertile Age
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLN. Sh. Shorakhmedova, Sh. I. Ruziyev
Republican Scientific-Practical Center for Forensic Medical Expertise, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Adenomyosis, characterized by the insertion of endometrial tissues into the myometrium, is one of the most common gynecological diseases affecting women of fertile age. This condition can cause various clinical manifestations, including dysmenorrhea, dyspareunia, and infertility, making it important for public health and reproductive medicine. Understanding the morphological changes that occur as a result of adenomyosis, as well as the analysis of immunohistochemical markers that play a role in the pathogenesis of this disease, is of key importance for the development of effective diagnostic and therapeutic approaches.
Keywords: Adenomyosis, Morphological aspects, Immunohistochemical aspects, Reproductive age, Women, Inflammation
Cite this paper: N. Sh. Shorakhmedova, Sh. I. Ruziyev, Morphological and Immunohistochemical Studies of Adenomyosis in Women of Fertile Age, American Journal of Medicine and Medical Sciences, Vol. 15 No. 6, 2025, pp. 1941-1945. doi: 10.5923/j.ajmms.20251506.67.
1. Introduction
- Morphological studies of tissues affected by adenomyosis enable the identification of characteristic changes, such as endometrial hyperplasia and structural abnormalities of the myometrium, which contribute to a more accurate classification of the disease [1]. Additionally, immunohistochemical analysis can provide valuable information about the pathogenic mechanisms of adenomyosis, including the activation of inflammatory processes and changes in the expression of hormones such as estrogens and progesterone. Studying the interactions between these factors helps to gain a deeper understanding of how adenomyosis affects reproductive function and the overall health of women [2].It is important to note that adenomyosis is not always associated with symptoms, which can complicate its diagnosis in the early stages. Therefore, further investigation of the morphological and immunohistochemical aspects of adenomyosis in women of reproductive age will not only improve the understanding of the disease's pathogenesis but also allow for the development of more effective screening and treatment methods. In this context, this study aims to provide an in-depth analysis of the changes associated with adenomyosis, with the goal of enhancing the rationale for clinical decisions and improving the quality of life for women suffering from this condition [3]. Adenomyosis is a safe disease of the uterus, in which glands on the endometrium floor and uterine myometrium floor are pathologically manifested in stroma, and a specific unit in determining the causes of anomalous bleeding from the uterus (Bacchus) (polyp, adenomyosis, leukomyoma, malignant and hyperplasia, coagulopathy, dysfunction of the ovule, hyperplasia of the endometrium is a study of yatrogenic and (International Society of gynecology and obstetrics) unclassified Bacchus causes [4]. While it has always been considered a classic case of recurrent miscarriages in women over 40 years of age with diagnosed pain and multiple menstrual bleeding at the time of hysterectomy, epidemiologically these cases have been found to be completely different. Adenomyosis is detected in young women using visualization techniques such as transvaginal ultrasound and magnetic resonance imaging, in cases where pain, anomalous uterine bleeding, infertility or symptoms are not observed in most cases [5]. Nevertheless, today there is no single opinion on the identification and classification of adenomyotic lesions, both histopathologically and visualistically, and this presents some difficulties and inaccuracies in the diagnosis. It is considered necessary to introduce a unified and general reporting system to improve our understanding of the features of visualization, their relationship with pathogenetic theories, their importance in terms of clinical symptoms and impact on treatment. In fact, while the pathogenesis of adenomyosis remains uncertain, no theory can explain all the different phenotypes of the disease. In addition, adenomyosis often occurs along with other gynecological diseases such as endometriosis and uterine fibroids [6]. This increases the heterogeneity of available data. It also requires lifelong administration of treatment activities, as the disease, along with adverse effects on the mother's lifestyle in cases of menstrual symptoms, fertility and pregnancy, further increases the risk of miscarriage and obstetric complications [7].Despite some difficulties in studying the relationship between adenomyosis and infertility, according to metatahlil results, the negative effects of adenomyosis on pregnancy have been proven. On the basis of the origin of infertility in adenomyosis, an approximate four types of mechanisms lie, which are: disorders of the endometrial floor peristalsis, the receptivity of the endometrium, the connection with implantation and chronic endometritis. Adenomyosis and endometriosis will have a number of common features in terms of clinical appearance, morphology, as well as molecular changes. The two main differences between them will be related to the origin of the ectopic endometrium (in basal - adenomyosis, functional - endometriosis) and the anatomical location of its lesions (inside or outside the uterus, respectively) [8].G. Younes and others, in their 2017 metatahlil results, proved the detrimental effects of adenomyosis on the outcomes of Assisted Reproductive Technology. In a comparative analysis of the effectiveness of extracorporeal insemination (EKU) in 519 patients with adenomyosis and 1,535 women without adenomyosis, implantation rates, pregnancy clinic, progressive pregnancy and live birth frequency have been shown to be statistically significantly lower in the group of patients with adenomyosis, while the frequency of miscarriage is significantly higher. M. published in 2022 [9]. In the metataholic of CozzoLino and others, pregnancy in adenomyosis, a decrease in the frequency of clinical and progressive pregnancy, as well as an increase in the frequency of miscarriage, are once again reliably proven. Thus, the results of a modern study with high levels of evidence have been studied to negatively affect the ECU outcomes of adenomyosis. Therefore, the previously theoretical bond between adenomyosis and infertility has now been shown to be purely Real [10].Scientific research is a promising comparative observational study, consisting of several directions and stages.Scientific research is presented consisting of prospective comparative observational studies involving several fields and stages. During 2020-2024, 142 cases of adenamiasis were studied, of which clinical cases were studied in women of reproductive age between the ages of 18 and 42 in the gynecology department of the multidisciplinary clinic of the Tashkent Medical Academy, prospective and retrospective analysis data were obtained. In addition, morphological examinations were carried out in the Department of "adult pathology and diagnosis of biopsy diagnostics" of the Republican Center for pathological anatomy.The study was of a complex nature and included clinical and morphological-immunogystochemical components:* Prospective Cohort Study of clinical cases of adenamiasis in women of reproductive age;* Retrospective analysis of disease histories of women with adenamiasis of reproductive age;* Morphological and immunogystochemical study of the uterus and the "junctional zone".Based on the analysis of the research materials, patients were divided by age groups as follows:• Group 1-ages 18-22: 19 (13.4%) <BR>;• Group 2 -ages 23-27: 34 (23.9%) <BR>;• Group 3-ages 28-32: 48 (33.8%) <BR>;• Group 4-ages 33-37: 31 (21.8%) <BR>;• Group 5-ages 38-42: 10 (7.1%).The following methods were used to carry out the study:1. Analysis of clinical anamnestic and laboratory indicators of women with adenamiasis in reproductive age;2. Study of specific morphological and histochemical changes in the uterus and endometrium of women with adenamiasis in reproductive age;The clinical examination included a detailed analysis of Anamnesis, specifically focusing on risk factors for female reproductive age (hormonal contraception use, obstetric Anamnesis, surgical interventions performed, etc.q.). All patients received a standardized gynecological examination, during hospitalization, on the 3rd and 7th days, as well as an assessment of adenamiasis severity on the PASS (Pictorial Assessment of Adenomyosis Severity Score) Scale when excreted. The functional result was evaluated on the 30th and 90th days after treatment using the EHP-30 (Endometriosis Health Profile-30) scale. Determination of immunogystochemical changes and specific aspects of "junctional zone" and myometrium in women with adenamiasis in reproductive age;Study of multiplexed morphometric indicators of "junctional zone", myometrium and endometrium in women with adenamiasis in reproductive age. According to the types of adenamiasis, the materials were distributed as follows: diffuse adenamiasis - 71 (50.0%), focal adenamiasis - 36 (25.4%), superficial adenamiasis - 21 (14.8%), deep adenamiasis - 14 (9.8%).Statistical analysis was carried out in accordance with the methods of statistical analysis on interpretation in MS Office Excel 2007 and STATISTICA for Windows 10 application package. The significance level of the differences was used: p<0.05. For analysis, the Student t-criterion is used when the selected norm is distributed: changes in the dynamics within groups and among the population are studied. Correlation analysis was carried out, and the Pearson coefficient was used in normative distributions; the Spirman coefficient was used for the distribution. Studies conducted at the Republican Center for pathological anatomy during 2020-2024 analyzed the death of 142 women of reproductive age (23-41 years) whose diagnosis of adenomyosis was morphologically confirmed. Based on the analysis of the research materials, it turned out that patients died between the ages of 23 and 41. Initially, the patient's medical history and autopsy report were analyzed. Patients with adenomyosis at reproductive age were divided into the following groups by incidence and age of major diseases in women's uterine myometry and ovarian tissue, including: Group 1-9 (22.5%) by age 18-22; group 2 - 14 (35.0%) by age 23-27; group 3-8 (20.0%) by age 28-32; Group 4-7 (17.5%) by age 33-37; group 5 – 38-42 accounted for 2 (5.0%).
2. The Results of the Study
- The reproductive organs of the uterus consist of anatomical cells, endometrium, myometrium and serous membrane, histological and functional features of each uterus were studied. However, in 2011, at the 11th Congress of Gynecologists, held in France, the endometrium and myometrium were combined into a "junctional zone", which presented data on the pathogenesis of adenomyosis and endometriosis. During histological examination of the uterus and its mediastinum, the pathologist performs an autopsy. Macroscopic examination of autoimmune diseases of the uterus and its environment has shown that autoimmune diseases can occur with autoimmune diseases. After that, 10% of the solution was neutralized with formalin, alcohols were removed and paraffin was added. Histological properties of hematoxylin-eosin, SCHICK reaction and Van gieson.The results of pathomorphological studies:1. The presence of myometrium, endometrial glands and stroma2. Hypertrophy of myometrial fibers3. Infiltration of mucous membranes4. Violations of the boundaries of the endometrium and myometriumMorphologically, the endometrium and myometrium can be divided into two equal parts by the basement membrane. Spirally arranged arteries are located on the border with the endometrium, and branched arteries and veins are located at the junction with them. With endomyometriosis, the plough has no pronounced morphological features, and with adenomyosis, there is a violation of this boundary. Since the basal and functional stroma of the endometrium consist of fibroblasts and histiocytes of varying degrees of variability, spiral structures are formed with the spiral connection of thin arterial vessels in the oral direction. The endometrium, consisting of asanas, basophils and eosinophils, is characterized by a variety of epithelial cells.
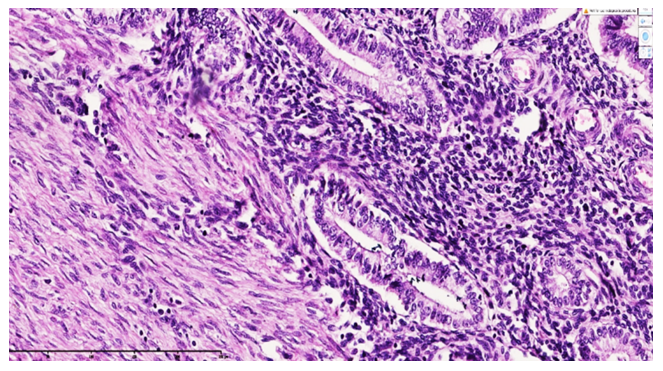 | Figure 1. 28th diagnosis of adenomyosis confirms the diagnosis of a diseased uterus. The endomyometrium is an area where fibroblasts are damaged and the basal region of the endometrium is atrophied to improve myogenesis and coronary artery development. Hyperchromia of the endometrial and myometrial fibroblast nuclei is accurate. Without A doubt. E. The first 20x10. In myometrial subendometrial contraction of the rotator cuff, the muscles contract in a striated section, while the small-caliber artery contracts in cross-section and the Vein contracts in cross-section. The endometrium and myometrium of the oral "junctional zone" are characterized by a pronounced morphological pattern |
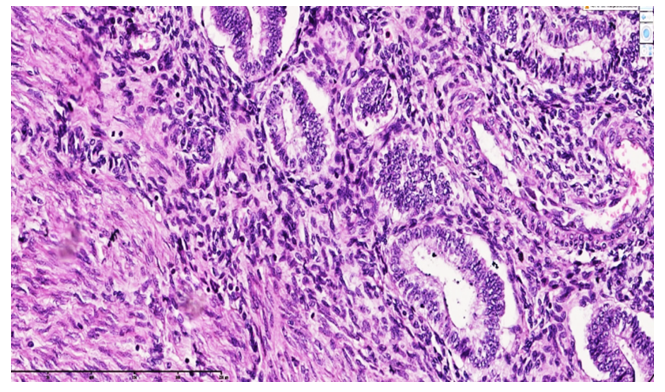 | Figure 2. Example 2. A 35-year-old woman. The diagnosis of adenomyosis is confirmed patient uterus. The boundaries in the endomyometrial Sox are uneven and notable-the fibroblasts in the border Sox are uniform in appearance, and the endometrial gland is found to be surrounded by foci of myogenesis finding evolutionarily around the basal floor. HyperChrome-core fibroblasts are detected in the endometrium and myometrium. Paint G.E. Size 20x10 |
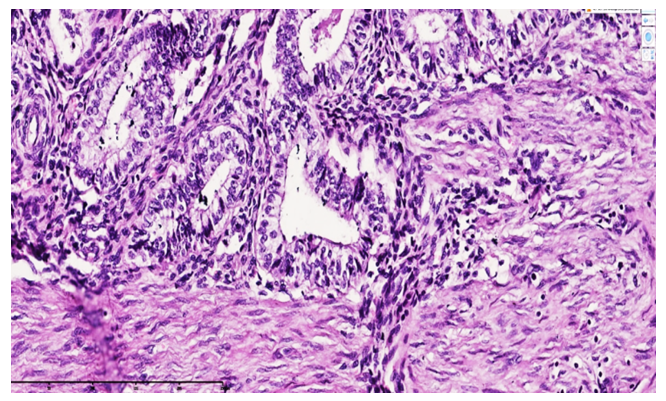 | Figure 3. Example 3. A 32-year-old woman. The diagnosis of adenomyosis is confirmed patient uterus. The boundaries in the endomyometrial Sox are uneven and notable-the fibroblasts in the border Sox are uniform in appearance, and the endometrial gland is found to be surrounded by foci of myogenesis finding evolutionarily around the basal floor. HyperChrome-core fibroblasts are detected in the endometrium and myometrium. Paint G.E. Size 20x10. The presence in the ham endometrium of the tutuams of the same collagen fibers, located in the ora ora, partially confirms the presence of a passing soxa. The 13 uterus ecstyped with the diagnosis of adenomyosis between endometrium and myometrium refers to the same-looking fuchsinophilic fiber sandwich 2+1 i.e. a border that is iboart from two layers of collagen fibers and sparse fibrous connective tissue in the oral. This, in turn, is precisely in this passing field, where the nuclear cytoplasmic index of myocytes is different, and in the endometrium, cells with tumors are detected, where the nuclei of excited fibroblasts in the Supra basal Sox gland stroma are painted dark HyperChrome, the cytoplasm is rich in pale eosinophilic inputs |
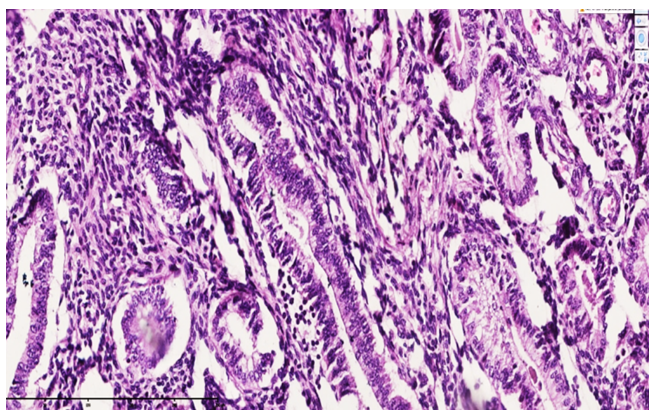 | Figure 4. Pattern 4. A 38-year-old woman. The diagnosis of adenomyosis is confirmed patient uterus. In the endometrium floor, transfor-Masialized fibroblasts and foci of myogenesis are detected, located unevenly and chaotically. Most are found to be surrounded by foci of myogenesis, which are finding evolution around the endometrial gland. HyperChrome-core fibroblasts are detected in the endometrium and myometrium. Paint G.E. Size 20x10 |
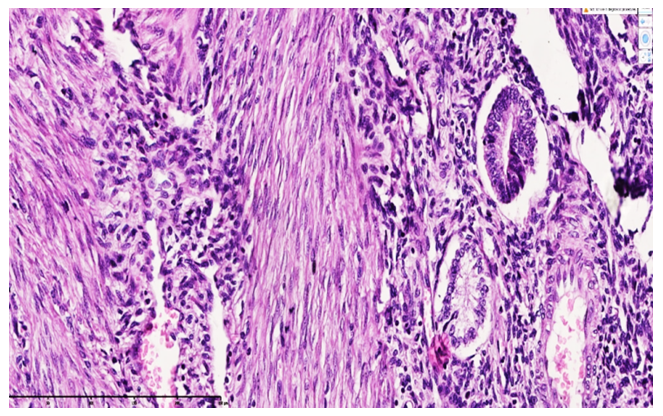 | Figure 5. Pattern 5. A 38-year-old woman. The diagnosis of adenomyosis is confirmed patient uterus. In the endometrium floor, transfor-masialized fibroblasts and foci of myogenesis are detected, located unevenly and chaotically. Most are found to be surrounded by foci of myogenesis, which are finding evolution around the endometrial gland. HyperChrome-core fibroblasts are detected in the endometrium and myometrium. Paint G.E. Size 20x10 |
3. Сonclusions
- The modern interpretation of the morphological and immunogystochemical characteristics of adenomyosis allows you to more thoroughly understand the pathogenetic mechanisms of this disease, clarify the criteria for differential diagnostics and develop new areas of treatment. In Uzbekistan, the study of morphological and immunogystochemical aspects of advanced adenomyoses in women of reproductive age is an urgent task, large-scale scientific research should be carried out in this area.