-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(6): 1921-1924
doi:10.5923/j.ajmms.20251506.62
Received: May 21, 2025; Accepted: Jun. 15, 2025; Published: Jun. 20, 2025

Excess Body Weight and Abdominal Obesity as Determinants of Carbohydrate Metabolism Disorders
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNishanova M. S.
Assistant of the Department of Hospital Therapy and Endocrinology, Andijan State Medical Institute, Andijan, Uzbekistam
Correspondence to: Nishanova M. S., Assistant of the Department of Hospital Therapy and Endocrinology, Andijan State Medical Institute, Andijan, Uzbekistam.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study is devoted to assessing the prevalence of prediabetes and type 2 diabetes mellitus among the rural and urban population of the Andijan region, as well as identifying the relationship between the degree of obesity and carbohydrate metabolism disorders. 3400 individuals over 40 years of age were included in the study. BMI, waist and hip circumference, and their ratio were assessed. It was established that excess body weight prevailed in both populations, and obesity of I-II degree was reliably associated with a higher frequency of IGT, IFG, and DM2. The abdominal type of obesity was a characteristic feature of groups with impaired carbohydrate metabolism. The identified differences between rural and urban populations emphasize the need for a differentiated approach to screening and prevention of metabolic diseases.
Keywords: Pre-diabet, BMI, Obesity, Waist circumference (WC), Hip circumference (HB)
Cite this paper: Nishanova M. S., Excess Body Weight and Abdominal Obesity as Determinants of Carbohydrate Metabolism Disorders, American Journal of Medicine and Medical Sciences, Vol. 15 No. 6, 2025, pp. 1921-1924. doi: 10.5923/j.ajmms.20251506.62.
1. Introduction
- Pre-diabetes is an intermediate hyperglycemic state or a non-diabetic hyperglycemic state without symptoms or with minimal symptoms [1]. That is, it is a condition in which blood glucose levels are above normal but below the threshold value for a clinical diagnosis of diabetes.Prediabetes can progress to DM2 in 50% of cases within 5 years [2]. In this regard, in attempts to delay the onset of DM2, prevent or delay microvascular and macrovascular complications, increasing attention has been paid to pre-diabetes.In China, the prevalence of prediabetes among adults reaches 50%.The prevalence of IFG with age adjustment was high in low-income countries such as Nepal. A recent meta-analysis from Nepal showed a high prevalence of pre-diabetes (9.2%) based on IFG and IGT [1]. The prevalence of pre-diabetes is especially high in the urban conditions of South Asian countries, reflecting the growth of urbanization and the transition to a high-calorie diet and sedentary lifestyle [2].In Russia, the prevalence of prediabetes (NATION program) diagnosed according to HbA1c levels using ADA criteria can be 19.3%, with regional variations from 10.3% to 22% [4], and for GN levels - from 18-28.1% according to WHO criteria (and the Russian Endocrinology Association) to 54.8% according to ADA criteria [3].The prevalence of prediabetes worldwide is increasing as the prevalence of obesity increases [4].Research objective: to assess the frequency of prediabetes and type 2 diabetes mellitus occurring depending on aIGTropometric indicators.
2. Materials and Methods of Research
- To implement the goals and objectives of the dissertation research, we conducted a simultaneous epidemiological study involving men and women aged 35 to 75 living in rural areas and cities. The survey was conducted among 1,800 individuals over 40 years of age in the Markhamat district of Andijan region and 1,600 individuals over 40 years of age in the city of Andijan. The study was conducted in 3 stages. The phased approach in implementing the monitoring assumes that at the first stage, data on the main risk factors are collected using questionnaires (1st stage). Then, in the second stage, the simplest physical examinations are conducted (2nd stage), and only then is it recommended to take blood samples for biochemical studies (3rd stage). The diagnosis of prediabetes was established in accordance with the criteria proposed by the WHO and the recommendations developed by experts of the Russian Endocrinology Association (2017), EACD and ADA (2015, 2018). Pre-diabetes was defined as IFG or IGT. Hyperglycemia included a diagnosis of diabetes or prediabetes.Carbohydrate metabolism parameters were assessed based on the assessment of capillary blood glycemia levels using glycometers. The HbAls level was determined by us using a set of reagents from the company "HUMAN" with automatic determination of blood hemoglobin levels and calculation of the percentage ratio of HbAls to the total.The aIGTropometric study was conducted as follows: the height was determined in the "standing" position with an accuracy of up to 0.5 cm (without shoes), with the subject's heels, buttocks, and shoulders touching the measuring pole, and the head positioned so that the connecting line was horizontal. Body weight was measured without shoes on a standard scale with an accuracy of up to 0.1 kg. To study excess body weight (BMI) and obesity, the following were performed: the calculation of the body mass index (BMI) was carried out according to the Ketle index (BMI) - the ratio of body mass in kg to the square of the height value in meters according to the formula, the level of obesity was calculated (Table 1).
|

3. Research Results
- From the data presented in Table 2, it follows that in Marhamat district, excess body weight ranked 1st - 69 patients (37.5±5.8%), obesity 1st degree ranked 2nd - 56 individuals (30.4±6.2%), and obesity 2nd degree ranked 3rd (9.2±1.2%). In addition, in the Marhamat district, patients with excess body weight were most common in the group with IFG+ IGT - 21 observations (39.6±6.8%), IFG - 9 individuals (47.4±11.8%), and DM 2 - 19 cases (36.5±6.7%). At the same time, 3rd-degree obesity was observed in only 3 cases out of 184 observations (3.5%), while 1st and 2nd-degree obesity were observed in 56/17 (30.4/9.2%) cases, respectively. Patients with type 2 diabetes mainly had excess body weight - 19 cases (36.5±6.7%).
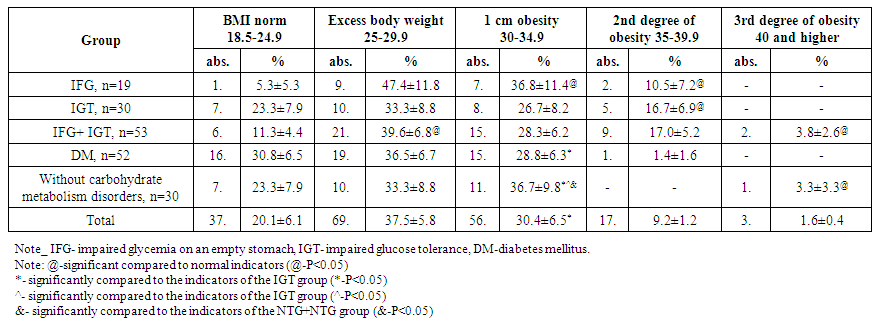 | Table 2. Body mass index by groups, Marhamat, n=184 |
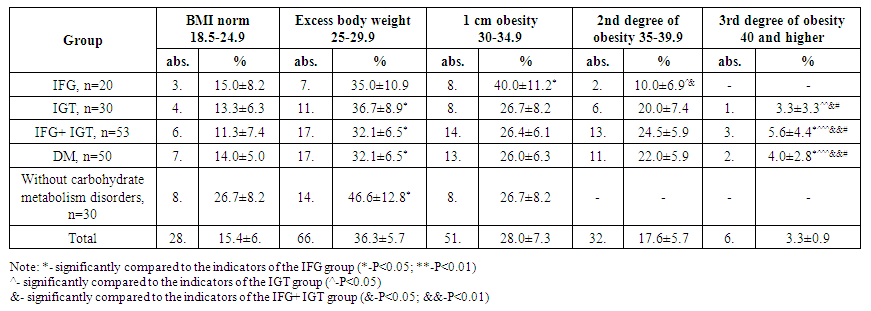 | Table 3. Body mass index by groups, Andijan city, n=182 |
|
|
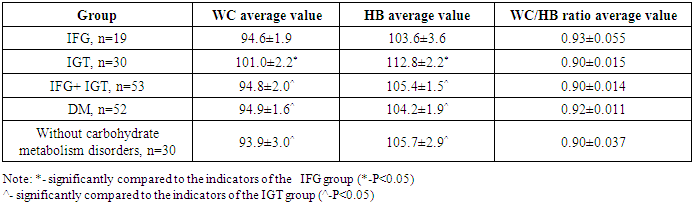
4. Conclusions
- 1. The conducted research showed that both rural (Marhamat district) and urban (Andijan city) populations of Andijan region show high prevalence of excess body weight and obesity, which corresponds to the global trend of obesity growth in low- and middle-income countries [1,2]. The identified data indicate a significant burden on alimentary-dependent diseases, including metabolic disorders.2. Among the rural population, individuals with excess body weight (BMI 25.0-29.9 kg/m2) and obesity of the 1st degree (30.0-34.9 kg/m2) predominate, while in urban sample, more severe forms of obesity (II and III degrees) are more common. This may be due to differences in the nature of nutrition, physical activity level, economic security, stress stress, and access to medical care, as indicated in studies conducted in other regions with similar demographic characteristics [3,4].3. Differences between rural and urban residents in BMI indicators, waist circumference, hip circumference, and WC/HB coefficient are statistically significant (p < 0.05), which confirms the heterogeneity of the epidemiological profile and requires the development of targeted prevention programs for obesity, differentiated by place of residence [5]. Early diagnosis of carbohydrate metabolism disorders in individuals with the abdominal type of obesity, which is more closely associated with insulin resistance, is particularly relevant [6].4. The obtained results indicate the need to strengthen sanitary and educational work among the population, as well as to implement regional pre-diabetes and type 2 diabetes screening programs. Systematic observation of a IGT topometric indicators can be an effective tool for early prevention of metabolic diseases and cardiovascular complications [7,8].