Eshankulov Galibjon Turakulovich, Kamalova Feruza Rahmatillaevna
Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan
Correspondence to: Eshankulov Galibjon Turakulovich, Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
In children of early school age and school age and the effectiveness of their optimal treatment is an urgent problem of modern medicine, because it allows determining the need for orthodontic treatment and preventive measures of the population, as well as calculating the necessary amount of orthodontic care and determining the effectiveness of treatment and preventive measures.
Keywords:
Children of early school age and school age, Anomalies and deformations of the tooth-jaw system, Orthodontic treatment and preventive measures
Cite this paper: Eshankulov Galibjon Turakulovich, Kamalova Feruza Rahmatillaevna, Assessment of the Dynamic Status of Standard and Complex Orthodontics Treatment in the Dental-Jaw System in Age-Dependent Children with Anomalies of the Dental-Jaw System, American Journal of Medicine and Medical Sciences, Vol. 15 No. 6, 2025, pp. 1908-1911. doi: 10.5923/j.ajmms.20251506.59.
1. Introduction
Currently, the prevalence of anomalies of the dento-maxillofacial system in orthodontic dentistry, according to the World Health Organization, is more than 50% (WHO, Geneva 2017). As stated in scientific research, "... The incidence of dental and jaw anomalies in children in our country is 48 - 62% is meeting Age-related prevalence of dental-jaw system anomalies in early school age is most common among children aged 3 to 6 years, and 7 to 9 years old in school age. One of the urgent problems is the early detection of anomalies of the tooth-jaw system among preschool and school-age children, study of prevalence indicators, development of effective treatment methods, and implementation.Worldwide, effective work has been carried out to develop methods for early diagnosis and complex treatment of dentofacial anomalies in preschool and school-age children, to achieve stable aesthetic results in the treatment of orthodontic patients and to reduce the number of relapses. However, the existing diagnostic methods are insufficient, which creates an urgent need for additional diagnostic and treatment methods [1,3,5,7,9,11,13,15]. In this regard, the development of diagnostic and treatment measures aimed at improving the quality of orthodontic care in preschool and school-age children is of great importance in the practice of orthodontic dentistry.
2. Results and Analysis
Thus, based on the goals and objectives of the research, the scope of the research was to study the prevalence of anomalies of the dento-maxillofacial system among preschool children in the regions of the Bukhara region, evaluate the results of the main preventive examination, and provide a comparative clinical assessment of the results obtained in them with the use of traditional and complex orthodontic treatment measures, depending on age. According to it, 1066 children underwent a full preventive dental examination (Gijduvan, Olot, Karakul, Bukhara district and Bukhara city), and 83 children with anomalies of the dento-maxillofacial system were selected for the main group. Of them, 41 were aged 3-6 years old, and 42 were aged 7-9 years old. The main group of children underwent traditional treatment, depending on age, and additional complex orthodontic treatment measures. Accordingly, in addition to traditional measures, we used Infantil Trainers T-4.K-1 in children aged 3–6, and removable orthodontic appliances that expand the anterior part of the upper and lower jaw, according to indications, in children aged 7–9. | Figure 1. Infantile trainers used to guide dental eruption and correct muscle tone in early childhood. We used infantile trainers and removable orthodontic appliances that expand the anterior part of the upper and lower jaw |
The comparison group consisted of 87 children, 48 of whom were aged 3–6 years and 39 were aged 7–9 years. Children in this group had anomalies in the maxillofacial system, and the following traditional treatment measures were performed depending on their age. In children aged 3–6 years, the procedure consisted of grinding teeth that did not have physiological caries during the period of milk teething, surgically lengthening the labial and lingual frenulum, and installing removable appliances to prevent tooth movement, and in children aged 7–9 years, the preventive method based on the Hotz method and the use of removable plate prostheses were used. The results were compared accordingly. The main methods of treatment of anomalies in the maxillofacial system are myogymnastics, various plates, and surgical methods. In some children, several of these methods may be used depending on the indications. Orthodontic appliances are divided into preventive (to prevent the eruption of certain groups of teeth, to prevent changes in the alveolar process and jaw shape due to bad habits, to correct the condition of the tongue, etc.), therapeutic appliances (intraoral or extraoral), etc. Myogymnastics is a treatment method that is very effective in early childhood (in the period of primary teeth and early molars). The effect of this method is not noticeable during the period of permanent molars. Infantil trainers are highly effective orthodontic devices that eliminate excessive pressure on the muscles, and after a certain period of use, it is easy to achieve the desired result, and it is known that their use in early childhood gives a 90% good result. Infantil T4 K1 trainers are made of soft or hard silicone, and are aimed at correcting the eruption of teeth in the jaws, improving muscle tone along with eliminating bad habits [2,4,6,8,10,12,14]. One of their main features is that they gently affect the lips, tongue and teeth, helping to keep the child's tongue and lips in the correct proportion. Based on this effect of the device, the child is forced to give up bad habits. We use trainers in this category more often in the following cases:- clenching of the teeth in the front part of the lower jaw;- the occurrence of an open bite under the influence of harmful habits;- distal occlusion, protrusion and retrusion of front teeth;The instructions given above are considered to be problems of the tooth-arch line that are identified in the early period of children's life.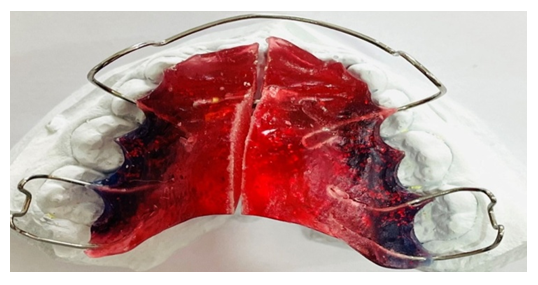 | Figure 2. Jaw expander device used to correct bite anomalies and promote proper jaw development in children |
Jaw expander devices - devices of this category are mostly used to correct tooth-jaw lines and eliminate pathological bite in children of early age at the beginning of the first and first molar teeth. It is during this period that the jaws are in active growth. And it is during this period that eliminating a pathological bite is relatively cheap, takes less time and requires less effort. Instructions for the use of plates of this type are calculated as follows:- when there is no place for permanent teeth to emerge in the jaws;- when the teeth are clenched;- in cases where certain groups of teeth are incorrectly located in the arch rows.The results recorded from the studied groups in the period to the treatment were as follows: the proportion of children with anomalies in the lateral regions of the left side compared to the right side was not found statistically significant differences for any age group, nor for the sagittal, transversal and vertical directions (p < 0.05). The proportion of lateral anomalies differed for different directions in all children. Defects in the lateral parts of the teeth were detected in the sagittal direction both on the right (20.23%), and on the left (19.85%) and more often than in the transverse direction (7.63% and 8.02%, respectively). The ratio among all examined children in the sagittal direction was statistically significantly higher than the ratios in the transversal and vertical directions (p < 0.05). The average arithmetic proportion between the left and right sides for the sagittal direction was 20.04%, and for the horizontal direction it was 7.23%. That is, it was found that there were almost 3 times more anomalies of the teeth in the sagittal direction than in the horizontal and vertical directions. In the vertical direction, the violation of occlusal contacts was detected in the area of individual teeth or groups of temporary molars, dento-alveolar elongation or shortening, and in some cases, delayed eruption of lateral permanent teeth, which led to an increase in dento-alveolar height in the area of antagonist teeth that should have erupted. The average arithmetic proportion of anomalies between the left and right sides for the vertical direction was 9.35%. Also, the violation of the contacts of the teeth with each other in the frontal area had differences in the vertical (7.78%), sagittal (7.35%) and horizontal (3.4%) directions in all children. The percentage of anomalies in the transverse direction was statistically significantly lower than in other directions (R<0.05).We also examined the vertical effects of perturbations in the frontal field in an eye-dependent manner. Thus, in the initial period of the period of exchange of teeth, children with ratio violations made up 11.4%, in the late period - 5.8%, and permanent teeth - 9.1%. Statistically significant differences were not detected, that is, the ratio of anomalies in the frontal field in the vertical direction was approximately the same in different age groups. In addition, in our study, cases of disorders in the frontal area in the sagittal direction were also studied. we learned No statistically significant differences were found between the indicators of these subgroups.We also examined the effect of age on frontal lobe disorders in the transverse direction. The percentage of children with disorders in the early period of mixed teeth was 0.8, in the period of milk bite - 2.3%, in the late period of mixed teeth - 2.5%. No statistically significant differences were found in all age groups. Thus, in the groups we studied, anomalies of the tooth-jaw line were found in 38.5%, mixed type anomalies in 18.5%, and in a separate group of teeth anomalies in 30.5%, and in occlusion in 26.5%. A detailed study of the main parameters of dental arches and occlusal relationships showed their variability over time. The dynamic state of teeth and occlusion has been shown to be susceptible to the effects of risk factors. At the same time, it can be assumed that teeth and their relationships may undergo targeted changes during periods of active growth and development under the influence of orthodontic treatment and preventive measures. The data we obtained showed a variety of dental-jaw anomalies, differences in the localization of disorders in the period of initial mixed bite, final mixed and permanent bite.
3. Conclusions
In this regard, it is advisable to record in detail the shape, size, symmetry and deviations from the occlusion of teeth in the frontal and lateral incisors in three mutually perpendicular directions during preventive examinations of children. Taking into account these features, we believe that it is necessary to analyze the effectiveness of treatment and preventive measures in children over time, during clinical observation, especially in the presence of risk factors.
References
| [1] | Abreu RR Rocha RL, Lamonier JA, Guerra AF Etiology, clinical manifestations and concurrent findings in mouth-breathing children // J. Pediatr. (Rio.). - 2008. - Vol. 84. - P. 529-535. |
| [2] | De Menezes VA Prevalence and factors related to mouth breathing in school1 children at the Santo Amaro project-Recife, // Braz. J. Otorhinolaryngol. 2006. - Vol. 72, No. 3. - P. 394-399. |
| [3] | Deb U. Care of nasal airway to prevent orthodontic problems in children / U. Deb, SN Bandyopadhyay // J. Indian Med. Assoc. 20 14. - Vol. 105, No. 11. -P. 640 - 642. |
| [4] | Dokic D., Karkinski D., Isjanovska R. et al. Measuring nasal volumes with acoustic rhinometry // Appendix. - 2010. - Vol. 31, N1. - P. 339-347. |
| [5] | Ferraz MJ, Nouer DF, Teixeira JR Cephalometric assessment of the hyoid bone, position in oral breathing children // Braz. J Otorhinolaryngol. - 2007. - Vol. 73. - No. 1. - p. 45-50. |
| [6] | Flutter J. The negative effect of mouth breathing on the body and development of the child // Int. J. Orthod. Milwaukee: - 2016. - Vol. 17. - No. 2. - P. 31-37. |
| [7] | Fricke BL, Donnelly LF, Schott SR, Poe SA, Chini BA, Amin RS Comparison of lingual tonsil size as depicted on MR imaging between children with obstructive sleep apnea despite previous tonsillectomy and adenoidectomy and normal controls. Pediatric Radiol. - 2016 Jun. - N. 36(6). - P. 518-23. |
| [8] | Fujimoto S., Yamaguchi K. Gunjigake K. Clinical estimation of mouth breathing // Am. Orthod. Dentofacial Orthop. - 2017. - Vol. 136. - #5. - P.630. |
| [9] | Giancotti A., Greco M. The use of bonded acrylic expander in patients with open-bite and oral breathing // Eur. J. Paediatr. Dent. -2008. - Vol. 9. - #4. Suppl. P. 3-8. |
| [10] | Izuka EN, Costa JR, Pereira SR Radiological evaluation of facial types in mouth breathing children: a retrospective study // Int. J. Orthod. Milwaukee. - 2016. - Vol. 19. - No. 4. - P. 13-19. |
| [11] | Izuka, EN Radiological evaluation of facial types in mouth breathing children: a retrospective study // Int. J. Orthod. Milwaukee. 2008. - Vol. 19, No. 4. - P. 13-16. |
| [12] | Torakulovich EG The Modern Concept of the Origin of the Dental Anomaly // International Journal of Integrative and Modern Medicine. - 2024. - T. 2. – no. 4. – S. 16-19. |
| [13] | Torakulovich EG Methodical Approach to the Occurrence, Early Diagnosis and Complex Treatment of Anomalies in the Gums // International Journal of Alternative and Contemporary Therapy. - 2024. - T. 2. – no. 4. – S. 23-25. |
| [14] | Torakulovich EG Analysis of the Share of Scientific Literature on the Spread and Causes of Dental Anomalies // World of Medicine: Journal of Biomedical Sciences. - 2024. - T. 1. – no. 4. – S. 40-44. |
| [15] | Eshenkulov GT Criteria for evaluation of early diagnosis of tooth-jaw system anomalies // Community Dent Health. - 2002. - T. 19. - S. 161-165. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML