Akhmedov Farkhod Khakimovich
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Akhmedov Farkhod Khakimovich, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The causes of gallbladder cancer are complex. The disease develops against the background of an inflammatory process, cholelithiasis. Risk factors such as predisposition to the development of a pathological condition play a major role. Mostly women are affected, the proportion of female patients is 3-4 times higher than that of men. The age range is 50-60 years. At the same time, the disease is often diagnosed very late due to the lack of characteristic, typical symptoms of the pathological condition.
Keywords:
Spleen, Liver, Ultrasound diagnostics, Computed tomography
Cite this paper: Akhmedov Farkhod Khakimovich, Ultrasound Diagnostics of Gallbladder Tumors, American Journal of Medicine and Medical Sciences, Vol. 15 No. 6, 2025, pp. 1697-1701. doi: 10.5923/j.ajmms.20251506.14.
1. Introduction
Gallbladder cancer is a malignant tumor that develops from the tissues of the organ. Mostly adenocarcinomas are encountered, but sometimes other histological variants of malignant tumors develop. The neoplasm develops against the background of an inflammatory, usually long-term process. Although commonly considered rare, gallbladder cancer is the most common malignant disease of the bile ducts and accounts for 80-95% [1-2]. Early diagnosis of cholelithiasis is very important, as its clinical manifestations are nonspecific and can be observed during inflammatory processes, therefore the tumor is often detected quite late, already during its spread beyond the organ. The article covers the features of the etiology and clinical course of cholelithiasis, which complicate its diagnosis and differential diagnosis [3]. As a rule, women are ill, but the disease also occurs in men, although several times less often. An overview of the possibilities and limitations of the ultrasound research method in diagnosing cholelithiasis using various ultrasound modalities is presented (V-mode, duplex scanning, three-dimensional reconstruction, endosonography, application of contrasting ultrasound agents, elastometry). The pathological condition almost does not give characteristic symptoms. It is quite difficult to determine that cancer has developed. Specialized diagnostics of the disorder is needed [4].
2. Materials and Methods
Patients undergo ultrasound and CT examination at the RSHTYOIM PF and RIO and RIATM, and morphometric results are compared.
3. Results and Discussion
The prevalence of the disease is from 2 to 8% of the total number of oncopathologies. At the same time, among gastroenterological types of cancer, gallbladder tumor is approximately in 5th place, second to stomach oncology and intestinal cancer. Determining the causes is important in the context of developing secondary prevention measures. After the treatment, in order to prevent relapses of the disorder.The causes of gallbladder cancer can be very different. As a rule, the pathogenesis of the disease is based on the following points:• inflammatory process;• formation of gallstones;• gallbladder injuries;• other volumetric processes in the organ structure;• infectious processes of a local nature.The inflammatory process in the gallbladder is called cholecystitis. The pathological condition is accompanied by painful sensations, a long, often chronic course. It occurs in patients of all ages, but is predominant in women over 50. With a significant history of inflammation, cellular transformation processes begin, which ultimately leads to low-symptomatic cancer.Gallstone disease is the result of an inflammatory process, a disorder of the processes of bile evacuation from the body. The pathological condition is accompanied by minimal symptoms. Often stones (calculi) are discovered during ultrasound, accidentally. Trauma and damage to the gallbladder can be the result of moving stones. But in some cases, trauma occurs against the background of abdominal injuries (falls, traffic accidents, etc.). A single injury is usually not enough to cause cancer, but it is possible.Volumetric processes can cause a pathological process. Thus, polyps can degenerate. They are rightly considered precancerous formations. Sometimes cysts with a solid component develop into cancer. But this is a rarer phenomenon.Finally, the influence of infectious processes is possible. Cancer processes develop against the background of salmonellosis, shigellosis and some other septic processes (Figure 1-2.)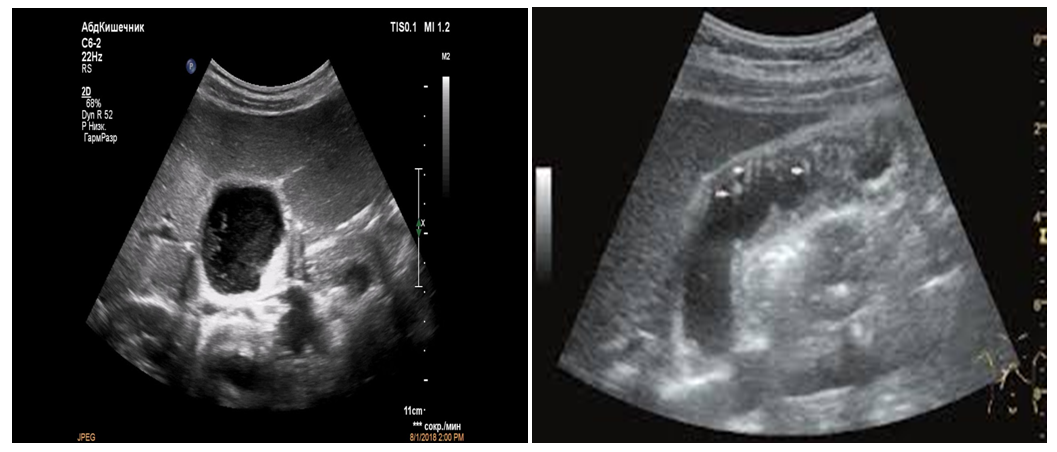 | Figure 1-2. Echogenic image of gallbladder tumour |
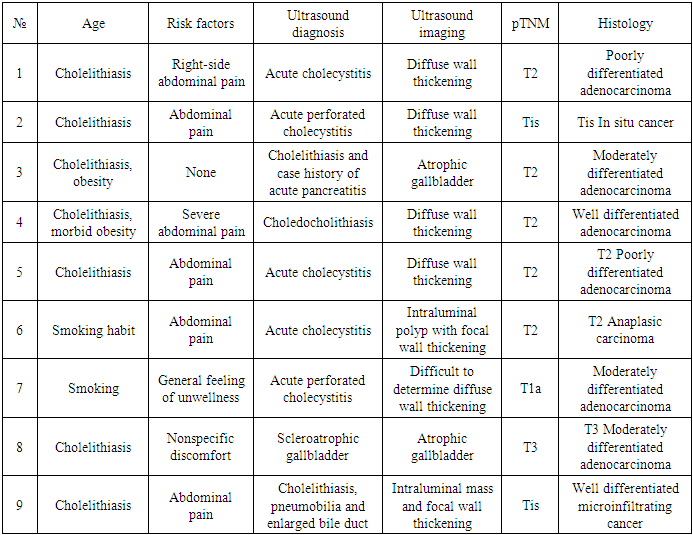
Gallbladder oncology develops against the background of a whole complex of reasons. But with competent medical care they can be corrected and eliminated.Increased risk factors play no less a role. If there is a direct cause, they stimulate the development of the pathological process, increasing the likelihood of the disorder. Risk factors include:• smoking, nicotine use, and the longer the addiction, the higher the likelihood of a pathological process;• alcohol dependence, alcohol abuse, the likelihood of the disease also depends on the length of the “friendship” with alcohol;• obesity, increased body weight in the patient, it is important to correct the weight;• improper, poor quality nutrition with an excess of fatty, fried foods and other nutrients that are unnatural for the human body;• age 50+, in the overwhelming majority of cases, gallbladder cancer develops after 50 years, with very rare exceptions;• female gender, it is mainly women who get sick;• disturbances of normal hormonal levels;• diseases of the digestive tract, various structures of the gastrointestinal tract.Also regular exposure of the human body to carcinogens. As part of professional activity or under other circumstances [5-6].Symptoms of gallbladder cancer are non-specific. The disorder is accompanied by various disorders, but they are not so characteristic to determine cancer and make an unambiguous diagnosis. Sometimes there are no symptoms of the pathological process at all. This significantly complicates the process of early diagnosis.Some of the symptoms worth paying attention to include:• pain, discomfort are minor, a person usually does not pay attention to them, the same symptom is observed in chronic cholecystitis, in advanced stages of the pathological condition the pain becomes stronger;• a feeling of pressure in the right side, distension under the ribs;• nausea, vomiting, including regardless of food intake;• disorders of normal digestion due to impaired bile flow and increasing phenomena of enzymatic deficiency;• weakness.As the pathological process progresses, dyspeptic symptoms develop. The patient experiences bowel movements. Both diarrhea and constipation are possible. Often, alternation of one and the other is observed. The stool changes its color. When the bile ducts are blocked by a tumor, mechanical jaundice develops [7]. The sclera of the eyes turns yellow, the skin changes its color. When the tumor disintegrates, symptoms of general exhaustion of the body, poisoning by the products of tumor cell death develop. Possible manifestations include drowsiness, weakness, weight loss, and appetite disorders. An increase in body temperature to subfebrile values is possible. This is a typical symptom of cancer. According to our estimates, the clinical picture remains insufficiently clear until the terminal stage of the pathological process. And even then, the patient does not always suspect that he has cancer (Table 1).Table 1. The clinical data, results of ultrasound scanning, pT, postcholecystectomy, and tumor type
 |
| |
|
Ultrasound diagnostics of gallbladder cancer. The most common variant 40-65% is an echogenic formation within the gallbladder fossa with concomitant cholelithiasis. Gallbladder cancer can develop against the background of constant irritation of the gallbladder wall by gallstones. The formation can spread beyond the lumen of the bladder to the liver. Less often, cancer looks like a focal or diffuse thickening of the gallbladder wall 15-20%. Combined changes can be obstruction of the bile duct, metastases in the liver and peripancreatic lymphadenopathy. Gallbladder cancer is the fifth most common among all tumors of the gastrointestinal tract and is more common in women than in men. Cancer (carcinoma) of the gallbladder can be divided into 4 groups, 1) infiltrative, 2) endophytic, 3) exophytic, 4) mixed.CT. In cases with strong suspicion of gallbladder cancer or biliary tract disease, arterial phase (at 20 to 30 seconds) and venous phase (50 to 60 seconds) can be acquired. When there is an incidental finding of gallbladder cancer and no suspicion of biliary tract cancer, only venous phase is required [8-9].In plain CT scan, gallbladder cancer is typically hypodense. It shows irregular, peripheral enhancement on arterial phase.Typically gallbladder adenocarcinomas appear as large heterogeneous masses, which may have engulfed gallstones or areas of necrosis. Patchy moderate contrast enhancement is usually seen.Features of advanced disease include:• intrahepatic biliary dilatation• invasion of adjacent structures• lymphadenopathy• peritoneal carcinomatosis• hepatic and other distant metastasesMRI. Dynamic MRI is considered useful and reliable in staging advanced gallbladder carcinoma. MRI combined with MRCP is sensitive in detecting obstructive jaundice, liver invasion, and hepatic and lymph nodal metastasis. It may be more difficult to delineate any invasion into the duodenum or to detect omental metastasis by MRI. Reported sensitivity rates for direct hepatic invasion and lymph node invasion on MRI can be as high as 100% and 92% respectively.The infiltrative variant of tumor development leads to the growth of the thickness of the gallbladder wall and causes its uneven thickening. The tumor can be echographically increased, average, decreased or mixed echogenicity, heterogeneous structure.The endophytic variant of gallbladder tumor is located predominantly in the cavity of the latter. The tumor structure is most often heterogeneous, echogenicity is usually increased. Exophytic variant of the tumor, also originates from the wall of the gallbladder, has a vector of spread directed outward, and grows into surrounding tissues and organs. Echogenicity is increased, echostructure is heterogeneous [10].The mixed variant of tumor growth includes the features of the previous ones. One of the tumor variants described above, in the gallbladder there may be stones of various sizes, with an acoustic shadow, bile clots and directly in the thickness of the tumor (Figure 3).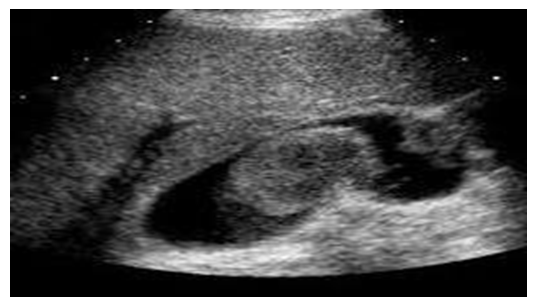 | Figure 3. Echogenic image of gallbladder tumour |
The study lists the main events in the lives of 157 patients who underwent cholecystectomy before and after the operation. Cholelithiasis occurs mainly at the age of 51-60 and 61-70 years, and most of these patients are women. Changes in the common bile ducts and intrahepatic bile ducts depending on age were determined by ultrasound examination of 157 patients with acute cholelithiasis before laparoscopic and traditional cholecystectomy. Of the 123 patients who underwent laparoscopic cholecystectomy, 21 were men and 102 were women. Of these, before the operation, the common bile duct was dilated in 27 patients, intrahepatic bile ducts - in 94. Among the 34 patients who underwent traditional cholecystectomy, 10 were men and 24 were women. Of these, before the operation, the common bile duct was dilated in 23 cases, the intrahepatic bile ducts were dilated in 23 cases. In ultrasound diagnostics of extrahepatic biliary tract pathology, it has false positive results in 4.9% of cases. The diagnostic accuracy of ultrasound in detecting gallstones is 95-99%, and visualization of common bile duct stones is successful only in 29.0-89.6% of cases. During laparoscopic and traditional cholecystectomy of ducts in individuals aged 51-70 years, dilation of the bile ducts was observed: in 8 women and 4 men, the common bile duct was dilated, 34-35 common bile ducts, and intrahepatic bile ducts were dilated in 5 women and 2 men. After traditional cholecystectomy, the common bile duct was dilated in 13 women and 9 men, the intrahepatic bile ducts in 9 cases in men and 13 cases in women did not decrease even after the operation. As a result of a comprehensive study of gallbladder materials in 157 patients with acute and chronic cholecystitis, who were examined in the biopsy and diagnostic department of the Bureau of Pathological Anatomy of the Bukhara region, 4 different types of chronic cholecystitis were identified [11-12]. As a result of studying the histological materials prepared from the gallbladder wall, pathomorphological changes in the form of pathological hyperplasia and metaplasia were revealed. Single cases were examined by histochemical methods. The results were as follows: 80 interstitial-proliferative chronic cholecystitis, 3 of them had dysregenerative changes that led to tumors; 1 of 34 chronic cholecystitis with interstitial fibrosis had a tumor-forming condition; 2 of 23 cases of interstitial myxomatosis and mucinous chronic cholecystitis were found to have tumor dysregenerative changes; In 3 of 20 cases of chronic cholecystitis with adenomyomatosis and polypous hyperplasia, tumor dysregenerative changes were detected. Dysregenerative changes leading to tumor were detected in 9 cases out of 157, which is 5.7%.
4. Conclusions
1. Ultrasound diagnostic method: obtaining detailed information about pancreatic neoplasms, clearly describing their location, nature of growth, visualizing altered lymph nodes.2. It should be noted that the accuracy of the patient's examination results directly depends on the level of the ultrasound scanner used, the scanner settings, the level of specialist training, and compliance with the examination methodology.3. Ultrasound diagnostics, including in relation to pancreatic pathology, is a rapidly developing area of medicine, which is developing in terms of innovations - elastography (compression, cutting wave), the search for new contrast agents, minimally invasive diagnostics and therapeutic manipulations, as well as already developed basic diagnostic methods and directions.
References
| [1] | Kaprin A.D., Starinskiy V.V., Petrova G.V., The State of Oncological Care for the Population of Russia in 2012. М.; 2013. 232 с. |
| [2] | National cancer registry (USA). 2012. |
| [3] | Kloppel G., Solcia E., Longnecker D.S., Capella C., Sobin L.H. Histological typing of tumours of the exocrine pancreas: WHO International Histological Classification of Tumours. 2nd ed. Berlin: Springer-Verlag; 1996. 68 р. |
| [4] | Solcia E., Kloppel G., Sobin L. WHO: Histological typing of endocrine tumours. 2nd ed. Berlin: Springer; 2000. 160 p. |
| [5] | Maev I.V., Kucheryavыy Yu.A. Pancreatic diseases. М.; 2009. 736 c. |
| [6] | Lv P., Mahyoub R., Lin X., Chen K., Chai W., Xie J. Differentiating pancreatic ductal adenocarcinoma from pancreatic serous cystadenoma, mucinous cystadenoma, and a pseudocyst with detailed analysis of cystic features on CT scans: a preliminary study. Korean J. Radiol. 2011; 12 (2): 187-95. |
| [7] | Galvin A., Sutherland T., Little A.F. CT characterisation of pancreatic neoplasms: a pictorial essay. Insights Imag. 2011; 2 (4): 379-88. |
| [8] | Lyadov V.K., Ler Y.-M., Andren-Sandberg O. Prognostic factors for resectable pancreatic cancer. М.; 2010. |
| [9] | Akhmedov F.X. Ultrasound Examination in Liver Cirrhosis Journal of Interdisciplinary Science 2024; 2 (4): 110-116. |
| [10] | Akhmedov F.X. Ultrasound Diagnostics for Liver Cirrhosis Journal of Interdisciplinary Science 2024; 1 (2): 98-110. |
| [11] | Akhmedov F.X. Ultrasound diagnostics for splenomegaly scientific-practical conference "science and innovation" Volume 1, No. 1. (5.05.2024) P: 67-68. |
| [12] | Carmen Zevallos Maldonadoa, Maria Jose Ruiz Lopez, Francisco Miguel Gonzalez Valverde and others. Ultrasound Findings Associated to Gallbladder Carcinoma Hallazgos ecográficos asociados al cáncer de vesícula biliar Vol. 92. Issue 5. Pages 348-355. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML