-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(6): 2084-2088
doi:10.5923/j.ajmms.20251506.101
Received: Jun. 8, 2025; Accepted: Jun. 25, 2025; Published: Jun. 28, 2025

Specific Features of the Newborn Hearing Screening Monitoring System in Uzbekistan During Its Implementation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLF. I. Inoyatova, V. I. Primako, N. Sh. Nadjimutdinova, A. A. Abdukayumov, M. U. Mahmudov
Republican Specialized Scientific and Practical Medical Center of Pediatrics, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study was to evaluate the efficiency of the monitoring system for universal audiologic screening of newborns. Background. According to the World Health Organization “...there is a high prevalence of congenital hearing loss - from 0.8 to 15.5 per 1,000 children, with a population average of 2-4 per 1,000 newborns, and in developed countries the prevalence of bilateral hearing loss is 1.33 per 1,000 births”. It is crucial to establish an efficient monitoring system - continuous collection, transmission, quality control and analysis of audiological screening data for the successful implementation of the screening program. Material and methods. The material of the study consisted of data for the years 2023-2024. The study included newborns from 189 maternity institutions in Uzbekistan, and the re-screening was conducted in 12 regional children's medical centers, with subsequent referral to the Republican Specialized Scientific and Practical Medical Center of Pediatrics for the final diagnosis, determining the form and degree of hearing loss and the choice of auditory correction. Monitoring was coordinated through technical management in the form of implementation of a hearing screening tracking center system in conjunction with audiological screening. Results. In 2024 (the second year of implementation), a total of 474,888 newborns were screened in 183 maternity complexes. Over the two years, the average screening error rate was 14.1% and screening coverage amounted to 82.6%. There were 1372 (0.33%) children verified as hearing impaired, and the prevalence of hearing impairment was 3.3 per 1000 newborns. This system allowed to reduce the number of open statuses by 7.8 times and to prevent the child from entering the 2nd stage of screening by closing his status in 86.7% of cases. Conclusion. This monitoring allows to promptly identify newborns who have not been screened or need to be re-screened, and to organize timely follow-up and care for them.
Keywords: Hearing pathology, Congenital hearing loss, Newborn, Screening
Cite this paper: F. I. Inoyatova, V. I. Primako, N. Sh. Nadjimutdinova, A. A. Abdukayumov, M. U. Mahmudov, Specific Features of the Newborn Hearing Screening Monitoring System in Uzbekistan During Its Implementation, American Journal of Medicine and Medical Sciences, Vol. 15 No. 6, 2025, pp. 2084-2088. doi: 10.5923/j.ajmms.20251506.101.
Article Outline
1. Introduction
- According to the World Health Organization “...there is a high prevalence of congenital hearing loss - from 0.8 to 15.5 per 1,000 children, with a population average of 2-4 per 1,000 newborns, and in developed countries the prevalence of bilateral hearing loss is 1.33 per 1,000 births” [1]. Hearing pathology is detected by parents at the age of 2-3 years, when parents notice the child's lack of speech and response to speech sounds. However, this age is considered late, and therapeutic and rehabilitative interventions for hearing and speech development are delayed [2].In March 2021, the WHO released the first World Hearing Report, which summarized epidemiological and financial data on hearing loss worldwide and proposed cost- efficient solutions to achieve an “integrated people-centered approach” (IPC-EHC) [3].As early as 1995, a WHO resolution was adopted calling on Member States to develop national plans for the prevention and control of the main causes of avoidable hearing loss and for the early detection of hearing impairment in infants, young children and children. However, in 2012, only 32 countries reported implementing such policies, and WHO regretted the lack of epidemiological and other data related to hearing and hearing care [4,3]. The goal of newborn screening of congenital hearing loss is to detect hearing loss in asymptomatic children as early as possible, followed by treatment that can prevent further progression or efficient early habilitation [5]. Existing Hearing Screening Programs in different states vary widely in quality, data collection, and availability of services for children with hearing loss. the World Hearing Report 2021 calls for a 20% increase in efficient hearing screening coverage by 2030 [4].The Republic of Kazakhstan has developed “Rules for organizing the screening of article 5 of the Law of the Republic of Kazakhstan dated by July 11, 2002” On social and medical-pedagogical correctional support for children with disabilities". Universal audiological screening (UAS) in the Republic of Kazakhstan began to be carried out in 2010, when on September 9, 2010 Order No. 704 “On Approval of the Rules of Organization of Screening” was issued. Throughout the whole period since 2010 in Kazakhstan universal neonatal audiological screening is carried out, the program of which includes 3 stages. However, according to Medeulova A. et al. (2016), the implementation of UAS proved to be a complex process and UAS itself was not successful as there was no centralized regulation of the process [6-8]. The UAS program for newborns and children of the first year of life has been implemented in the Russian Federation since 2008 [Letter of the Ministry of Health and Social Development of Russia No. 2383-RH dated 01.04.2008]. UAS in Russia is a 2-stage program [9].In Germany, universal hearing screening has been available since 2009, although the first attempts were initiated in the late 1990s through local screening programs in selected regions of Germany - Hesse, Hamburg, Berlin/Branderburg, Mecklenburg-Western Pomerania, Saarland, Bavaria. In 1999, Prof. K. Neumann organized a newborn hearing screening project in the state of Hesse. Under her guidance, the most suitable program was created, which was then implemented throughout Germany, including not only the identification of hearing impairments, but also their therapy and pedagogical assistance. Only after the introduction of universal screening for newborns in the state of Hesse and its quality control, it was possible for the first time in Germany to demonstrate that the start of therapy for hearing impairments was possible on average as early as three and a half months, and further optimization of this indicator was not excluded [10].The American Academy of Pediatrics (AAP) recommends hearing screening at ages 4, 5, and 6 years, as well as ages 8, 10, 12, 15, and 18 years, regardless of the presence or absence of risk factors for hearing loss [11].The experience of various countries in early identification and treatment of hearing impairment in children demonstrates that the long-term success of such programs requires certain additional measures, including priority support from the state and the existence of a legislative framework in this area. The most acceptable and consistent with the Wilson & Jungner screening principles is the program proposed by Katrin Neumann, which was implemented in Germany in the state of Hesse [10].it is crucial to establish an efficient monitoring system for the successful implementation of the screening program - continuous collection, transmission, quality control and analysis of audiological screening data. The monitoring provides tracking of each child through all stages of the hearing evaluation, ensuring that no newborn with potential hearing loss is lost from the doctors' sight.The aim of the study was to evaluate the efficiency of the monitoring system for universal audiologic screening of newborns.
2. Material and Methods
- The material of the study consisted of data for the years 2023-2024. The study included newborns from 189 maternity institutions in Uzbekistan. The re-screening was conducted in 12 regional children's medical centers, with subsequent referral to the Republican Specialized Scientific and Practical Medical Center of Pediatrics for the final diagnosis, determining the form and degree of hearing loss and the choice of auditory correction. Monitoring was coordinated through technical management in the form of implementation of a hearing screening tracking center system in conjunction with audiological screening. A distinctive feature was that in all periods there was centralized management and coordination from the head office (RSSPMCP – a clinic performing cochlear implantation operations), i.e. a government agency interested in the timely, early and complete identification of children with hearing impairments. Children with hearing impairment received specialized care from audiologists at 12 regional children's medical centers, as well as ENT doctors at these centers.After the screening at the first stage (at the maternity hospital), the results of each newborn are entered into an electronic database. Daily data transmission is provided: audiological screening results from maternity hospitals are manually sent online to the central monitoring information system (once a day at the same time). For this purpose, the screening devices are equipped with a wireless data transmission module that directly sends the results to the State Server Base (IT-MED SSB) from where the data are used only by the specialists of the RSSPMCP. Each child has a unique identifier (ID - number). The audio screening system is integrated with the state electronic newborn registration system: when entering data, it is possible to scan the QR code of the child's birth certificate to automatically register his or her demographic data in the Q-screen audiologic screening machine. These data can be used by audiologists to manage further stages of children with hearing loss. It allows each patient to be identified and eliminates duplicate records. At the level of a regional surdology office, when conducting the second stage of the examination, the results are also entered into the same database of the State server and become available for analysis in the monitoring center of the RSSPMCP. An information system which allows tracing the complete path of a patient from birth to surgery is created.The role of the monitoring coordination center is performed by RSSPMCP. Specialists of the center (coordinators and IT-administrator of the system) carry out daily control of incoming data. Their tasks include: checking the completeness of coverage (reconciling the number of births and the number of screened children in each region), identifying cases where a child has not been screened or has received a positive result without further confirmation in the second stage, and informing the responsible persons at the local level. The Monitoring Center generates lists of children requiring attention (e.g., those who did not pass the retest on time) and sends these lists to the regional centers to arrange for inviting families to be examined. On a monthly basis, the central level prepares an analytical report with the main indicators for the Republic and for each region, which is sent to the Ministry of Health and relevant specialists.
3. Results
- In 2023 (the first year of universal hearing screening implementation), a total of 155,124 children out of 277,007 newborns were screened in 98 maternity centers. Screening coverage amounted to 56.0%. In 2024 (the second year of implementation), a total of 474,888 out of 574925 newborns were screened in 183 maternity facilities. Screening coverage amounted to 82.6%. The data collection allowed monitoring the quality control of hearing screening at the local level, tracking screening errors such as: - manual entry of the newborn's data; - conducting studies on only one ear; - identification of “incomplete” hearing tests (open statuses) when tests were interrupted; - identification of missing screening data (Figures 1, 2).
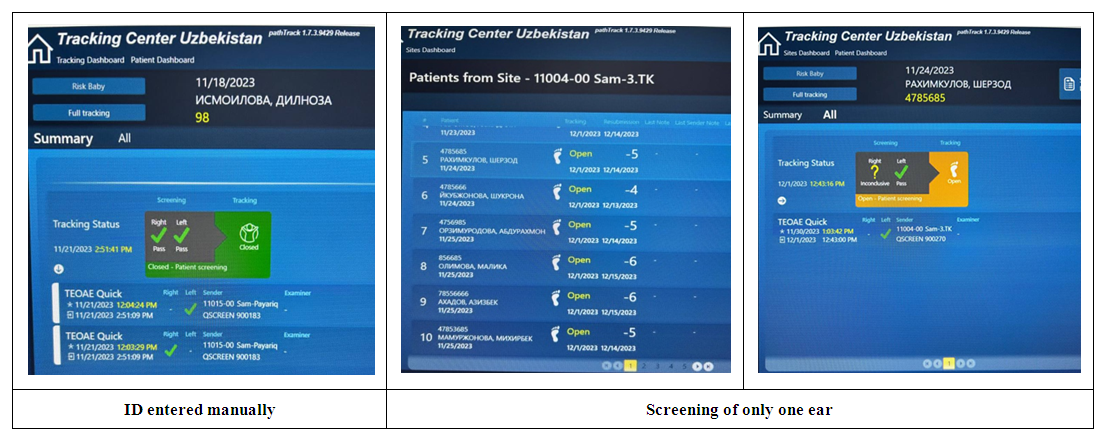 | Figure 1. Cases of open statuses detected during hearing screening monitoring |
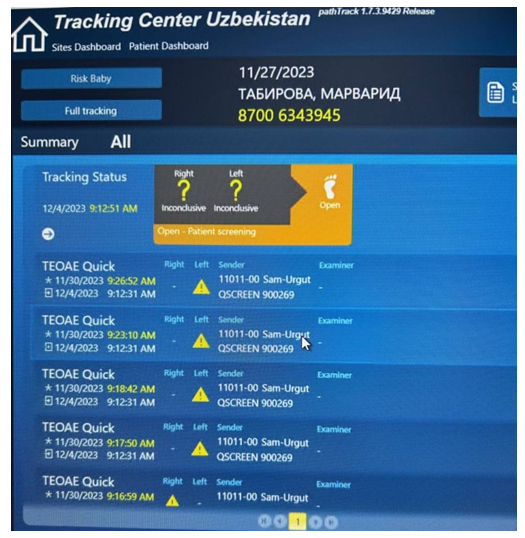 | Figure 2. Cases of open statuses detected during hearing screening monitoring: Incompleteness of the research |
4. Discussion
- A monitoring system for regions with a large number of births, maternity facilities and large distances between hearing diagnostic centers and maternity facilities requires the implementation of a tracking system with online monitoring capabilities, a unified system for conducting hearing screening on identical devices with modems for transmitting data via a cellular telephone system. In addition, the screening process was monitored by five tracking specialists who were assigned to individual regions. Overall supervision was performed by an IT specialist who monitored the operation of the entire screening and the operation of the devices, in particular: their breakdowns, the uninterrupted functioning of the modem systems with cellular telephony online. Such a system reduced the number of open statuses from 32678 (in the first year of implementation) to 4167 (in the second year of implementation) and thus prevented a child from reaching Stage 2 screening by closing their status in 86.7% of cases. Also, our system allowed to avoid loss of patients at the stage of rescreening and extended audiologic examination, as these examinations were carried out simultaneously.
5. Conclusions
- Our monitoring system allows to promptly identify newborns who have not been screened or need to be re-screened, and to organize timely follow-up care and assistance for them.Organization of monitoring of newborns universal audiological screening based on an adapted program has demonstrated its efficiency. Their implementation allows children's hearing loss to be detected at the earliest stages of life and rehabilitation measures to be taken immediately. For the health system, it means rationalizing the use of resources, reducing the burden on specialized institutions and improving integral health indicators for the child population. For the children themselves and their families, it is a chance for a full life free from hearing loss and the assurance that their health is being monitored from the first days of their lives.
Conflict of Interests’ Statement
- The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.
ACKNOWLEDEGMENTS
- The authors express their gratitude to the management of the multidisciplinary clinic of Republican Specialized Scientific and Practical Medical Center of Pediatrics for the material provided for our study.
Ethical Approval and Consent to Participate
- The Research Ethics Board of our institution does not require review or approval of case reports. Our research was carried out in accordance with the World Medical Association Code of Ethics (Declaration of Helsinki).
Source of Funding
- Each of the authors has reviewed and approved this manuscript. None of the authors has a conflict of interest, financial or otherwise. This manuscript is original, no part of it has been previously published and is not being considered for publication elsewhere. The corresponding author agrees to accept full responsibility for authorship at the submission and review stages of the manuscript.