-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(6): 1670-1674
doi:10.5923/j.ajmms.20251506.08
Received: May 7, 2025; Accepted: May 29, 2025; Published: Jun. 5, 2025

Detection of Carriers of Antibodies to Staphylococcal Infection Among the Population Donating Blood at the Republican Blood Transfusion Centre
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLYulduz Saburova1, A’lonur Saidov2, Shokhista Bobojonova1, Shakhnoza Sokhibova1, Roshona Tojiyeva1, Ubaydullo Patkhullayev1, Kumush Alikulova1, Dilnoza Mirkhamidova1
1Tashkent State Medical University, Tashkent, Uzbekistan
2DSc., Professor, Republican Blood Transfusion Center, Tashkent, Uzbekistan
Correspondence to: Yulduz Saburova, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article presents the results of research work aimed at identifying the carriage of antibodies to Staphylococcus aureus infection among the population of the Republic of Uzbekistan, in the conditions of the Republican Blood Transfusion Centre. The conclusions drawn from the results of this research work are useful for understanding the prevalence of staphylococcal infection, its carrier with the presence of antibodies to staphylococcus aureus in the blood. Among non-reimbursed donors, this study was conducted for the first time. Determination of antibodies to staphylococcal infection in blood serum is done by determining the content of anti-alphastaphylolysin, which is the leading factor of staphylococcal pathogenicity.
Keywords: Staphylococcal bacteria carrying, S. aureus., Antibody titer for staphylococcus, Staphylococcus transmission pathways, Types of staphylocococci
Cite this paper: Yulduz Saburova, A’lonur Saidov, Shokhista Bobojonova, Shakhnoza Sokhibova, Roshona Tojiyeva, Ubaydullo Patkhullayev, Kumush Alikulova, Dilnoza Mirkhamidova, Detection of Carriers of Antibodies to Staphylococcal Infection Among the Population Donating Blood at the Republican Blood Transfusion Centre, American Journal of Medicine and Medical Sciences, Vol. 15 No. 6, 2025, pp. 1670-1674. doi: 10.5923/j.ajmms.20251506.08.
1. Introduction
- The urgency of the problem of infections caused by Gram-positive microorganisms is increasing worldwide [1. 238], as indicated by research works in this area by domestic and foreign scientists, Staphylococcus aureus, relative to other genera belonging to the family Micrococcaceae, are the causative agents of the majority of out-of-hospital and nosocomial bacteraemias, pneumonias, infections of skin and soft tissues, organs, bones and joints [6. 63–67], and today it is more harmful to the health of patients and affects the process of treatment and course of the disease within the walls of hospitals.As for staphylococci themselves, it should be noted that the Firmicutes (from Latin firmus - strong, cutes - skin) department includes prokaryotic microorganisms with Gram-positive type of cell wall, this department is represented by bacteria of various properties, forming a group of aerobic Gram-positive cocci. Of particular medical importance are the cocci of the families Micrococcaceae and Streptococcaceae. Representatives of the Micrococcaceae family, capable of causing disease in humans, belong to the genera Staphylococcus, Micrococcus and Stomatococcus [17]. Staphylococci are gram-positive, geometrically regular spherical bacteria 0.5-1.5 µm in diameter. These bacteria divide in several planes, producing a characteristic bunch-of-grapes shape. Peptidoglycan and teichoic or glyceric acids are the basis for the structure of the cell wall of pathogens. The cell wall of S. aureus also includes protein A, which reacts with Fc-fragments of human IgG [3. 472], which gives us the detection of IgG in ELISA study, which makes us understand the chronic course of diseases caused by Staphylococcus aureus and the carrier of the infection itself in the body for life.A part of Staphylococcus aureus surrounding a human or animal is not capable of causing disease, i.e. non-pathogenic [10. 89], and makes it possible to refer them to the conditionally pathogenic microflora of the organism. Disease-causing species possess a certain set of pathogenicity factors that allow bacteria to successfully penetrate into the body and exist in it for a long time, avoiding the host's immune response [8. W52–57]. Among non-spore-forming bacteria, staphylococci are the most resistant to external factors. They are able to tolerate drying and remain viable and virulent up to several months in dry dust, being a source of dust infection. Direct sunlight has a pernicious effect only after several hours of direct exposure, diffused light acts rather weakly [3. 472].In 20-30% of healthy people, Staphylococcus aureus is found in the nasal passages [15. 22], without causing disease, but turning these people into carriers. Pathways of transmission are diverse, the most common being airborne transmission, progressing to household contact via household items, hands, especially among health care workers [14. 437-44]. The alimentary route of infection is less frequently observed, but still occurs - the susceptibility to staphylococcal infection in this case is quite high. From 90 to 100% of people who have consumed contaminated products become ill. The disease is registered throughout the year, more often in the warm season [9. 21–22].In terms of pathogenesis and clinical picture, staphylococci have a number of distinctive features. Like all Gram-positive opportunistic microorganisms, they are capable of causing opportunistic infection. The clinic of purulent-inflammatory processes is characterised by different localisation and varying degrees of severity, from local to severe generalised infections [7. 21–25]. The most formidable purulent-inflammatory process is sepsis, in which a purulent focus is observed, from which the pathogen enters the blood and spreads throughout the body to any organ, affecting the reticuloendothelial system, releasing toxins and allergens. The formation of purulent foci in various organs and tissues, leads to septicopaemia [18. 603–661]. In this regard, Staphylococcus aureus has been recognised as having a variety of forms of infection:- diseases of the skin and subcutaneous tissue [13. 102–106]; - respiratory diseases [12. 134]; - diseases of the nervous system and sensory organs [11. 51–55]; - diseases of the digestive organs [1. 238]; - diseases of the musculoskeletal and connective system [20. 39–43];- diseases of the circulatory system [4. 675–684]; - diseases of the genitourinary organs [16. 46-50].Post-infection immunity - cellular-humoral, unstable, unstressed, narrowly specific. By orientation - antitoxic, antienzyme, antibacterial. Due to contact with the pathogen, most adults develop antibodies to Staphylococcus aureus and its toxins [2. 79–90].For the treatment and therapy of chronic staphylococcal infections and its prevention in pregnant women, newborns and immunodeficient patients it is recommended to use purified, adsorbed with aluminium hydroxide staphylococcal anatoxin [19. 3279]. But in cases of severe intoxication and sepsis, the use of human anti-staphylococcal immunoglobulin from the blood of donors immunised with staphylococcal anatoxin is indicated [6. 1797-806].Immune sera and immunoglobulins are preparations containing ready-made specific antibodies (immunoglobulins), the introduction of which into the body leads to the immediate acquisition of passive humoral immunity capable of protecting the body from intoxication or infection. They are intended to produce passive antitoxic, antibacterial or antiviral immunity in a person in need of protection against infection or other potentially dangerous substances with antigenic properties. They are used as means of seroprophylaxis and serotherapy. Therapeutic agents are used when there is reason to believe that the body is unable to provide its own defence.Human immunoglobulins are prepared from donor or placental blood, the concentration of antibodies in them is low. To obtain preparations of immunoglobulins with increased antibody content, preliminary selection of raw materials - blood sera containing the appropriate antibodies - is performed, and sera of re-vaccinated patients or immunised donors are used. Such preparations are labelled separately and used for special risk groups: newborns, critically ill and others. Current methods of globulin preparation completely exclude the possibility of the presence of viruses, including HIV (human immunodeficiency virus), but they may contain reactogenic proteins aggregated during preparation. [2]1
2. Materials and Methods
- For this study, serum of 500 donors who voluntarily donated blood and 50 donors immunised with staphylococcal anatoxin from January 2024 to January 2025 at the Republican Blood Transfusion Centre of the Ministry of Health of the Republic of Uzbekistan was isolated.The serum was tested for the presence of antibody titres by determining the level of anti-alphastaphylolysin in serum preparations of human and animal blood using a commercially available kit ‘Staphylococcal diagnostic toxin’ and ‘Staphylococcal anatoxin purified adsorbed’ (manufacturer: N.F. Gamaleya NICEM of the Ministry of Health of Russia, Moscow) with instructions from the manufacturer. Ministry of Health of Russia, Moscow) with instructions from the manufacturer. The drug has haemolytic effect, causing haemolysis of rabbit erythrocytes in vitro. Before the experiment it is recommended to determine Lh toxin (limit of haemolytic toxin), the detection limit of which is from 0.1 to 0.2 ml. According to the control results, the Lh toxin was 0.14. When calculating the activity of the test drug, appropriate recalculation coefficients are entered for each specific experiment according to the formula:
 K-coefficient of recalculation; a-number of international units according to accepted standards in the control tube in which haemolysis of 50% of erythrocytes was registered (extinction index 0.35⁺_0.05). A comparative analysis was performed between a control group consisting of donors immunised with anti-staphylococcal anatoxin and donors who donated blood. Detected titres were labelled from 1 to 5 International Units.
K-coefficient of recalculation; a-number of international units according to accepted standards in the control tube in which haemolysis of 50% of erythrocytes was registered (extinction index 0.35⁺_0.05). A comparative analysis was performed between a control group consisting of donors immunised with anti-staphylococcal anatoxin and donors who donated blood. Detected titres were labelled from 1 to 5 International Units.3. Results
- Staphylococcus aureus antibody titre detection assay is one of the serological methods based on direct haemagglutination reaction and indicates the presence of passive immunity against Staphylococcus aureus infection. According to the results obtained from 500 donors who donated blood, 78% of them were men and 22% women. The donors were in the age group of 18 to 60 years. In our study, the overall detection rate of titres was 18.7%, of which the antistaphylococcal titres were 1IU*2-20%, 2IU-10%, 3IU-12%, 4IU-23%, 5IU-35%, and the distribution by blood groups was as follows O(I)-37%, A(I I I)- 29%, B(I I I I)-27%, AB(IV)-7% (Figure 1).
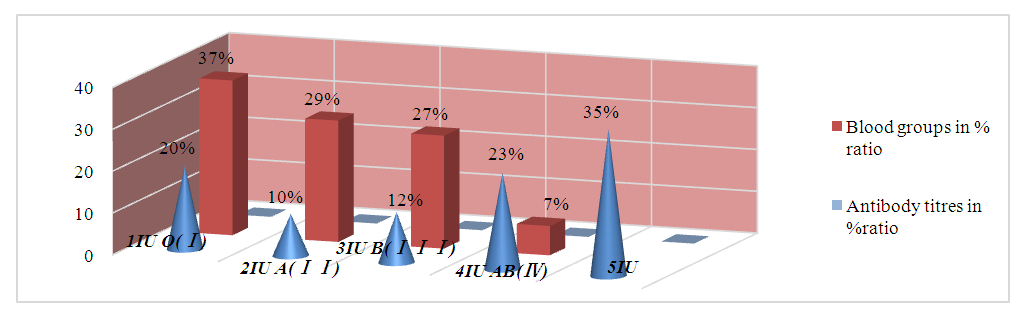 | Figure 1. Total percentage detection of antibodies in correlation of titre and blood group data |
|
4. Discussion
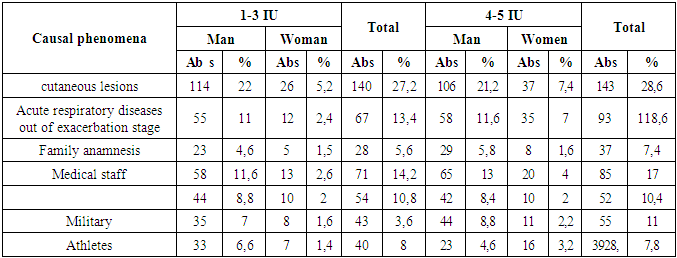
- In our study we have analysed the frequency of staphylococcal infection and carriage of its antibodies among donors of Republican Blood Transfusion Centre. This finding is useful in understanding the prevalence of staphylococcal infection among donors and the possibility of providing raw material on a continuous basis for production of anti-staphylococcal plasma for therapeutic purposes. This is the first time this study has been conducted among donors.Staphylococci are representatives of the normal microflora of humans and animals. They densely colonise various biotopes of the human body: skin, nasal mucosa, pharynx, oral cavity. The source of infection is patients with any clinical form of staphylococcal infection, healthy carriers.The practical significance of this work is to produce sufficient quantities of necessary raw materials in the form of immune plasma for the production of staphylococcal immunoglobulin, necessary for the population of the republic. The task of this work is: to develop a questionnaire to identify people with staphylococcal infection among blood donors. In addition, determination of antibody titres to staphylococcal infection among different population groups, study of blood parameters of immune donors in dynamics, comparative study of antibody titres in plasma of ‘active’ and ‘passive’ immune donors, as well as development of an algorithm for preparation of immune plasma.The results of our study, based on the above-mentioned methods of research, showed in the percentage of carrying antibodies to Staphylococcus aureus in the blood, where the highest percentage was in people suffering from skin lesions of staphylococcal infection-58%, and acute respiratory diseases outside the exacerbation stage-28%. It should also be noted that 20-30% of the population of our planet, belonging to healthy people, are carriers of staphylococcal infection.
5. Conclusions
- Blood transfusion can save lives and improve health, but many patients who require transfusion do not have timely access to safe blood. An adequate supply of safe blood and blood products should be an integral part of national health policy and infrastructure in every country. As recommended by the World Health Organization, blood banks are responsible for activities such as the collection, testing, processing, storage, control products. A national blood supply system should be based on a national policy and legislative framework, apply uniform standards in a consistent manner and provide high quality and safe blood, blood components and blood products.The problems of haemotransmissible infections are one of the most important problems of modern transfusion medicine. Today, donor screening, laboratory tests and pathogen inactivation procedures are the most important tools to reduce the risk of blood-borne infections, but they do not eliminate all risks completely. The relevance of this study lies in the fact that it requires a systemic solution by developing scientific and methodological foundations for improving the diagnostic component of staphylococcal infection, which will make it possible to assess the real situation with staphylococcal infection, as well as to prepare a sufficient amount of raw materials for the production of anti-staphylococcal immunoglobulin required for the population of the republic.Sometimes donating blood can save someone's life, and often blood products and components. People affected by staphylococcal infection can also become donors, but only during remission, and their blood will be used as raw material for the production of anti-staphylococcal plasma, which will serve to develop passive immunity for patients with weakened organism, as a consequence and immunity. This will help donors to protect their health for many years from serious diseases and may also save the lives of hundreds of people.
Notes
- 1. https://studfile.net/preview/19495665/page:14/ Characteristics of drugs belonging to the group of serums and immunoglobulins. Bacteriophages.2. * International Units (IU).