-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(5): 1606-1607
doi:10.5923/j.ajmms.20251505.66
Received: Apr. 25, 2025; Accepted: May 21, 2025; Published: May 30, 2025

Clinical and Prognostic Significance of Renal Dysfunction in Patients with Coronary Heart Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLPulatova Parizoda Hamza Kizi1, Tashkenbayeva Eleanora Negmatovna2
1Bukhara State Medical Institute, Bukhara, Uzbekistan
2Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Pulatova Parizoda Hamza Kizi, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study was to study the effect of renal dysfunction on the clinical and prognostic course of coronary heart disease (CAD) in patients with various forms of angina pectoris. 120 patients were examined, divided into two groups: patients with unstable angina (NS) and stable angina pectoris (SSN). The parameters of kidney function (glomerular filtration rate, creatinine, and urea levels), the frequency of adverse cardiovascular outcomes, and the features of the disease course were evaluated. It has been found that renal dysfunction is more common in unstable angina and is associated with a worse prognosis.
Keywords: Coronary heart disease, Renal dysfunction, Angina pectoris, Prognosis, GFR
Cite this paper: Pulatova Parizoda Hamza Kizi, Tashkenbayeva Eleanora Negmatovna, Clinical and Prognostic Significance of Renal Dysfunction in Patients with Coronary Heart Disease, American Journal of Medicine and Medical Sciences, Vol. 15 No. 5, 2025, pp. 1606-1607. doi: 10.5923/j.ajmms.20251505.66.
1. Introduction
- Coronary heart disease (CHD) is a significant public health problem and is responsible for a significant increase in hospitalizations. From a social, epidemiological, and financial point of view, CHD makes the most significant contribution to the structure of cardiovascular morbidity and mortality [1]. The importance of understanding the mechanisms and forming views on the development of renal dysfunction in CHD. Both acute and chronic renal dysfunction are important risk factors for the development of cardiovascular complications (CVC) [2]. In turn, the progression or acute development of cardiovascular failure, accompanied by deterioration of myocardial contractile function, may be an important cause of intrarenal hemodynamic disorders [3]. The formation of unified pathogenetic mechanisms leading to remodeling and disruption of cardiorenal relationships contributes, in particular, to inadequate regulation of water balance with the formation of hyperhydration syndrome, which in some cases can proceed latently [4].The relationship between the heart and kidneys is important for the regulation of their functions and control of hemodynamics. Based on epidemiological and clinical studies, a close relationship has been established between the severity of renal dysfunction, the risk of overall mortality and the occurrence of cardiovascular events [5]. Every 10 ml/min/m2 decrease in glomerular filtration rate (GFR) correlates with a 7% increase in cardiovascular mortality. As is known, there are bidirectional interactionsbetween the heart and kidneys, and changes in hemodynamics in one of the organs can affect the hemodynamics of the other organ [6,7].The purpose of this study was to determine the clinical and prognostic significance of renal dysfunction in patients with CBS with various forms of angina pectoris.
2. Materials and Methods
- 120 patients with CBS who were undergoing inpatient treatment at Bukhara Multidisciplinary Medical Center in 2024-2025 were examined. The average age of the patients was 64.3 ± 8.7 years. Men — 72 (60%), women — 48 (40%).The patients were divided into two groups:Group 1 (n = 60) — patients with unstable angina pectoris.Group 2 (n = 60) — patients with stable angina pectoris of functional class II–III (FC) according to the classification of the Canadian Society of Cardiology.Criteria for assessing kidney function:§ glomerular filtration rate (GFR), calculated using the CKD-EPI formula;§ serum creatinine and urea levels;§ the presence of chronic kidney disease (CKD) — GFR <60 ml/min/ 1.73 m2.Clinical and prognostic indicators:§ a history of myocardial infarction;§ the frequency of hospitalizations over the next 6 months;§ lethality.Research methods:§ clinical examination;§ laboratory and instrumental methods (ECG, echocardiography, biochemical blood analysis);§ 12-month prognosis analysis (hospitalization for cardiac decompensation, myocardial infarction, death).Statistical processing was carried out using the SPSS 26.0 program. To assess the reliability of the differences, the Student's t-test and Pearson's -2-test were used.
3. Results
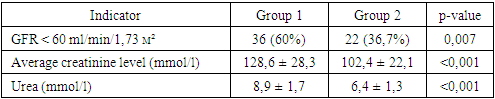
- Based on the results of the analysis, the following results were obtained: In group 1 (unstable angina), renal dysfunction was detected in 36 patients (60%). The average GFR was 58.2 ml/min/1.73 m2.In group 2 (stable angina pectoris), renal dysfunction was noted in 22 patients (36.7%). The average GFR was 66.4 ml/min/1.73 m2 (table 1).
|
|

4. Discussion
- The results obtained indicate a significant prevalence of renal dysfunction in patients with CBS, especially in unstable angina pectoris. Renal dysfunction has a significant impact on the clinical prognosis: it increases the risk of hospitalization, worsens the course of the disease and increases mortality.The mechanisms of influence of impaired renal function on the outcomes of CBS may include hypertension, dyslipidemia, chronic inflammation, activation of the renin-angiotensin-aldosterone system, as well as increased atherosclerosis. This confirms the need for routine assessment of renal function in patients with CBS, especially in unstable clinical presentation.
5. Conclusions
- 1. Renal dysfunction is significantly more common in patients with unstable angina compared with the stable form of CBS.2. Decreased kidney function is associated with a higher risk of cardiovascular complications and mortality.3. GFR assessment should be a mandatory component of risk stratification in patients with CBS.