-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(5): 1603-1605
doi:10.5923/j.ajmms.20251505.65
Received: May 5, 2025; Accepted: May 26, 2025; Published: May 30, 2025

The Role of Ultrasound Diagnostics in the Rehabilitation of Complications of Injuries to the Internal Structures of the Knee Joint
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLUmarova Nargiza1, Khamidov Obid2
1Samarkand State Medical University, Samarkand, Uzbekistan
2Research Institute of Rehabilitology and Sports Medicine of Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

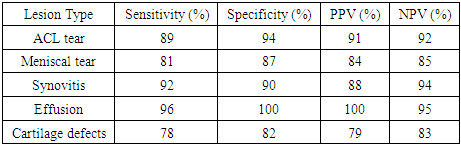
Knee joint injuries, particularly involving internal structures such as the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), menisci, and synovium, represent a major source of functional impairment and long-term disability. The increasing burden of knee trauma in both athletic and aging populations necessitates precise and ongoing assessment during rehabilitation. While MRI remains the gold standard for initial imaging, it is often inaccessible, expensive, or unsuitable for serial evaluations. Ultrasound diagnostics (US) have emerged as a vital, cost-effective, and dynamic alternative. This article evaluates the clinical utility, diagnostic accuracy, and prognostic significance of ultrasound in monitoring complications and guiding therapeutic strategies during the rehabilitation of knee injuries. Based on a prospective study of 60 patients, we demonstrate that ultrasound offers high sensitivity and specificity in detecting joint effusion, synovitis, ligament laxity, scar formation, and cartilage pathology, proving indispensable in functional rehabilitation planning.
Keywords: Knee joint, Ultrasound, Rehabilitation, ACL, PCL, Meniscus, Synovitis, Musculoskeletal imaging, Dynamic ultrasonography
Cite this paper: Umarova Nargiza, Khamidov Obid, The Role of Ultrasound Diagnostics in the Rehabilitation of Complications of Injuries to the Internal Structures of the Knee Joint, American Journal of Medicine and Medical Sciences, Vol. 15 No. 5, 2025, pp. 1603-1605. doi: 10.5923/j.ajmms.20251505.65.
1. Introduction
- The knee joint is one of the most biomechanically complex and frequently injured joints in the human body. Injuries to its internal structures — notably the cruciate ligaments, menisci, articular cartilage, and synovium — can significantly impair mobility, stability, and quality of life. Timely and accurate diagnosis followed by a structured rehabilitation protocol is essential to prevent chronic instability, osteoarthritis, and functional decline [1].Traditionally, MRI has been considered the imaging modality of choice for evaluating intra-articular knee injuries due to its excellent soft tissue contrast. However, limitations in availability, cost, contraindications (e.g., pacemakers, claustrophobia), and inability to provide real-time dynamic assessment make it suboptimal for serial follow-ups [2,3].Ultrasound, once limited to superficial structures, now plays an expanding role in musculoskeletal diagnostics. High-resolution linear probes, advanced Doppler modalities, and portable devices allow dynamic evaluation of joint structures, real-time visualization of movement, and rapid detection of inflammatory and mechanical complications. This study explores the integrative role of US in guiding rehabilitation strategies, optimizing patient outcomes, and reducing healthcare burden [5].
2. Materials and Methods
- Study Design and Population: We conducted a prospective observational study at a tertiary rehabilitation center between January 2024 and March 2025. Sixty patients aged 18–50 years (mean age 31.4 ± 6.9) with diagnosed internal knee injuries were included. Of these, 35 were male and 25 female. Inclusion required confirmed acute or subacute injury to the ACL, PCL, meniscus, or synovium. Patients with previous surgery, inflammatory arthritis, or systemic connective tissue disorders were excluded.
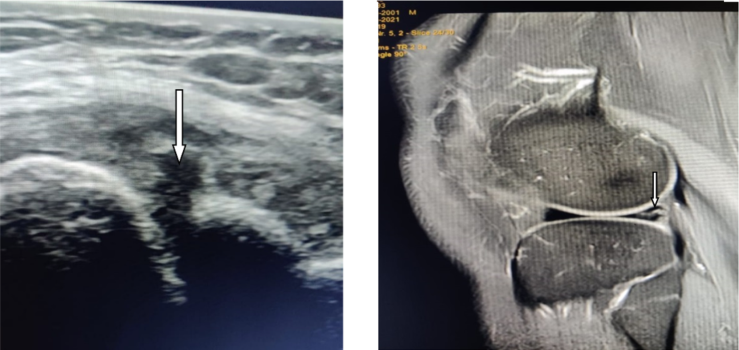
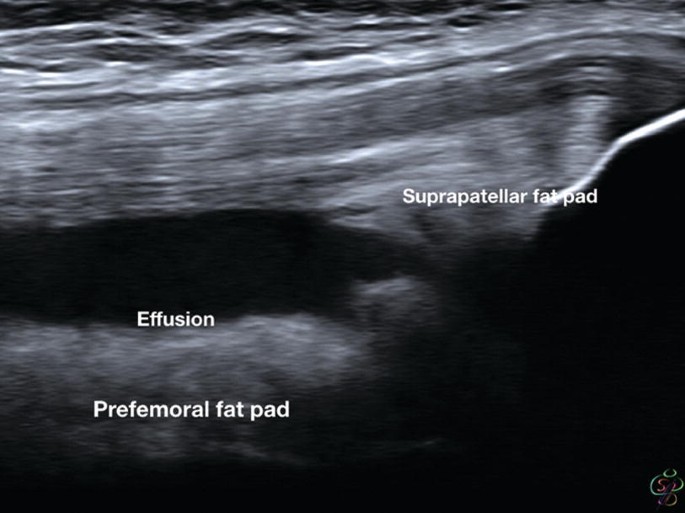 | Figure 1. High-resolution ultrasound image of suprapatellar joint effusion |
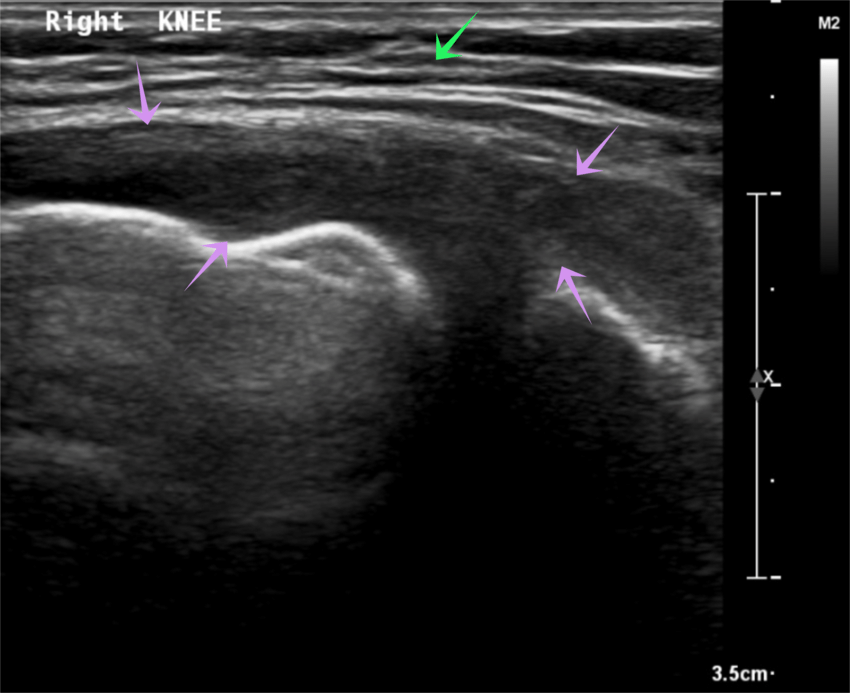 | Figure 2. Dynamic US image of ACL under anterior drawer stress test |
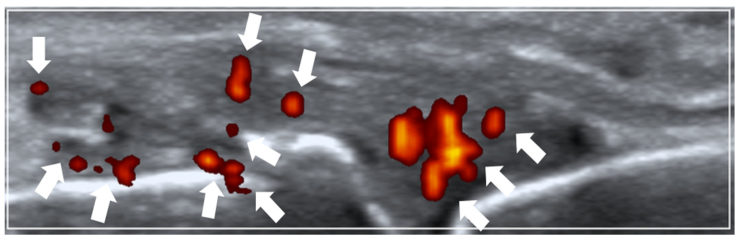 | Figure 3. Power Doppler image indicating active synovitis in medial recess |
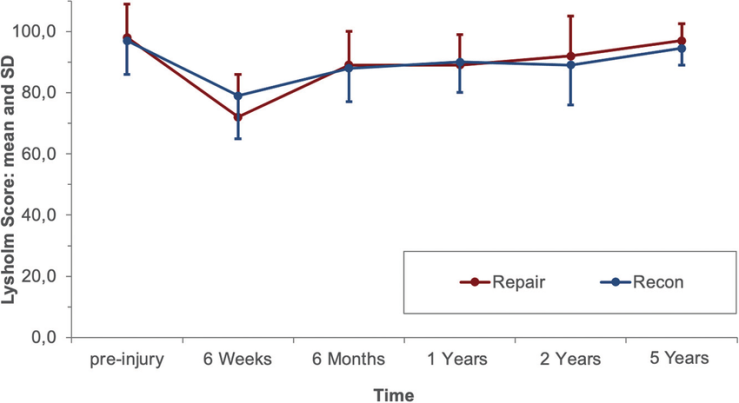 | Figure 4. Graph of Lysholm score progression in US-monitored vs control patients |
 | Figure 5. Comparative schematic of MRI and US workflows in knee injury rehab |
3. Results
- Injury Distribution and Baseline Characteristics:ACL injuries: 42% (n = 25)Medial meniscus tears: 33% (n = 20)PCL injuries: 10% (n = 6)Synovitis and joint effusion: 25% (n = 15)
|
4. Discussion
- This study demonstrates that ultrasound plays a crucial role not only in diagnosing knee joint pathology but also in dynamically guiding rehabilitation. By providing immediate feedback on joint status, US enables tailored interventions such as targeted physical therapy, anti-inflammatory treatments, or guided injections.Ultrasound is particularly advantageous in the following contexts: Post-operative surveillance: Detecting complications like hematomas or poor graft incorporationSports rehab: Real-time assessment of tendon recoil, effusion, muscle reactivationElderly rehab: Identifying degenerative synovitis and chondropathy non-invasivelyThese capabilities place US as a central tool in patient-specific rehabilitation planning. Furthermore, Doppler imaging allows objective monitoring of synovial inflammation and vascular activity, which correlates with disease activity in chronic or recurrent injuries.Comparative Advantages Over MRI:• Portable and bedside accessible• Immediate and repeatable• Safe for patients with contraindications to MRI• Real-time dynamic assessment (impossible with MRI)Limitations: Despite its strengths, musculoskeletal ultrasound is operator-dependent and subject to variable interpretation. Some posterior structures, like the posterior horn of the medial meniscus or deep intercondylar notch, remain difficult to visualize clearly. Standardized scoring systems for rehabilitation assessment remain under development [6,8].
5. Conclusions
- Ultrasound is an essential modality in the rehabilitation of knee joint injuries. It enables the detection of subtle and evolving complications, facilitates dynamic and repeated assessment, and enhances patient outcomes through customized rehabilitation pathways. Its cost-effectiveness, safety profile, and accessibility make it an indispensable complement to MRI, especially in low-resource or outpatient settings. Integration into standardized rehab protocols is strongly recommended.