-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(5): 1566-1569
doi:10.5923/j.ajmms.20251505.57
Received: Apr. 17, 2025; Accepted: May 16, 2025; Published: May 30, 2025

Risk Stratification of Thyroid Nodules Using the Thyroid Imaging Reporting and Data System (ACR-TIRADS) in Women of Reproductive Age in Kashkadarya Region
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKholikova A. O.1, Kenjaeva D. I.2
1Republican Specialized Scientific and Practical Medical Center of Endocrinology (RSSPMCE) of the Ministry of Health of the Republic of Uzbekistan named after academician E.Kh. Turakulov, Department of Neuroendocrinology, Tashkent, Republic of Uzbekistan
2Kashkadarya Branch of the RSSPMCE Ministry of Health of the Republic of Uzbekistan named after Academician. Y.H. Turakulova, Tashkent, Republic of Uzbekistan
Correspondence to: Kholikova A. O., Republican Specialized Scientific and Practical Medical Center of Endocrinology (RSSPMCE) of the Ministry of Health of the Republic of Uzbekistan named after academician E.Kh. Turakulov, Department of Neuroendocrinology, Tashkent, Republic of Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

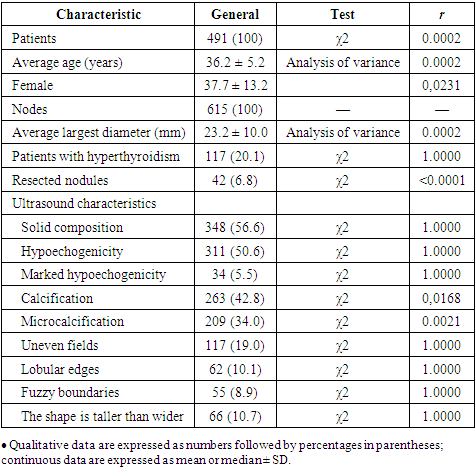
A total of 491 women of reproductive age (prospectively) with thyroid nodules (TN) were examined in the period from 2014 to 2024 in the Kashkadarya branch of the Republican Scientific and Practical Medical Center of Endocrinology and Epidemiology of the Ministry of Health of the Republic of Uzbekistan. The average age of the patients was 36.2 ± 5.2 years. The control group consisted of 20 healthy women of the corresponding age.The use of thyroid ultrasound, aimed at detecting developing tumors, in routine surveillance of patients with TN may aid in the early detection of thyroid malignancies The combination of thyroid scintigraphy in the TIRADS model is important for preventing unnecessary fine-needle biopsy and thyroid surgery.
Keywords: Nodular goiter, TIRADS, Women
Cite this paper: Kholikova A. O., Kenjaeva D. I., Risk Stratification of Thyroid Nodules Using the Thyroid Imaging Reporting and Data System (ACR-TIRADS) in Women of Reproductive Age in Kashkadarya Region, American Journal of Medicine and Medical Sciences, Vol. 15 No. 5, 2025, pp. 1566-1569. doi: 10.5923/j.ajmms.20251505.57.
1. Introduction
- Thyroid nodules are a common finding, especially in iodine-deficient regions. Ultrasound scoring systems such as the Thyroid Imaging Reporting and Data System (TIRADS) are useful in differentiating benign from malignant thyroid nodules, offering a risk stratification model. Depending on the constellation or number of suspicious ultrasound features, fine-needle biopsy is recommended. Thyroid nodules are more common in women [1], although the reasons for this phenomenon are not fully understood. There is an opinion that the appearance of nodules is associated with various factors, including increased estrogen levels, autoimmune diseases, stress, environmental endocrine disorders, excess iodine, and other circumstances.The prevalence of thyroid nodules is high, especially in iodine-deficient countries [1]. Overall, the prevalence of thyroid nodules in adults without previously diagnosed thyroid disease is estimated to be 59%, with a higher prevalence in the elderly population. [2,3]. In addition, multinodular structure is a common finding in patients with thyroid nodules. [3,4]. However, only a small number of these nodules are of clinical significance. Accordingly, the official journal of the German Medical Association has published a statement against sonographic screening of thyroid nodules in elderly asymptomatic patients. [5]. A similar recommendation against screening asymptomatic adults was published in 2017 by the U.S. Preventive Services Task Force. [6]. On the other hand, thyroid nodules are a common incidental finding on imaging studies of the neck, including arterial duplex sonography, MRI or CT, and ultrasonography in the context of otolaryngological examinations. Thus, it is necessary to decide which nodules represent a potential risk and require further investigation to identify either those that are presumed to be malignant (fine needle biopsy, thyroid surgery) or those that are functionally significant autonomous nodules.Official guidelines emphasize the importance of high-resolution ultrasound for accurate assessment of the sonomorphological features of nodules. B-mode ultrasound can be combined with color duplex to assess vascularity and, more recently, with sonoelastography to assess the elasticity or stiffness of thyroid nodules. [7,8].In the past, several ultrasound characteristics have been identified that indicate malignant or benign nodules. [9,10]. ACR TI-RADS classifies ultrasound features as benign, low suspicious, moderately concerning, or highly suspicious for malignancy. Each ultrasound feature of a nodule is assigned a score, with additional points being given to more worrisome features. When analyzing a nodule, the physician selects one feature from the first four categories, plus all relevant features from the last category, and calculates a total score. The resulting score determines the ACR TI-RADS grade of the nodule, which ranges from TR1 (benign) to TR5 (high probability of malignancy). The above served as the reason for the present study.Main part – to investigate the value of the ACR-TIRADS classification in assessing the risk stratification of thyroid nodules.
2. Material and Inspection Methods
- 491 women of reproductive age (prospectively) with NTG were examined in the period from 2014 to 2024 in the Kashkadarya branch of the Republican Scientific and Practical Medical Center of Epidemiology and Gynecology of the Ministry of Health of the Republic of Uzbekistan. The average age of the patients was 36.2 ± 5.2 years. The control group consisted of 20 healthy women of the corresponding age. Inclusion criteria: autoimmune thyroiditis, nodular, women of childbearing age.Exclusion criteria: pregnant and lactating women, children and adolescents, men, type 1 diabetes mellitus, chronic adrenal insufficiency, acute kidney and heart disease, connective tissue diseases, vasculitis, amyloidosis, systemic cancer, vitiligo, rheumatism. Research methods – general clinical, biochemical (bilirubin, direct, indirect, lipid spectrum, ALT, AST, PTI, coagulogram, hormonal (TSH, free thyroxine, antibodies to TPO, to thyroglobulin and thyrocyte receptors, prolactin in the blood) and instrumental: ECG, ultrasound of the thyroid gland, internal organs, chest X-ray, etc.Thyroid ultrasound examination was performed using a Hitachi EUB 5000 G or Hitachi Avius Hi Vision equipped with a 5–10 MHz linear transducer.The analysis included American recommendations for thyroid nodules according to the ACR-TIRADS (American College of Radiology-Thyroid Image Reporting and Data System) classification. Statistical calculations were performed in the Microsoft Windows software environment using the Microsoft Excel-2007 and Statistica version 6.0, 2003 software packages. We summarized the baseline and demographic characteristics using descriptive statistics. A two-sided p<0.05 was considered statistically significant.
3. Research Results
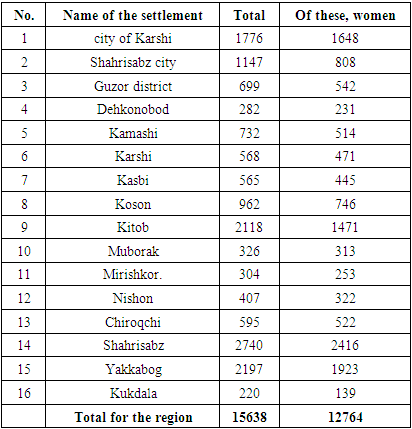
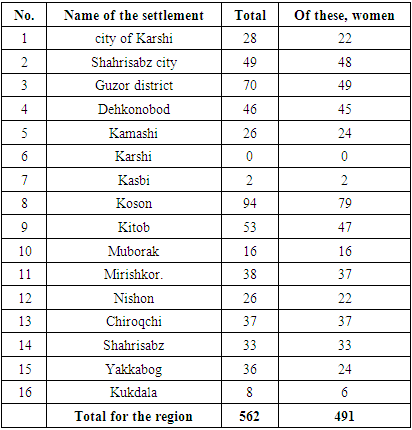
- First of all, we analyzed the number of women registered with thyroid diseases in 2024 (Table 1).
|
|
|
4. Conclusions
- The implementation of the ACR TIRADS system is a necessary measure for the early diagnosis of thyroid nodules. This system provides step-by-step instructions on the management and monitoring of thyroid nodules, creating conditions for timely puncture biopsy.