-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(5): 1474-1480
doi:10.5923/j.ajmms.20251505.37
Received: Apr. 22, 2025; Accepted: May 21, 2025; Published: May 27, 2025

Immunohistochemical Study of Morphological Changes in Patients with Uterine Cancer
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJuraeva Gulbakhor1, Mamadalieva Yashnar2, Amanov Akma1
1Assistant, Termez Branch of the Tashkent Medical Academy, Termez, Uzbekistan
2Professor, Department of Oncology of the Center for the Development of Professional Qualifications of Medical Workers of the Ministry of Health of the Republic of Uzbekistan, DSc, Professor, Tashkent, Uzbekistan
Correspondence to: Juraeva Gulbakhor, Assistant, Termez Branch of the Tashkent Medical Academy, Termez, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In this study, an immunohistochemical analysis of the expression of Ki-67, p53, and Bcl-2 markers was conducted in 60 patients with uterine body adenocarcinoma, divided into three groups depending on the degree of tumor differentiation (high, moderate, low; 20 patients in each group). The study was conducted using a Bond (Leica, Australia) automated immunohistochemical processor. It has been established that the expression of Ki-67, p53, and Bcl-2 increases as the degree of tumor differentiation decreases. Thus, in highly differentiated adenocarcinoma, a weak positive reaction (up to 30%) prevailed for all three markers, while in low-differentiated tumors, a high expression (more than 60%) was significantly more common. Microscopically, signs of pronounced cellular atypia, endometrial gland hyperplasia, myometrial invasion, and pathological mitoses were identified, especially in the G2 and G3 groups. The obtained data indicate that the indicators of proliferative activity (Ki-67), anti-apoptotic activity (Bcl-2), and mutational instability (p53) can be used as prognostic markers of tumor biological aggressiveness and contribute to determining the treatment tactics of patients with endometrial cancer.
Keywords: Endometrial cancer, Ki-67, p53, Bcl-2, Immunohistochemistry, Degree of differentiation, Morphology, Proliferation
Cite this paper: Juraeva Gulbakhor, Mamadalieva Yashnar, Amanov Akma, Immunohistochemical Study of Morphological Changes in Patients with Uterine Cancer, American Journal of Medicine and Medical Sciences, Vol. 15 No. 5, 2025, pp. 1474-1480. doi: 10.5923/j.ajmms.20251505.37.
1. Introduction
- According to WHO estimates, more than one billion people on our planet are overweight or obese. In Western European countries, 20-25% of women are obese. Statistics show that excess weight is detected in 54% of the Russian population. A characteristic feature of obesity is that it is often combined with serious diseases: type 2 diabetes mellitus, arterial hypertension, dyslipidemia, atherosclerosis, coronary heart disease, some types of reproductive diseases [9]. According to preliminary calculations by American Cancer RE, in 2019, 61,880 cases of endometrial cancer were diagnosed in the United States, with a mortality rate of 12,160. [22].In the period from 40 to 59 years, there is a sharp increase in the incidence of endometrial cancer, increasing approximately 4 times, gradually reaching a peak at 60-64 years, after which it significantly decreases. Thus, by age 65, the risk increases threefold, and by age 75, it increases 4.7 times. [23]. A number of biological factors may be involved in the relationship between obesity and endometrial cancer. Excessive accumulation of adipose tissue in postmenopausal women leads to an increase in estrogen levels, which, in turn, contributes to an increase in the mitotic activity of endometrial cells in the absence of a balancing effect of progesterone. [17].Bcl2 suppresses apoptosis in multicellular systems, including lymphohematopoietic and neuronal cells. It regulates cell death by controlling the permeability of the mitochondrial membrane.Bcl 2 suppresses apoptosis, including in lymphohematopoietic and neuronal cells. Depending on the prevalence and intensity of the immunohistochemical reaction, the eyepiece and objective 10-40 objects were examined in the field of view depending on the percentage of stained cells, and the absence of expression or staining of less than 10% of cells was assessed systematically - 0 points, from 10 to 30% - 1 point, from 30 to 60 50% - 2 points, from 60 to 100% - 3 points. The expression of Bcl 2 manifested itself in the form of brown staining of the cytoplasm of epithelial cells of varying intensity.Ki-67-protein (also known as MKI 67) is a cellular marker for proliferation and can be used in immunohistochemistry. This is closely related to cell proliferation. The proportion of Ki-67-positive tumor cells (Ki-67 marking index) is often associated with the clinical course of cancer. Ki-67-nuclear protein is a marker of the proliferative activity of cells and is evaluated as a percentage. Ki 67 is used for diagnostic purposes to determine the biological potential of malignant tumors in humans. The staining of nuclear cells is described as follows. <10% low activity, 10-20% moderate activity, >20% high proliferative activity. Through these results, it is possible to determine the prognostic factor of cancer.The antigen for these antibodies is the protein p53, which controls the course of cell cycle processes, as well as the presence of damage in the genome, which can lead to the further development of pathology. p53-dependent apoptosis is a powerful selector, preventing the accumulation of mutations, and if they have already appeared, p53-dependent apoptosis allows the destruction of such potentially dangerous cells for the organism. This gene encodes a transcription factor that controls the entry of cells into the cell cycle. Like all tumor suppressants, p53 controls the normal course of the cell cycle. p53 is a transcription factor that regulates the cell cycle; this reagent acts as a suppressor of the formation of malignant tumors. The p53 gene is an anti-oncogenic agent.
2. Research Material and Method
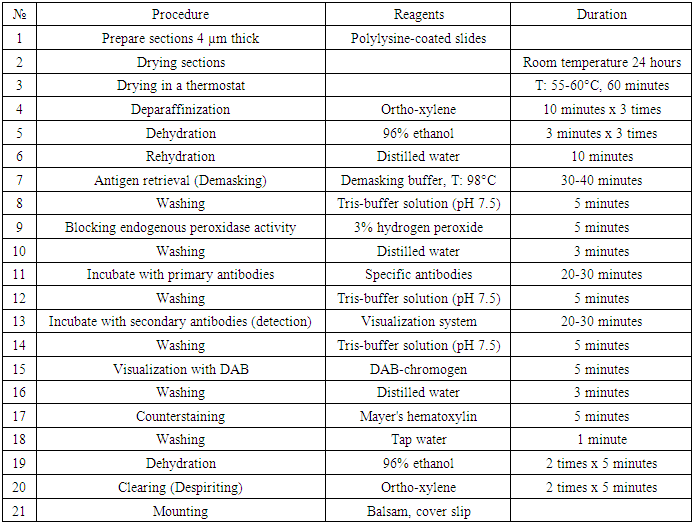
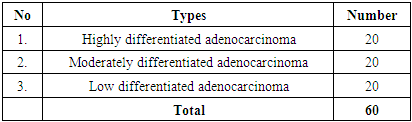
- To study pathomorphologically malignant tumors by the immunohistochemical method, a total of 60 patients with uterine cancer were examined by immunohistochemistry for the degree of selective differentiation, 20 each from 3 groups. In addition to the results of morphological studies, immunohistochemical studies are currently recognized worldwide as the gold standard. For immunohistochemical examination, cell expression through monoclonal antibodies Ki67, Bcl 2, and p53 was studied using an immunohistoprocessor from Bond Leica Australia (Australia). In all patients, candle blocks were cut, treated for immunocytochemical examination, slices were taken on a slide and examined using the immunohistochemical examination method for Ki67, Bcl 2, and p53 antigens. The conducted immunohistochemical examination method was technically carried out as follows (Table 1).
|
|
3. Results
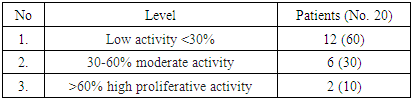
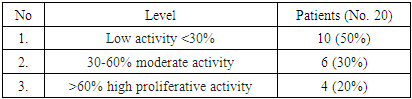
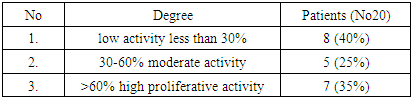
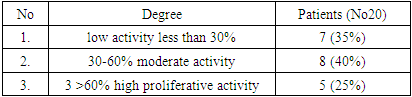
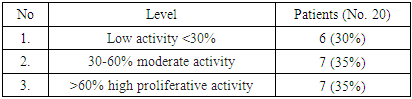
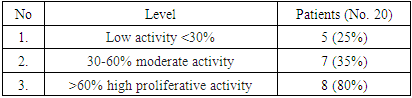
- As a result, highly differentiated adenocarcinoma: For this study, 20 patients with highly differentiated cancer were selected. The results obtained in all patients were evaluated as a percentage of the marker of proliferative activity of Ki 67 tumor cells. The obtained results were assessed as mild, moderate, and severe positive reactions. Of the 20 observed patients, 12 (60%) had a mild positive reaction, 6 (30%) had a moderate positive reaction, and 2 (10%) had a high positive reaction. No negative reaction processes were observed (Table 3).
|
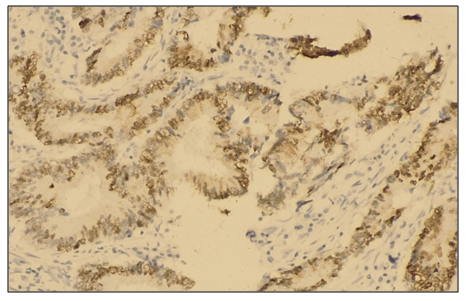
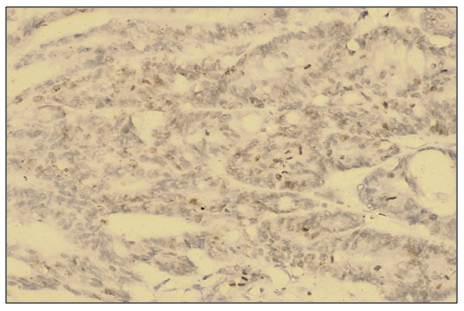 | Figure 1. Medium positive Ki 67 reagent reaction in highly differentiated adenocarcinoma in uterine body cancer. IGX - Dab chromogen. Ob10. Ok40 |
|
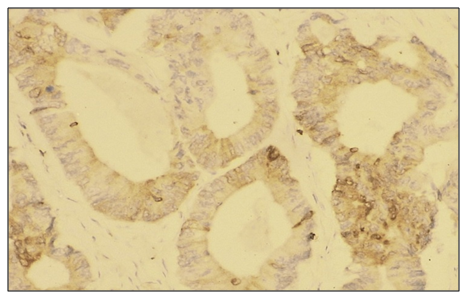
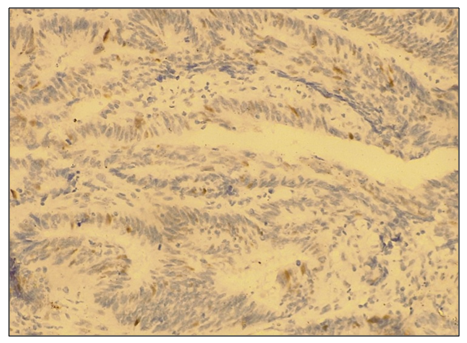 | Figure 2. Cancer of the uterine body in highly differentiated adenocarcinoma with a low degree of positive reaction to reagent p53 |
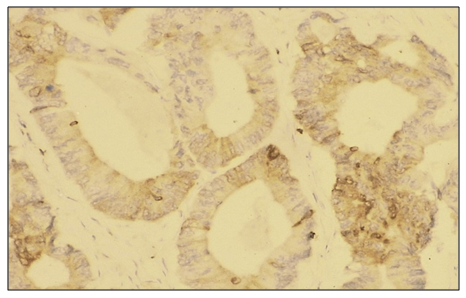 | Figure 3. Immunohistochemical micropreparation: Moderate expression of the Bcl-2 gene in a highly differentiated type of uterine body cancer. cytoplasmic reaction, tumor cell membranes stained brown. Ob10 × ok40 |
|
|
|
 | Figure 4. Low level positive reaction of p53 reagent in moderately differentiated adenocarcinoma in uterine body cancer. IGX - Dab chromogen. Ob10. Ok40 |
 | Figure 5. Immunohistochemical micropreparation: Moderate expression of the Bcl-2 gene in moderately differentiated uterine cancer cytoplasmic reaction, tumor cell membranes stained brown. Ob10 ×ok40 |
|
|
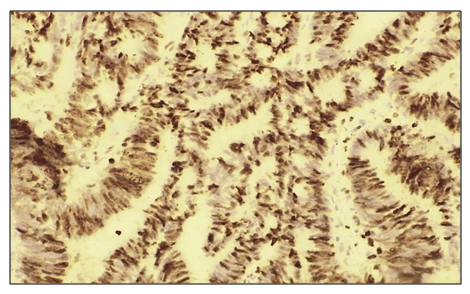 | Figure 6. In low-differentiated adenocarcinoma with uterine carcinoma High positive reaction to reagent Ki 67. IGX - Dab chromogen. Ob10. Ok40 |
|
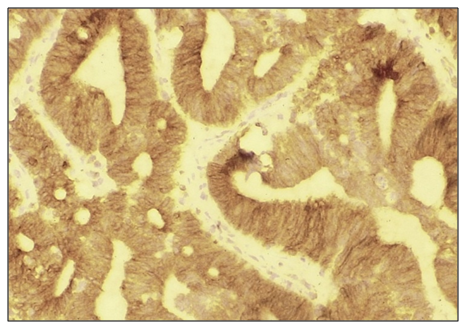 | Figure 7. Immunohistochemical micropreparation: Moderate expression of the Bcl-2 gene in low-differentiated uterine body cancer cytoplasmic reaction, tumor cell membranes stained brown. Ob10 ×ok40 |
|
4. Conclusions
- The conducted study showed that immunohistochemical study of the expression of proliferative (Ki-67), apoptotic (Bcl-2), and suppressor (p53) markers in patients with endometrial cancer allows for an objective assessment of the biological characteristics of tumors depending on the degree of their differentiation.A significant correlation was found between the expression level of the studied markers and the degree of tumor differentiation. Thus, in highly differentiated uterine body adenocarcinoma, low expression of Ki-67, Bcl-2, and p53 prevailed, indicating less aggressive biological potential. At the same time, in moderate and especially low-differentiated forms of adenocarcinoma, high proliferative activity was observed, increased expression of the p53 and Bcl-2 marker, which indicates a greater tendency of the tumor to invasive growth, metastasis, and recurrence.The obtained data confirm the diagnostic and prognostic significance of immunohistochemical prophylaxis in endometrial adenocarcinoma. Elevated expression of Ki-67 and p53 in G2-G3 tumors can be considered a potential unfavorable prognostic factor. Increased Bcl-2 expression, despite its antiapoptotic nature, is also associated with an unfavorable clinical course of the disease in certain cases.Thus, determining the expression of Ki-67, p53, and Bcl-2 markers can serve as a reliable tool for risk stratification, choosing treatment tactics, and assessing the prognosis in patients with uterine body adenocarcinoma.