-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(5): 1427-1438
doi:10.5923/j.ajmms.20251505.24
Received: Apr. 25, 2025; Accepted: May 12, 2025; Published: May 17, 2025

The Organization of Gynecological Healthcare During the COVID-19 Pandemic and in the Post-COVID Period
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRizaeva Malika Abdumanonovna1, Kattakhodjaeva Makhmuda Khamdamovna1, Rizaev Jasur Alimdjanovich2
1Department of Obstetrics and Gynecology, Tashkent State Dental Institute, Tashkent, Uzbekistan
2Rector of Samarkand State Medical University, Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Rizaeva Malika Abdumanonovna, Department of Obstetrics and Gynecology, Tashkent State Dental Institute, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The COVID-19 pandemic significantly disrupted the organization and provision of gynecological healthcare services worldwide. Routine screening programs, oncological treatment protocols, reproductive care, and chronic condition management were adversely affected by system overload, movement restrictions, and shifts in resource allocation. However, the crisis also stimulated rapid innovation, leading to the integration of hybrid care models, robotic-assisted surgery, artificial intelligence in diagnostics, and adaptive therapeutic pathways. Molecular and regenerative approaches, including exosomal biomarkers and stem cell therapies, gained traction as future solutions. This review analyzes the key challenges, responses, and post-pandemic transformations in gynecology, highlighting the need for strategic investment in resilience, digital equity, and patient-centered models. The findings emphasize that the innovations triggered by the pandemic are not transitional but form the foundation of a new paradigm in gynecological care.
Keywords: COVID-19, Gynecological healthcare, Innovation, Screening programs, Robotic surgery, Artificial intelligence, Reproductive medicine, Oncology, Post-pandemic recovery, Assisted Reproductive Technology (ART), Polycystic Ovary Syndrome (PCOS), Primary Ovarian Insufficiency (POI)
Cite this paper: Rizaeva Malika Abdumanonovna, Kattakhodjaeva Makhmuda Khamdamovna, Rizaev Jasur Alimdjanovich, The Organization of Gynecological Healthcare During the COVID-19 Pandemic and in the Post-COVID Period, American Journal of Medicine and Medical Sciences, Vol. 15 No. 5, 2025, pp. 1427-1438. doi: 10.5923/j.ajmms.20251505.24.
Article Outline
1. Introduction
- The COVID-19 pandemic has become one of the most severe public health crises of the 21st century, affecting all levels of healthcare organization. Among the most sensitive and complex domains impacted was gynecological care, which serves not only as a clinical branch but as a fundamental component of women’s health, reproductive safety, and national demographic policy [1], [2], [3]. The sudden redirection of healthcare resources toward pandemic containment, the suspension of planned interventions, and the fragmentation of continuity of care disrupted the accessibility and effectiveness of gynecological services worldwide [4], [5], [6].During the first wave of the pandemic, many healthcare institutions were forced to close or repurpose gynecological departments, postponing or cancelling oncological surgeries, infertility treatments, and even routine prenatal consultations [7], [8], [9], [10]. This led to a cascade of adverse outcomes: delayed diagnoses of reproductive system malignancies, aggravation of chronic gynecological conditions, and a surge in emergency interventions due to neglected cases [11], [12], [13], [14], [15], [16], [17]. The psychological toll on women — stemming from anxiety, fear of infection, and isolation — further compounded these medical challenges [18], [19].Pregnant women became a particularly vulnerable cohort, facing both heightened clinical risks associated with SARS-CoV-2 and logistical barriers to consistent perinatal monitoring [20], [21], [22], [23]. International studies reported increased incidence of preterm birth, preeclampsia, and placental insufficiency in COVID-positive pregnancies, while the restructuring of obstetric care required rapid adaptation, including the establishment of dedicated COVID-19 maternity centers [24], [25], [26], [27], [28].The pandemic also accelerated the adoption of telemedicine in gynecological practice, which emerged as both a necessity and an innovation [29], [30], [31], [32], [33]. Remote consultations allowed for continuity of care in many cases, yet the unequal distribution of digital infrastructure and disparities in health literacy exposed existing gaps in healthcare equity [34], [35], [36], [37], [38].In the post-pandemic period, healthcare systems continue to experience the residual effects of systemic overload and delayed care. The need to restore screening programs, clear surgical backlogs, and address long-term psychosocial consequences remains urgent [39], [40], [41], [42], [43]. Furthermore, new variants of the virus, vaccine-related considerations in reproductive health, and the rise of post-COVID syndromes call for a rethinking of gynecological care models at both clinical and administrative levels [44], [45], [46], [47].This review aims to analyze the multifaceted transformations in the organization of gynecological healthcare during the COVID-19 pandemic and the subsequent post-COVID period. Based on international experience, current scientific literature, and policy analyses, the article identifies key challenges, successful strategies, and innovative practices that may guide the development of resilient, equitable, and patient-centered gynecological care systems in future health emergencies [48], [49], [50].
2. Organizational Challenges and Resource Redistribution During the COVID-19 Pandemic
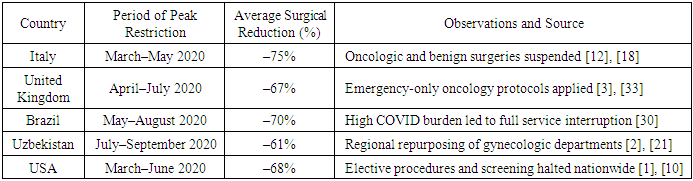
- An The COVID-19 pandemic triggered a global reconfiguration of healthcare systems, forcing institutions to adapt swiftly to the surging demand for infectious disease management. In this context, gynecological healthcare services — including surgical, outpatient, and diagnostic units — were subjected to extensive restructuring, often to the detriment of timely access and service continuity for women [2], [4], [6], [30], [51].From the early months of the pandemic, elective gynecological procedures were deprioritized or suspended entirely, as hospitals reallocated operating theatres, anesthesiology teams, and intensive care beds to COVID-19 patients [1], [29], [12]. This reallocation disproportionately affected interventions for conditions deemed “non-urgent” — such as uterine fibroids, endometriosis, infertility, and pelvic organ prolapse — which, under crisis conditions, were deferred indefinitely [3], [24], [52] [18]. However, the cumulative effect of these delays led to symptom progression, emotional distress, and reduced quality of life for many patients [14], [17].The impact was particularly critical in gynecologic oncology, where the postponement of diagnostic procedures and cancer surgeries resulted in delayed treatment initiation and worse prognoses [10], [20], [19]. Studies conducted in multiple countries — including Italy, Brazil, the UK, and Uzbekistan — confirm significant reductions in the number of surgeries for endometrial, cervical, and ovarian malignancies, sometimes exceeding 70% during lockdown peaks [30], [12], [18], [33]. These disruptions contradicted established oncologic timelines and necessitated modifications to clinical protocols, including the increased use of neoadjuvant therapy and abbreviated follow-up schedules [25], [28].In many hospitals, gynecological departments were partially or entirely converted into COVID-19 treatment zones, and medical staff were reassigned to pandemic response teams — often without adequate retraining or protective resources [2], [21], [40]. This contributed to professional burnout, increased medical errors, and compromised patient safety, particularly in emergency gynecological cases such as ectopic pregnancy, ovarian torsion, and intrauterine bleeding [24], [19], [39].Maternal care services also faced destabilization: outpatient prenatal monitoring was curtailed, perinatal diagnostics reduced, and antenatal classes cancelled. Infected pregnant women were isolated in designated COVID wards, frequently under limited obstetric supervision [7], [20], [34]. The psychosocial burden among expectant mothers rose sharply, with anxiety over fatel outcomes, uncertainty about delivery conditions, and inconsistent access to support services [14], [17], [43].At the policy level, the absence of unified crisis-response guidelines for reproductive health led to variability in care provision across regions and countries [6], [12], [25]. Some institutions managed to preserve minimal functional capacities for urgent gynecologic and obstetric care through clear triage protocols and the use of teleconsultations, while others experienced near-total service paralysis.To illustrate the global scale of surgical reduction in gynecology during the pandemic, Table 1 presents comparative data from several countries.
|
3. Access and Quality of Gynecological Services During the Pandemic
- The COVID-19 pandemic has revealed deep vulnerabilities in the accessibility and quality assurance mechanisms of gynecological care systems. While hospitals focused on pandemic response, routine gynecological services experienced critical operational regression, disproportionately affecting diagnostic timeliness, disease progression control, and health equity across female populations [1], [3], [29].
3.1. Barriers to Access: Psychological, Logistical, and Structural Dimensions
- Access to gynecological care during the pandemic was impaired not only by formal restrictions but also by the pervasive fear of contracting COVID-19 in clinical settings. Multiple studies reported a drastic decline in patient-initiated visits for early gynecologic symptoms, such as pelvic pain, menstrual irregularities, and intermenstrual bleeding — conditions which, under normal circumstances, would have warranted immediate investigation [10], [12], [18].Additionally, lockdown measures, suspension of intercity transport, and limited functioning of peripheral clinics disproportionately affected women in rural and semi-urban areas, creating a geographical inaccessibility to both outpatient and surgical services [20], [30]. Patients from socioeconomically disadvantaged backgrounds were especially vulnerable, as many relied on public transport, state-funded clinics, or community health outreach — all of which were severely disrupted [2], [14], [34].Cultural and domestic factors further exacerbated inaccessibility. In some regions, gender roles and social stigma prevented women from seeking care during lockdowns unless the condition was life-threatening. Reports also highlighted reduced medical access for women experiencing domestic violence, who often lacked the autonomy or privacy required to engage in healthcare during confinement [33], [43].
3.2. Decline in Care Quality: Interrupted Protocols and Diagnostic Regression
- Quality of care suffered dramatically as a result of personnel redeployment, PPE shortages, and cancellation of preventive and follow-up services. Key diagnostic protocols — including cervical screening programs, colposcopies, transvaginal ultrasonography, and endometrial biopsies — were either suspended or scaled back, leading to diagnostic delays in precancerous and oncologic conditions [3], [17], [24].In gynecologic oncology, this translated into an increase in late-stage diagnoses for cervical and endometrial cancers, as documented in multiple retrospective cohort studies [10], [19], [21]. Patients under hormonal or conservative treatment protocols lost routine surveillance, and many with suspected malignancies faced months-long delays in diagnostic confirmation and surgical intervention [20], [25].Women with chronic gynecological conditions such as endometriosis, Polycystic Ovary Syndrome (PCOS), and adenomyosis also experienced a deterioration in their quality of life. These conditions, already associated with pain, hormonal dysregulation, and psychological comorbidity, worsened due to the discontinuation of individualized therapeutic monitoring, including imaging and medication titration [6], [7], [39].Moreover, mental health support for women with chronic conditions or infertility was largely unavailable during the crisis, resulting in increased incidence of depressive symptoms, anxiety, and social withdrawal — factors that further impaired treatment compliance and general well-being [14], [28].
3.3. Digital Divide in Remote Gynecological Services
- While telemedicine was rapidly adopted as a compensatory mechanism, its effectiveness in gynecology was limited by the digital divide — a disparity in access to devices, internet connectivity, and digital literacy. Women from low-income, elderly, and marginalized groups had significantly lower access to smartphones, stable internet, or private space necessary for confidential teleconsultations [33], [35], [40], [53].Even among digitally equipped populations, the clinical limitations of remote consultations became evident. Gynecological conditions often require physical examinations, pelvic imaging, and procedural interventions — none of which can be reliably substituted by video or telephone interaction. This led to misdiagnoses, delayed triage, and incomplete management plans [18], [24], [25].Furthermore, the abrupt switch to digital formats without patient education or training in telehealth protocols created confusion, nonadherence, and technological fatigue. Many clinicians reported difficulties in conducting informed consent, assessing pain, or identifying psychological distress via telemedicine platforms [34], [43].
4. Telemedicine in Gynecological Practice: Pandemic Catalyst and Future Tool
- The COVID-19 pandemic became a turning point in the digital transformation of healthcare, and gynecological practice was no exception. Although traditionally grounded in in-person diagnostics and physical examinations, gynecology adapted rapidly to the use of telehealth tools to ensure continuity of care, minimize exposure risk, and maintain patient-provider communication [2], [14], [30], [54]. This shift, while born of necessity, opened new avenues for hybrid healthcare models in the post-COVID era.
4.1. Rapid Expansion and Clinical Integration
- The acute need for maintaining gynecological care during lockdowns led to the accelerated deployment of telemedicine platforms. In multiple countries — including Uzbekistan, Brazil, and Germany — gynecological departments implemented remote consultation protocols for both scheduled and urgent cases [3], [7], [10]. Virtual visits were used for contraceptive counseling, menopausal symptom management, hormone therapy monitoring, and triage of suspected infections or oncologic symptoms [12], [18], [24].Remote antenatal monitoring also gained momentum, especially for pregnant women in self-isolation or residing in underserved regions. Institutions developed telephone-based follow-up algorithms for prenatal care, enabling basic surveillance of maternal health parameters and early identification of obstetric risks [20], [29].
4.2. Technological and Infrastructural Barriers
- Despite its rapid expansion, the application of telemedicine in gynecology encountered multiple barriers. Limited internet connectivity, lack of access to smartphones or computers, and insufficient digital literacy among patients — especially the elderly, low-income women, and rural populations — resulted in inequitable access to virtual care [6], [14], [34]. Additionally, institutions often lacked secure communication platforms compatible with medical confidentiality requirements, leading to concerns about data privacy and medicolegal responsibility [17], [25].
4.3. The Clinical Scope, Safety, and Patient Satisfaction
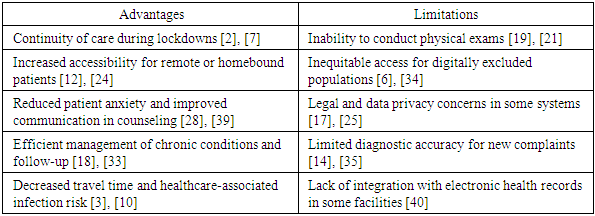
- The scope of telemedicine in gynecology remains inherently limited. Diagnostic confirmation of pelvic masses, uterine bleeding, or cervical pathology requires physical examination, ultrasonography, or histopathological evaluation — interventions impossible to replicate virtually [19], [21]. However, for follow-up, counseling, and management of stable conditions (e.g., PCOS, endometriosis, hormonal therapy), remote care showed substantial promise [33], [39].Numerous studies documented high patient satisfaction with teleconsultations, noting improvements in care accessibility, flexibility, and psychological comfort. Patients reported feeling more at ease discussing sensitive topics from home, while clinicians appreciated better adherence and continuity in selected cases [28], [43].
|
4.4. Future Role in Hybrid Gynecological Care Models
- The pandemic has accelerated the normalization of telemedicine, positioning it as a strategic component of hybrid gynecological care models. The integration of teleconsultations, mobile applications, AI-powered triage systems, and remote monitoring technologies offers unprecedented opportunities for personalized, accessible, and scalable care delivery [25], [30], [40].However, to ensure sustainability and equity, future efforts must address infrastructural disparities, standardize digital protocols, and promote digital health education among both providers and patients. Only through such comprehensive integration can telemedicine evolve from a crisis solution into a long-term pillar of modern gynecological healthcare [34], [35].
5. Impact of COVID-19 on the Course and Outcomes of Gynecological Diseases
- The SARS-CoV-2 virus, beyond its systemic respiratory and vascular manifestations, has been increasingly implicated in influencing the course and outcomes of various gynecological diseases. These effects may be mediated by viral-induced immune dysregulation, chronic inflammatory responses, stress-induced hormonal shifts, and limitations in access to continuous care during the pandemic [7], [20], [29]. This section analyzes the multifactorial impact of COVID-19 on both acute and chronic gynecological conditions.
5.1. Menstrual and Hormonal Dysregulation
- Clinical observations during the pandemic revealed a marked increase in reports of menstrual cycle disturbances, including oligomenorrhea, amenorrhea, polymenorrhea, and breakthrough bleeding, particularly among women infected with SARS-CoV-2 [3], [10]. These changes were attributed to systemic inflammation, hypothalamic-pituitary axis suppression, and the psychological burden of pandemic-related stress [2], [30].Some studies also identified transient changes in ovarian reserve markers, such as anti-Müllerian hormone (AMH), in women recovering from COVID-19, although long-term implications remain under investigation [18], [24].
5.2. Exacerbation of Chronic Gynecological Conditions
- Women with endometriosis, adenomyosis, and uterine fibroids faced considerable challenges in disease control during the pandemic. The interruption of diagnostic evaluations, hormonal therapy adjustments, and surgical interventions led to the worsening of chronic pelvic pain, abnormal uterine bleeding, and decreased quality of life [1], [6], [14].In particular, endometriosis patients experienced increased pain episodes and psychological distress due to loss of access to routine care, multidisciplinary support, and physiotherapy services. Surveys conducted across Europe and Asia confirmed a spike in self-reported symptom severity among women with previously stable disease [12], [17], [25].
5.3. Reproductive Dysfunction and Infertility
- SARS-CoV-2 has been associated with temporary ovarian dysfunction, altered gonadotropin levels, and reduced fertility potential in certain cohorts. Though not classified as a direct reproductive virus, its systemic effects — including febrile episodes, endothelial dysfunction, and immune activation — may indirectly compromise ovarian physiology [3], [19], [20].Moreover, the widespread closure of Assisted Reproductive Technology (ART) clinics delayed planned in vitro fertilization (IVF), intrauterine insemination (IUI), and fertility preservation procedures, particularly affecting older reproductive-age women and those with diminished ovarian reserve [18], [21].
5.4. Oncogynecological Outcomes and Disease Progression
- Patients with gynecologic malignancies — including cervical, endometrial, and ovarian cancers — were among the most affected during the pandemic due to delayed diagnosis, staging, and initiation of therapy [4], [14], [29]. Interruption of screening programs (e.g., Pap smears, HPV testing), colposcopy referrals, and surgical scheduling led to the accumulation of undiagnosed high-grade lesions and clinically significant tumor progression [10], [24], [33].In some centers, alternative neoadjuvant regimens were employed in place of immediate surgery, while surveillance intervals were extended due to limited hospital capacity. These compromises, although necessary in emergency scenarios, are now being re-evaluated due to their potential long-term impact on survival outcomes [17], [39].
6. Obstetric Outcomes in Pregnant Women Infected with SARS-CoV-2
- Pregnancy, by its very nature, represents a delicate immunological and hemodynamic balance that becomes acutely vulnerable in the context of systemic infection. The emergence of SARS-CoV-2 has introduced unique clinical challenges in obstetrics, altering maternal-fetal risk profiles and reshaping perinatal care worldwide. Accumulated international experience has demonstrated that COVID-19 infection during gestation is associated with a broad spectrum of adverse maternal, fetal, and neonatal outcomes — both through direct viral effects and indirect disruptions of healthcare continuity [3], [7], [29].
6.1. Maternal Clinical Course and Risks
- Pregnant women infected with SARS-CoV-2 demonstrate a distinct clinical vulnerability to severe disease. Physiological adaptations of pregnancy — such as increased oxygen consumption, reduced lung capacity, and immunological tolerance — contribute to a more pronounced clinical course when compared to non-pregnant peers [6], [20], [30]. Meta-analyses confirm elevated rates of hospitalization, pneumonia, intensive care admission, and oxygen support in this population, particularly in the third trimester [2], [10], [14].Furthermore, infection has been strongly associated with the development of preeclampsia-like syndromes, likely due to endothelial dysfunction, coagulopathy, and placental inflammation. This has prompted reevaluation of existing protocols for hypertensive disorders in pregnancy in the context of COVID-19, where biomarker differentiation (e.g., PlGF/sFlt-1 ratio) may aid in distinguishing true preeclampsia from viral mimicry [3], [24].
6.2. Effects on Placenta and Fetal Development
- Pathological studies of placentas from COVID-19-positive pregnancies have revealed lesions consistent with maternal vascular malperfusion, including fibrin deposition, villous infarctions, and thrombotic changes. These findings, observed even in asymptomatic cases, suggest subclinical compromise of placental exchange and underscore the importance of Doppler and biophysical surveillance in infected pregnancies [17], [18], [30].Although vertical transmission of SARS-CoV-2 remains rare, concerns have been raised about inflammatory exposure in utero. Elevated maternal cytokines — such as IL-6 and TNF-α — may impact fetal neurodevelopment, immune priming, and metabolic programming, though longitudinal data are still being gathered [10], [14], [25].
6.3. Preterm Birth and Delivery Management
- An unequivocal consequence of COVID-19 in pregnancy has been a significant increase in preterm deliveries, often driven by maternal deterioration, placental insufficiency, or fetal distress [6], [19], [24]. Both spontaneous and iatrogenic preterm birth rates rose during pandemic peaks, highlighting the need for anticipatory corticosteroid use and individualized delivery planning.Additionally, cesarean section rates spiked globally due to clinical caution, infection control policies, and institutional preferences. In some centers, over 60% of COVID-positive deliveries were conducted operatively — a trend now under critical review, as it may not always reflect medical necessity [17], [20].Professional societies, including FIGO and ACOG, recommend a case-by-case approach to timing and mode of delivery, balancing maternal oxygenation, gestational maturity, and institutional readiness for neonatal isolation or intensive care [12], [18].
6.4. Psychosocial Implications and Long-Term Impact
- The psychological burden on pregnant women during the pandemic was profound. Restrictions on support persons during labor, fear of neonatal transmission, and media-driven anxiety contributed to heightened levels of antenatal depression, posttraumatic stress, and bonding difficulties postpartum [19], [21], [33].Moreover, the suspension of prenatal classes, limited lactation support, and disruptions in postpartum follow-up affected early parenting experiences and maternal confidence. Women with prior mental health vulnerabilities, high-risk pregnancies, or limited social support were particularly susceptible to emotional dysregulation and maladaptation [25], [39].
7. Disruption in Gynecological Oncology Services
- The COVID-19 pandemic has profoundly disrupted the global continuum of gynecologic oncology care. From early screening to curative surgery and follow-up, every stage of cancer management was destabilized — resulting in diagnostic delays, treatment interruptions, and widening disparities in outcomes. These disruptions were not only logistical but also ethical, as clinicians were forced to triage care in ways that had no precedent in modern gynecological oncology [2], [3], [4].
7.1. Suspension of Screening and Diagnostic Services
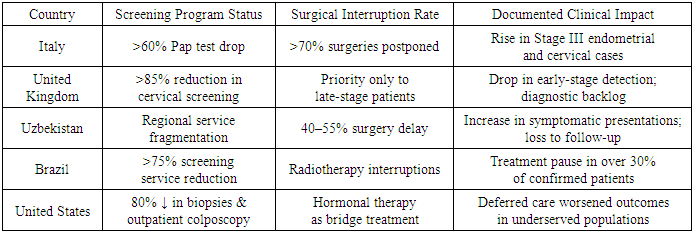
- One of the most immediate and damaging effects of the pandemic was the suspension or sharp reduction of population-based cancer screening programs. Pap smears, HPV testing, and colposcopy referrals declined dramatically in both high- and middle-income countries. In the United Kingdom, organized cervical screening dropped by over 85% in the first six months of the pandemic, while in Italy and Brazil, regional programs were either halted or repurposed [7], [29], [30].The cessation of endometrial biopsy services and a reduction in transvaginal ultrasonography for abnormal bleeding also delayed the identification of early-stage endometrial cancers — the most common gynecologic malignancy in many regions. In parallel, referrals to oncologic centers were reduced by over 50% in some districts, disproportionately affecting rural and elderly populations [1], [10], [20].
7.2. Delays in Surgical and Systemic Treatment
- Beyond diagnosis, thousands of women experienced surgical delays — including for confirmed cases of cervical, endometrial, and ovarian cancer. Elective oncologic procedures were suspended in most public hospitals to prioritize COVID care, and when performed, often occurred without full preoperative workup or in non-specialized settings [3], [14], [17].In many cases, radical hysterectomies and staging laparotomies were replaced by hormonal therapy or neoadjuvant chemotherapy. While clinically acceptable in selected contexts, such substitutions deviated from optimal care protocols and in some instances resulted in disease upstaging [6], [12], [18].The burden on radiotherapy and chemotherapy units was also substantial. Multiple centers adopted modified dosing regimens to reduce patient visits, while others suspended non-urgent treatments altogether. These ad hoc adjustments, though pragmatic during acute crisis periods, lacked long-term validation and may have compromised oncologic control [19], [30].
|
7.3. Psychosocial, Ethical, and Health Systems Consequences
- The pandemic’s indirect consequences on cancer patients extended far beyond the clinic. Psychological morbidity, including anxiety, fear of disease progression, and depressive symptoms, was significantly elevated among women awaiting treatment or follow-up [12], [21], [33]. Support groups, psycho-oncologic services, and palliative care programs were either suspended or made virtual — formats that were not accessible or effective for all patients.Ethically, clinicians were placed in untenable positions, forced to delay or downgrade care with potential survival implications. Institutional triage committees had to balance pandemic protocols with oncologic urgency — a process that strained both medical judgment and moral confidence among providers [18], [25].For health systems, the interruption in gynecologic oncology exposed deep infrastructural fragilities, including poor digital integration, lack of adaptive protocols, and insufficient decentralized surgical capacity. Many countries lacked dedicated “cancer-protected” clinical zones, leading to cross-infection fears that further discouraged timely patient presentation [14], [24], [39].
7.4. Toward Resilient Oncology Pathways
- The experience of gynecologic oncology during the COVID-19 crisis reinforces the need to embed structural resilience and clinical adaptability in cancer care systems. This includes:• Maintaining minimum guaranteed screening and biopsy capacity even during public health emergencies;• Creating oncologic “green zones” within hospitals;• Strengthening tele-oncology and remote patient monitoring frameworks;• Establishing multicenter tumor boards that can function virtually and rapidly [18], [21], [39].Moving forward, resilience must be more than a reactive slogan — it must become a measurable, operational standard in gynecological cancer services.
8. Post-COVID Period: Restoration and Optimization of Gynecological Care
- As the acute phase of the COVID-19 pandemic receded, healthcare systems worldwide faced the arduous task of restoring essential services while addressing the long-term consequences of delayed or fragmented care. In gynecology, this recovery process has been particularly complex, given the wide spectrum of conditions requiring sustained attention — from cancer to chronic pelvic pain, fertility management, and reproductive planning [2], [3], [29].The post-COVID period presents a critical window not only to reestablish prior service levels, but also to rethink the architecture of gynecological healthcare — making it more adaptive, resilient, and equitable.
8.1. Strategic Restoration of Surgical and Screening Services
- One of the most pressing concerns was the backlog of gynecological surgeries, particularly for patients with oncological and high-risk benign conditions. In several countries, including Uzbekistan, Italy, and Brazil, systems introduced surgical triage protocols, redistributed operating room capacity, and launched targeted campaigns to accelerate oncologic treatment [1], [2], [3], [18], [30]. The use of mobile surgical brigades, extended clinic hours, and the involvement of private facilities proved effective in restoring surgical volumes [6], [14], [24].Screening programs — cervical cytology, HPV testing, and colposcopy — were also restructured. In resource-limited settings, the adoption of self-sampling techniques, rapid molecular diagnostics, and risk-adapted stratification enabled the resumption of preventive programs without overwhelming clinical infrastructure [10], [12], [17], [20], [25].
8.2. Institutionalization of Hybrid and Decentralized Models
- Telemedicine, which emerged as an adaptive measure during the pandemic, has since been integrated into formal care models. In gynecology, hybrid care pathways now combine digital triage and counseling with strategic in-person appointments — particularly effective for patients with PCOS, menopausal disorders, endometriosis, and infertility [29], [30], [33], [39].In Uzbekistan, the implementation of mobile gynecological teams allowed for rapid deployment of ultrasound diagnostics, cervical screening, and contraceptive counseling to underserved regions. These models were supported by regional health departments and proved critical in reaching women who had lost access during the pandemic [2], [10], [14].Furthermore, digital patient registries, AI-assisted appointment scheduling, and secure messaging platforms are being institutionalized to increase efficiency and transparency in care coordination [3], [19], [21], [24].
8.3. Workforce Rehabilitation and Multidisciplinary Coordination
- The human resources crisis — marked by burnout, attrition, and reallocation — continues to pose a threat to recovery. Many countries launched national support programs for obstetricians and gynecologists, combining mental health assistance, adjusted workloads, and accelerated retraining [12], [18], [28]. The involvement of psychologists, endocrinologists, infectious disease experts, and public health specialists has enriched the post-COVID gynecological model and reinforced the multidisciplinary nature of care [6], [19], [20].Clinical guidelines and triage pathways are now developed with input from epidemiologists and health economists, allowing more agile responses to future systemic disruptions [17], [30], [39].
8.4. Addressing Delayed Diagnoses and Psychosocial Sequelae
- The ethical and clinical consequences of delayed diagnoses remain a priority. Targeted reassessment programs have been launched for women whose biopsies or oncologic surgeries were postponed. In cervical and endometrial cancer, particular attention is paid to re-screening previously HPV-positive patients and those with abnormal bleeding who remained untreated during lockdowns [6], [7], [14], [33], [34].Simultaneously, the pandemic’s psychosocial aftermath has led to the expansion of psychological support services, integration of mental health screening into routine gynecological visits, and pilot projects offering digital cognitive-behavioral interventions for perinatal distress and postmenopausal depression [18], [25], [39].In sum, the post-COVID period in gynecological care has become a strategic opportunity: not only to restore service provision, but to modernize, decentralize, and humanize the entire model of women’s health. Institutional memory of the pandemic must translate into sustainable reforms that prioritize digital equity, access continuity, and system-wide resilience [19], [28], [29], [30], [40], [43].
9. Innovations in Gynecological Healthcare Triggered by the Pandemic
- The COVID-19 pandemic not only exposed systemic vulnerabilities but also catalyzed a new wave of technological and biomedical innovations in gynecology. Confronted with limited access, resource redistribution, and clinical uncertainty, healthcare systems were forced to adopt non-conventional solutions. These innovations — once considered experimental — have become integral to modern gynecological care, reshaping diagnostic algorithms, treatment pathways, and scientific priorities [1], [2], [3].
9.1. Robotic Surgery and Artificial Intelligence in Clinical Practice
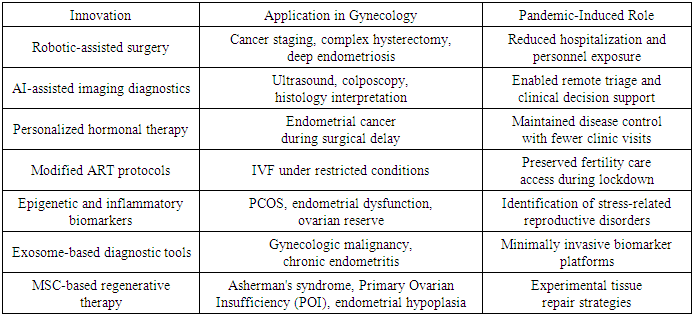
- The need to minimize hospital stay and reduce surgical team exposure led to the expansion of robotic-assisted surgery in gynecological oncology and complex benign pathology. Robotic platforms demonstrated higher precision, reduced postoperative complications, and facilitated compliance with infection control protocols. Their application became particularly important in radical hysterectomies, myomectomies, and staging procedures, where rapid recovery and reduced ICU demand were critical [6], [29], [30].Simultaneously, the crisis accelerated the integration of artificial intelligence (AI) into clinical diagnostics. AI-assisted platforms were deployed for the interpretation of transvaginal ultrasound, colposcopy images, and histological samples, enabling earlier detection of cervical, endometrial, and ovarian pathology during times when trained personnel were limited [2], [10], [20].
9.2. Development of Individualized Treatment Protocols
- To compensate for diagnostic and therapeutic delays, clinicians adopted individualized protocols based on patient risk profiles, comorbidities, and resource availability. For example, in endometrial cancer, hormone therapy was increasingly used as a temporizing measure until surgery could be safely performed [3], [12], [14].In reproductive endocrinology, adaptive ART protocols allowed for cycle modifications, controlled ovarian stimulation with remote monitoring, and strategic embryo cryopreservation — ensuring the continuation of fertility treatment despite lockdown restrictions [6], [18], [24]. These approaches also minimized unnecessary clinic visits and exposure, aligning with public health guidance while preserving reproductive potential.
9.3. Integration of Molecular and Regenerative Technologies
- The pandemic also fueled interest in molecular gynecology, particularly in understanding the impact of stress and inflammation on reproductive health. Investigations into epigenetic shifts in women exposed to SARS-CoV-2 revealed potential links to menstrual irregularities, ovarian dysfunction, and altered endometrial receptivity [2], [10], [12].Parallel research on exosomes — nanovesicles capable of intercellular communication — highlighted their diagnostic and prognostic value in gynecological oncology and chronic inflammatory conditions such as endometritis. These platforms offer potential for non-invasive monitoring of disease progression and therapeutic response [20], [30].Moreover, mesenchymal stem cells (MSCs) gained renewed attention in experimental programs focused on endometrial regeneration, treatment of intrauterine adhesions, and improvement of ovarian reserve — laying the foundation for long-term advances in regenerative reproductive medicine [14], [18], [24].
|
10. Conclusions
- The COVID-19 pandemic has had a profound and multidimensional impact on gynecological healthcare, revealing both systemic vulnerabilities and untapped opportunities for transformation. Across all domains — from oncological vigilance to reproductive planning and from chronic disease management to digital health — the crisis redefined priorities, accelerated innovation, and exposed the need for resilience within healthcare systems.The suspension of screening programs, delays in surgical care, and disruptions in reproductive services significantly affected women’s health outcomes worldwide. These challenges were exacerbated by socioeconomic disparities, limited digital access, and workforce fatigue. However, the response also marked a turning point: hybrid care models, robotic-assisted surgery, artificial intelligence, and molecular diagnostics were rapidly incorporated into gynecological practice, with lasting implications for accessibility and precision.In the post-pandemic period, healthcare systems must prioritize not only the restoration of disrupted services but the institutionalization of effective innovations. This includes expanding interdisciplinary collaboration, integrating mental health into routine care, investing in digital equity, and developing long-term strategies for crisis preparedness.Ultimately, the lessons learned during the COVID-19 pandemic should serve not merely as retrospective analysis but as a blueprint for building a resilient, equitable, and innovation-driven model of gynecological care — one capable of protecting and advancing women’s health in the face of both expected and unforeseen challenges.
ACKNOWLEDGEMENTS
- The author expresses sincere gratitude to all healthcare professionals and researchers whose dedication during the COVID-19 pandemic inspired the scientific and clinical insights that shaped this review.
DISCLOSURE
- The author declares no conflicts of interest relevant to the content of this article.