-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(5): 1424-1426
doi:10.5923/j.ajmms.20251505.23
Received: Apr. 11, 2025; Accepted: May 13, 2025; Published: May 17, 2025

Modern Trends in Diagnosis and Surgical Treatment of Liver Echinococcosis in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLParpiyev Mirziyod Mirsaitovich1, Ollabergenov Odilbek Tojiddinovich2, Terebaev Bilim Aldamuratovich2
1Doctoral Student, Department of Pediatric Surgery, Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
2Associate Professor, Doctor of Medical Sciences, Department of Pediatric Surgery, Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
Correspondence to: Parpiyev Mirziyod Mirsaitovich, Doctoral Student, Department of Pediatric Surgery, Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background. Echinococcosis is a severe parasitic disease characterized by extensive organ involvement and a long-term chronic course, leading to significant organ dysfunction. Objective. To improve diagnostic approaches and surgical treatment strategies for liver echinococcosis in children. Materials and Methods. This study analyzed treatment outcomes of 193 children aged 3 to 18 years with liver echinococcosis, treated at the Tashkent Pediatric Medical Institute from 2018 to 2024. Imaging modalities were used to determine the location and complexity of cysts. In doubtful cases, the antigen-binding lymphocyte (ABL) reaction was performed to detect residual or recurrent echinococcosis. Results. The effectiveness of surgical treatment depends on the choice of operative method and tactic. A comprehensive surgical approach including traditional or laparoscopically assisted techniques, along with albendazole (Zentel) therapy, yielded favorable outcomes. Conclusion. Long-term outcomes were assessed based on the presence or absence of complications and recurrences. The comprehensive approach allowed for effective treatment and prevention of relapses.
Keywords: Children, Liver echinococcosis, Diagnosis, Surgical treatment
Cite this paper: Parpiyev Mirziyod Mirsaitovich, Ollabergenov Odilbek Tojiddinovich, Terebaev Bilim Aldamuratovich, Modern Trends in Diagnosis and Surgical Treatment of Liver Echinococcosis in Children, American Journal of Medicine and Medical Sciences, Vol. 15 No. 5, 2025, pp. 1424-1426. doi: 10.5923/j.ajmms.20251505.23.
1. Introduction
- Echinococcosis is a parasitic disease frequently encountered in the Central Asian region. In recent decades, Uzbekistan has shown a steady increase in the incidence of liver echinococcosis among children, characterized by extensive tissue involvement and a prolonged chronic course. Early detection of the disease is particularly challenging due to the lack of specific clinical symptoms and patient complaints. In most cases, echinococcal cysts are identified incidentally during routine radiological or ultrasound screenings conducted in preschool and school institutions.Despite improvements in diagnostic quality and the development of new surgical techniques, complications such as suppuration and rupture of hepatic cysts, persistent residual cavities following cyst removal, and disease recurrence continue to raise concerns among specialists in determining the most effective treatment strategy.Timely and accurate diagnosis of liver echinococcosis in children, the selection of optimal surgical approaches for solitary, multiple, and complicated forms, as well as the application of effective anthelmintic therapy remain critical topics of discussion and research. These issues highlight the presence of unresolved clinical and scientific questions [2,3,4,6,7,10,13].Currently, ultrasound examination (US) plays a central role in the diagnosis of liver echinococcosis. Literature data suggest that the diagnostic accuracy of ultrasound in detecting hepatic echinococcosis ranges between 74% and 97%. Key ultrasound features include hypoechoic lesions, peripheral hypoechoic rims, daughter cysts, posterior wall enhancement, and the double-contour sign of the cyst wall.Compared to ultrasound, multislice computed tomography (MSCT) offers superior resolution, particularly for the differential diagnosis of cystic and focal liver lesions. MSCT is commonly used in cases of multiple echinococcosis or complications such as cyst rupture into the peritoneal cavity or bile ducts [3,5,8,11].Surgical treatment remains the only radical and effective method for managing liver echinococcosis in children. The most frequently described radical procedures include ideal echinococcectomy and pericystectomy, ranging from partial (contact-margin) to total resection. However, ideal echinococcectomy is rarely performed (approximately 3%) and only under specific conditions due to the risk of cyst rupture and peritoneal dissemination.Closed echinococcectomy remains the preferred surgical approach for medium and large cysts. There is ongoing debate regarding liver resection as a treatment option, as some researchers argue it is a radical procedure that prevents recurrence, while others highlight its high trauma and potential for recurrence (5–36%), regardless of surgical technique [1,2,3,9,12].These findings clearly demonstrate the relevance of liver echinococcosis in children and underscore the need for further research into its diagnosis and surgical management.
2. Methods
- From 2018 to 2024, 193 pediatric patients with hepatic echinococcosis (age 3–18) were treated at the Pediatric Surgery Department of the Tashkent Pediatric Medical Institute. Of these, 15 patients (7.8%) presented with recurrent disease.Cysts were localized in the right hepatic lobe in 150 (77.7%) cases, the left lobe in 17 (8.8%), and both lobes in 26 (13.5%). Solitary cysts were identified in 114 (59.1%) cases and multiple cysts in 79 (40.9%). Most cysts were located in liver segments V–VII, ranging from 50–100 mL in volume.Complications were noted in 35 (18.1%) cases, including suppurated/dead cysts (28 patients, 14.5%), rupture into the peritoneal cavity (3 patients, 1.6%), and obstructive jaundice due to compressive cysts (4 patients, 2.1%).
3. Results and Discussion
- The use of imaging techniques at all stages of the diagnostic and therapeutic process significantly contributed to selecting optimal surgical or conservative treatment strategies and enhanced the overall effectiveness of management. In uncertain cases involving patients with multiple liver echinococcosis or those previously operated on elsewhere, the antigen-binding lymphocyte (ABL) reaction with echinococcal antigen was utilized to detect residual or recurrent disease in its early stages. The ABL test yielded positive results in all such patients, corresponding to high serum titers (1:64). In cases of residual echinococcosis, titers were even higher, indicating cellular sensitization and the presence of antibodies against the echinococcal cyst fluid antigens.All children admitted to the clinic with liver echinococcosis underwent surgery after individualized preoperative preparation, depending on the severity of their condition and the nature of any complications. The choice of echinococcectomy technique was based on the location, size, and complexity of the cysts.A consistent surgical strategy was followed, involving echinococcectomy regardless of cyst size, multiplicity, or complications, both cyst-related and hepatic. Traditional echinococcectomy was performed in 172 patients (89.1%), while laparoscopically-assisted echinococcectomy was conducted in 21 patients (10.9%). The only difference between these approaches was the method of cyst removal—closed or semi-closed with drainage.The closed echinococcectomy method involved eliminating the parasite cavity by suturing the fibrous capsule to prevent residual cavity formation. Capitonnage was performed using either the Delbet technique or figure-of-eight layered sutures (figure 1).
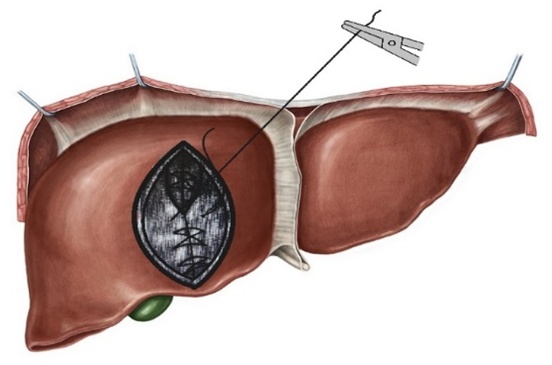 | Figure 1. Schematic representation of capitonnage using layered figure-of-eight sutures |
4. Conclusions
- Surgical treatment combined with intraoperative cyst cavity sterilization and targeted antiparasitic therapy is essential for preventing recurrence and achieving cure in children with liver echinococcosis. Our results demonstrated preserved liver function postoperatively and no recurrences. A comprehensive approach ensures favorable short- and long-term outcomes.