-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(5): 1379-1383
doi:10.5923/j.ajmms.20251505.13
Received: Apr. 15, 2025; Accepted: May 3, 2025; Published: May 8, 2025

Diagnosis and Choice of Treatment Tactics for Payre's Syndrome in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRakhmatullaev Akmal Abadbekovich , Terebaev Bilim Aldamuratovich , Majidov Temur Xamidovich
Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Payr’s syndrome is a rare but clinically significant condition associated with abnormal fixation and elongation of the transverse colon, leading to chronic abdominal pain and colostasis in children. Due to the non-specific symptoms, timely diagnosis and appropriate surgical tactics remain a challenge in pediatric practice. Materials and Methods: This study analyzed 83 pediatric patients (52 girls, 31 boys) aged 4–18 years with diagnosed Payr’s syndrome treated at the Tashkent Pediatric Medical Institute between 2018 and 2024. Diagnostic methods included abdominal Doppler ultrasound, irrigography, virtual colonoscopy, and colonoscopy. Colon elongation was quantified using segmental length coefficients (L1 in contrast-filled and L2 in contrast-evacuated colon). Treatment tactics included conservative therapy (41 patients), laparoscopic intervention (34), and open resection with end-to-end anastomosis (8). Patient complaints, colon anatomy, and function were thoroughly evaluated. Results: Constipation alone was observed in 39.8% of cases, pain with constipation in 43.4%, and isolated abdominal pain in 16.9%. Segmental analysis revealed significant elongation of the transverse colon (P<0.01). Based on elongation coefficients, laparoscopic correction was performed for moderate elongation (L = 0.8–1.0), while open surgery was indicated for severe elongation (L < 0.8). Postoperative outcomes assessed with a custom scoring scale were good or satisfactory in 88.1% of cases. Conclusion: A standardized diagnostic protocol and use of colon elongation coefficients improve the selection of optimal surgical tactics in children with Payr’s syndrome. The introduced outcome assessment scale provides an objective tool for evaluating postoperative results and guiding further care.
Keywords: Payr’s syndrome, Children, Colon elongation, Chronic constipation, Surgical treatment
Cite this paper: Rakhmatullaev Akmal Abadbekovich , Terebaev Bilim Aldamuratovich , Majidov Temur Xamidovich , Diagnosis and Choice of Treatment Tactics for Payre's Syndrome in Children, American Journal of Medicine and Medical Sciences, Vol. 15 No. 5, 2025, pp. 1379-1383. doi: 10.5923/j.ajmms.20251505.13.
Article Outline
1. Introduction
- Currently, one of the pressing issues in gastroenterology and pediatric surgery is the diagnosis and treatment of chronic colostasis and abdominal pain syndrome of the large intestine. According to the authors, chronic abdominal pain occurs in 10–17% of children under the age of 15. In addition, up to 10–40% of children with gastrointestinal diseases suffer from constipation. The prevalence of these pathologies represents a significant medical and social problem in the population.Payr’s disease, resulting from abnormal fixation of the colon, leads to traction, ischemia, and the development of pathological connective tissues [1,4,9,10,13,15].According to the literature on Payr’s syndrome, 45–65% of patients suffer from abdominal pain, and colostasis is observed in 40% of cases. The main diagnostic methods for detecting Payr’s syndrome are contrast-enhanced irrigography, CT, and MRI. One of the characteristic radiological signs in irrigography is a high position of the splenic flexure of the transverse colon and the appearance of “Payr's double-barrel colon” together with the descending segment [2,3,7,11,16].Various approaches to the surgical treatment of Payr’s syndrome are described in the literature. Among them is the dissection of the phrenocolic and splenocolic ligaments to correct the high position and sharp angle of the splenic flexure. Other scientific reports indicate that the pain syndrome becomes more severe with age. Therefore, early surgical intervention is recommended to prevent excessive dilation of the ascending and transverse colon and the development of reflux ileitis [5,6,8,12,14].Thus, the development of a unified approach to the diagnosis and treatment of Payr’s syndrome is considered relevant.Objective: To improve the diagnosis and treatment outcomes of Payr’s syndrome in children.
2. Materials and Methods
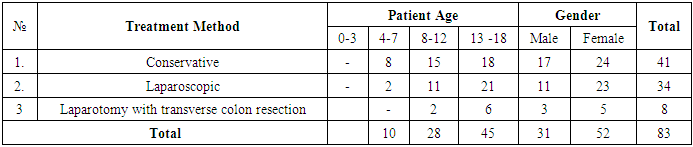
- Between 2018 and 2024, a total of 83 patients aged 4 to 18 years diagnosed with Payr’s syndrome were treated at the clinic of the Tashkent Pediatric Medical Institute. Among these, 52 (62.7%) were female, and 31 (37.3%) were male. The majority of the patients—45 individuals (54.2%)—were between 13 and 18 years old. In 41 cases (49.4%), the patients were diagnosed with the compensated stage of Payr’s syndrome. These patients underwent conservative treatment methods based on the standardized “Guidelines for the Diagnosis and Treatment of Payr’s Syndrome.” Of the remaining 42 patients, 34 underwent laparoscopic correction of the acute splenic flexure of the colon, addressing the abnormal intestinal positioning through minimally invasive surgical intervention. In the other 8 patients, a traditional laparotomy was performed to shorten the length of the transverse colon, followed by an “end-to-end” anastomosis to restore intestinal continuity (see Table 1).
|
3. Analysis of Clinical Presentation and Diagnostic Methods
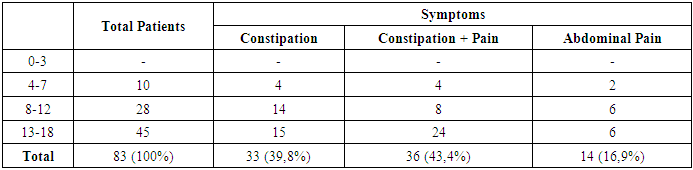
- An analysis of the reasons for patients’ initial visits to the clinic revealed that 33 patients (39.8%) primarily complained of constipation. In 36 patients (43.4%), both abdominal pain and constipation were simultaneously observed. The remaining 14 patients (16.9%) reported abdominal pain as the sole symptom. These findings are presented in Table 2.
|
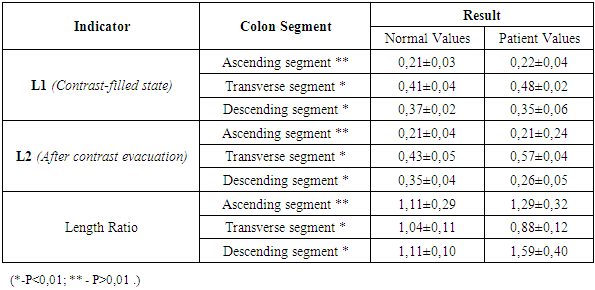
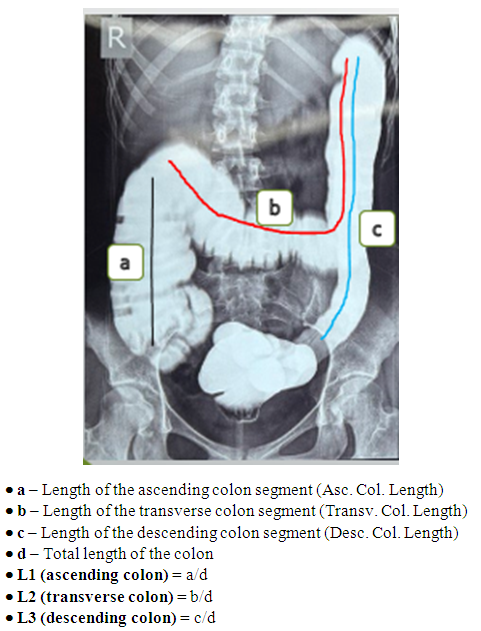 | Figure 1. Relative length coefficients of the colon segments in a contrast-filled state |
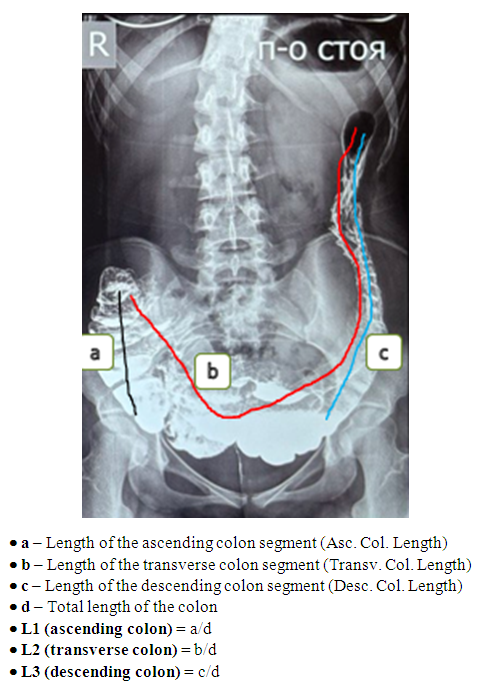 | Figure 2. Relative length coefficients of the colon segments after contrast evacuation |
4. Results
- By dividing the average L1 values obtained while the colon was filled with contrast by the average L2 values recorded after the colon was emptied, we determined the colon elongation coefficient. This analysis enabled us to assess the evacuatory function of the colon, the degree of elongation of the transverse colon, and the prominence of the “double-layer sign” characteristic of Payr’s syndrome. Using these calculated coefficients, we evaluated critical parameters for determining the colon’s functional status and choosing the optimal surgical method, as well as identified internal anatomical alterations of the colon and their clinical significance. These analyses play a vital role in understanding the structure of the colon, identifying influencing factors, and setting precise criteria for surgical planning (see Table 3).
|
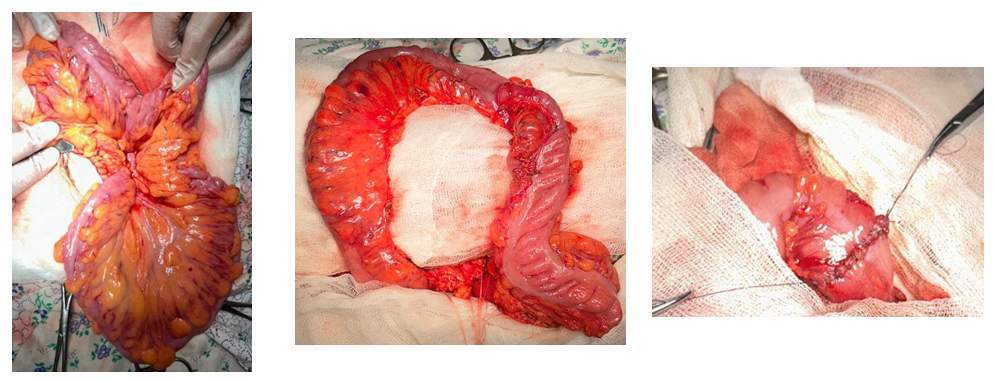 | Figure 3. Resection of the transverse colon and application of an “end-to-end” anastomosis |
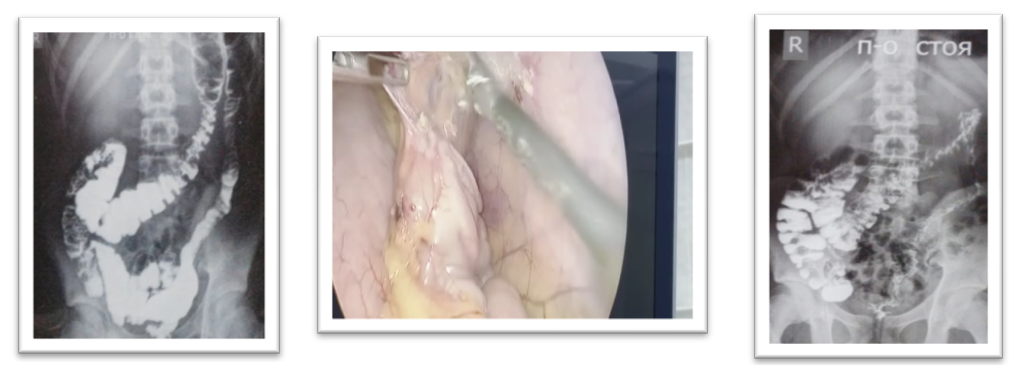 | Figure 4. Laparoscopic separation of the splenic flexure from pathological adhesions and fibrous bands. Preoperative and postoperative irrigograms |
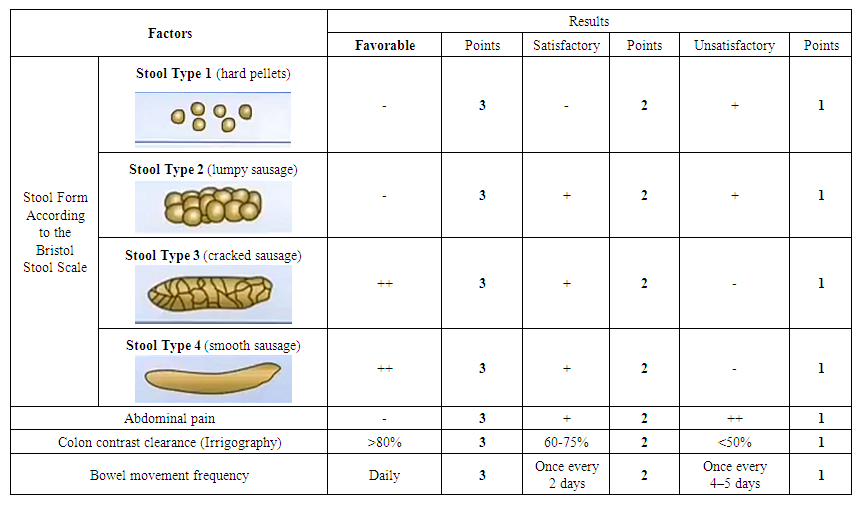 | Table 4. Scale for Analyzing Surgical Outcomes in Children with Payr’s Syndrome |
5. Conclusions
- Thus, the primary specialized diagnostic methods for detecting Payr’s syndrome in children include ultrasonography of the mesenteric veins of the colon, irrigography, virtual colonoscopy, and traditional colonoscopy. When selecting the appropriate treatment method, determining the colon length coefficient via irrigographic imaging holds critical importance. Additionally, the developed Scale for Analyzing Surgical Outcomes in Payr’s Syndrome provides an accurate and objective means of evaluating postoperative results in patients, ensuring a comprehensive assessment of their functional recovery.