-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(5): 1364-1368
doi:10.5923/j.ajmms.20251505.10
Received: Apr. 9, 2025; Accepted: Apr. 28, 2025; Published: May 8, 2025

Gender Differences in the Prevalence of Arterial Hypertension Among Adolescents and Medical Students: Evidence from a Population-Based Study in the Fergana Valley
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLZamira Makhmudzhanovna Khashimova 1, Nematjon Soliyevich Mamasoliyev 2, Kurbanova Rano Rustambekovna 3
1Assistant, Department of Pediatrics, Faculty of Advanced Medical Training, Andijan State Medical Institute, Andijan, Uzbekistan
2MD, Professor, Academician, Head of the Department of Internal Medicine, Faculty of Advanced Medical Training, Andijan State Medical Institute, Andijan, Uzbekistan
3Candidate of Medical Sciences, Associate Professor, Department of Internal Medicine, Faculty of Advanced Medical Education, Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Zamira Makhmudzhanovna Khashimova , Assistant, Department of Pediatrics, Faculty of Advanced Medical Training, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective: To examine gender and age differences in the prevalence and severity of arterial hypertension (AH) among adolescents and medical students in the Fergana Valley, considering behavioral and sociocultural factors. Materials and Methods: A population-based, cross-sectional study of 2,502 participants aged 11–22 years (1,371 adolescents, 1,131 students) was conducted. Blood pressure (BP) was measured following AHA/ACC 2017 and ESC/ESH 2018 guidelines. Behavioral factors (smoking, physical activity, BMI) were assessed via standardized questionnaires. Statistical analysis included chi-square tests, t-tests, and Pearson correlations. Results: Significant gender- and age-related differences were found. Adolescent girls more frequently had isolated Stage I diastolic hypertension, while male students showed higher rates of Stage II systolic and diastolic hypertension (p < 0.05). Elevated BMI, smoking, and low physical activity correlated with increased BP, particularly among males. A decline in normal BP prevalence with age, especially among males, was observed, influenced by sociocultural factors like academic stress. Conclusion: Male sex and age progression increase hypertension risk. Early, gender-sensitive screening, physical activity promotion, nutritional counseling, and smoking prevention in educational settings are crucial. Public health strategies should consider local sociocultural contexts to optimize prevention efforts.
Keywords: Arterial hypertension, Adolescents, Students, Gender differences, Behavioral risk factors, Prevention, Fergana Valley
Cite this paper: Zamira Makhmudzhanovna Khashimova , Nematjon Soliyevich Mamasoliyev , Kurbanova Rano Rustambekovna , Gender Differences in the Prevalence of Arterial Hypertension Among Adolescents and Medical Students: Evidence from a Population-Based Study in the Fergana Valley, American Journal of Medicine and Medical Sciences, Vol. 15 No. 5, 2025, pp. 1364-1368. doi: 10.5923/j.ajmms.20251505.10.
1. Introduction
- Arterial hypertension (AH) has emerged as a significant public health concern among adolescents and young adults, with early onset contributing to increased risk of chronic cardiovascular diseases (CVD) later in life [1]. According to the World Health Organization, up to 80% of non-communicable diseases can be prevented through early identification and management of modifiable risk factors such as elevated blood pressure [2]. As elevated blood pressure during youth often tracks into adulthood, understanding the epidemiological patterns and associated risk factors is critical for developing effective preventive strategies [3,4].Recent global meta-analyses estimate that the prevalence of hypertension among adolescents ranges between 4% and 6%, with increasing trends observed over recent decades [11,22]. Notably, studies from China and other Asian countries report similar findings, highlighting regional differences influenced by sociodemographic factors and lifestyle behaviors [18].Gender differences in blood pressure trajectories have gained attention in the last decade. Evidence indicates that boys are more likely to develop elevated systolic and diastolic blood pressure during adolescence and early adulthood compared to girls [8,9,19]. Hormonal differences, such as the impact of testosterone on sympathetic nervous system activity and vascular tone regulation, partially explain these patterns [13]. Additionally, boys are more prone to engage in risk behaviors including smoking, reduced physical activity, and unhealthy dietary habits, which further exacerbate hypertension risk [5,17,21].Conversely, girls tend to adopt healthier lifestyles, maintain higher levels of physical activity, and exhibit better adherence to dietary guidelines, contributing to lower hypertension prevalence during adolescence [9]. However, isolated diastolic hypertension has been observed more frequently among adolescent girls, suggesting different pathophysiological mechanisms influenced by hormonal and autonomic factors [14].Emerging research emphasizes the role of behavioral and environmental factors in shaping blood pressure patterns. Sedentary behavior, poor diet, and academic stress during the transition to university life have been linked to increased hypertension risk among youth [16,21]. Systematic reviews underline the strong association between reduced physical activity and elevated blood pressure levels among adolescents, further reinforcing the need for lifestyle interventions [21].International guidelines, including the 2023 recommendations for hypertension management in children and adolescents, call for early detection and intervention strategies tailored to specific risk profiles, including gender differences [20]. Despite extensive research globally, there remains a scarcity of population-based studies examining gender-specific hypertension trends among adolescents and university students in Central Asia, particularly in Uzbekistan [14,15].Given the importance of early identification of at-risk groups and the need for targeted preventive measures, this study aims to assess gender differences in the prevalence and severity of arterial hypertension among adolescents and medical students in the Fergana Valley. The findings are expected to inform the development of gender-sensitive public health strategies to reduce the burden of cardiovascular diseases in this vulnerable population.
2. Materials and Methods
- This population-based, cross-sectional study was conducted between 2021 and 2023 in the Fergana Valley region of Uzbekistan. The study sample consisted of 2,502 participants, including 1,371 adolescents (schoolchildren aged 11–17 years) and 1,131 medical students (aged 18–22 years). A stratified cluster sampling method was used to ensure proportional representation by age, sex, and area of residence (urban vs. rural).Blood pressure (BP) measurements were performed using validated automated oscillometric devices after a 5-minute rest in a seated position. Three readings were taken at 2–3 minute intervals, and the average of the last two values was used for analysis. Classification of BP levels was based on the American Heart Association/American College of Cardiology (AHA/ACC, 2017) and European Society of Cardiology/European Society of Hypertension (ESC/ESH, 2018) guidelines, with age-appropriate percentile-based thresholds.Each participant completed a standardized questionnaire, which included items on behavioral and demographic factors: smoking status, alcohol consumption, physical activity level, dietary habits, family history of hypertension and cardiovascular diseases, and self-perceived health status. Anthropometric parameters, including height, weight, and body mass index (BMI), were also assessed.All data were analyzed using SPSS software (version XX). Descriptive statistics were used to characterize the sample. Chi-square (χ²) tests were applied to assess differences in categorical variables, and Student’s t-test was used for continuous variables. Pearson correlation coefficients were calculated to explore associations between blood pressure levels and relevant risk factors. A p-value of <0.05 was considered statistically significant.
3. Results
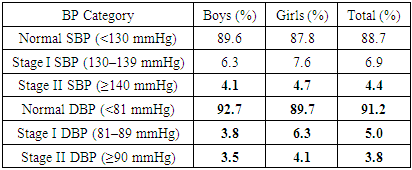
- The study population consisted of 2,502 participants, with nearly equal gender distribution: 1,254 males (50.1%) and 1,248 females (49.9%). Participants were grouped into adolescents (11–17 years) and medical students (18–22 years). The analysis of arterial blood pressure (BP) according to AHA/ACC (2017) guidelines revealed clear gender- and age-related differences in prevalence, severity, and patterns of hypertension.Among the adolescent group, systolic and diastolic blood pressure values varied by gender, though the majority of both boys and girls had BP within the norm. However, significant differences were noted in the distribution of elevated BP categories, especially for diastolic values.
|
|
4. Discussion
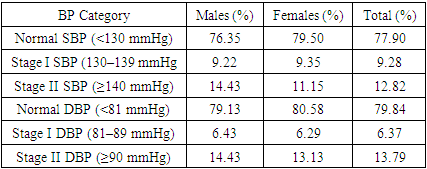
- This study provides valuable insights into gender- and age-specific differences in the prevalence and severity of arterial hypertension among adolescents and university students. Our findings are consistent with previous research suggesting that males, especially in late adolescence and early adulthood, are at greater risk for developing elevated blood pressure and more severe hypertension stages [8,9,18].Several factors may underlie the higher prevalence of Stage II hypertension among male students compared to females. Biological mechanisms, including the effects of testosterone on sympathetic nervous system activity, endothelial function, and sodium retention, are likely contributors [13,19]. Additionally, behavioral patterns observed in our study sample reinforce these findings: male participants exhibited higher rates of smoking, lower levels of physical activity, and a higher mean body mass index (BMI) compared to females [17,21]. These behaviors are known to exacerbate hypertension risk and likely accelerate progression from Stage I to Stage II hypertension.Our data also revealed that adolescent girls exhibited a higher prevalence of isolated diastolic hypertension at Stage I. This pattern is consistent with previous observations suggesting that hormonal fluctuations during puberty, differences in autonomic nervous system balance, and early vascular tone dysregulation contribute to diastolic blood pressure elevation in females [14].An important age-related trend was the sharp decline in the proportion of individuals with normal blood pressure as participants transitioned from adolescence to early adulthood. This trend was particularly pronounced among males, indicating the cumulative effect of unfavorable behavioral and environmental factors during this critical life stage. Sociocultural factors, including increased academic stress, changes in dietary habits, reduced physical activity during university years, and high rates of smoking among male students in the Fergana Valley, may also contribute significantly to the observed patterns [16,22].The cross-sectional design of our study limits the ability to infer causality; however, the associations observed are consistent with established physiological and behavioral risk profiles. While blood pressure measurements were performed according to standardized protocols [20], the reliance on single-visit assessments may introduce measurement variability. From a public health perspective, these findings underscore the urgent need for early, gender-sensitive screening and prevention strategies. Targeted interventions addressing modifiable risk factors such as smoking cessation, promotion of physical activity, and dietary improvements should begin during adolescence and be sustained through the university period [5,7]. Furthermore, public health programs should consider the sociocultural context influencing health behaviors in this population.Future longitudinal studies are necessary to track the progression of hypertension from adolescence into adulthood and to further elucidate the gender-specific mechanisms driving these trends. Evaluating the effectiveness of gender-specific health promotion initiatives in educational settings could provide critical evidence for shaping public health policies.
5. Conclusions
- This population-based study revealed significant gender- and age-related differences in the prevalence and severity of arterial hypertension among adolescents and medical students in the Fergana Valley. Adolescent girls were more likely to exhibit isolated Stage I diastolic hypertension, while male students demonstrated markedly higher rates of Stage II systolic and diastolic hypertension. The progressive rise in blood pressure observed during the transition from adolescence to early adulthood, particularly among males, underscores the need for early, targeted intervention strategies. Our findings highlight the importance of gender-specific approaches to hypertension screening, prevention, and management.We recommend that schools and universities implement regular blood pressure screening programs beginning in early adolescence. Educational institutions should promote physical activity through structured sports programs, offer nutritional counseling to encourage healthy dietary habits, and provide smoking prevention and cessation programs targeting at-risk youth, especially males. Public health initiatives must address not only biological risk factors but also behavioral and psychosocial determinants that contribute to hypertension in youth. These interventions should be culturally adapted to the regional context of the Fergana Valley to enhance their acceptance and effectiveness.Further research is warranted to explore the long-term impact of early intervention programs on cardiovascular outcomes and to develop comprehensive, gender-sensitive public health strategies for the prevention of hypertension and related diseases among young populations.