Ollabergenov O. T. , Barotov F. T. , Uglonov I. M.
Tashkent Pediatric Medical Institute, Tashkent, Republic of Uzbekistan
Copyright © 2025 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The results of treatment of 126 patients aged 1 to 17 years with acute pleural empyema were analyzed. The effectiveness of early endoscopic interventions, such as sanitation bronchoscopy with short-term bronchial occlusion, as well as sanitation videothoracoscopy in the complex treatment of acute pleural empyema in children was assessed. The results of the conducted treatment showed high clinical efficiency of early simultaneous implementation of sanitation bronchoscopy with bronchial occlusion, as well as sanitation videothoracoscopy in the complex treatment of acute pleural empyema in children. The obtained results indicate the prospects for their widespread use, as they have high resolution and low invasiveness, prevent the development of serious complications and prevent the disease from becoming chronic.
Keywords:
Children, Acute pleural empyema, Sanitation bronchoscopy with short-term bronchial occlusion, Sanitation videothoracoscopy
Cite this paper: Ollabergenov O. T. , Barotov F. T. , Uglonov I. M. , Choice of Surgical Treatment Acute Pleural Empyema in Children, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 1301-1305. doi: 10.5923/j.ajmms.20251504.95.
1. Relevance of the Problem
Despite the successes achieved in the treatment of children with purulent-inflammatory lung diseases, this problem remains far from solved, which is largely due to the difficulty of determining the exact parameters of destructive changes in the lung tissue at various stages of the disease. An important role in this is also played by the fact that there is still no consensus on issues of diagnosis, tactics and methods of performing surgical interventions in the early stages of the disease; this factor inevitably leads to various complications and functional disorders of both the respiratory organs and the body as a whole [1,4,6]. Empyema of the pleura is a severe form of purulent-inflammatory process in the pleural cavity in children, the severity of which is due to manifestations of both respiratory failure and severe purulent intoxication. The progressive course of the disease is accompanied by inflammation of the visceral and parietal pleura, which in turn leads not only to pathological changes in the bronchopulmonary system, but also poses a serious risk of developing severe complications that put the patient's life at risk. The causative agents of diseases of the bronchopulmonary system are microorganisms and viruses; they participate in the development of suppuration processes in the lung tissue. The microbial agent enters the lungs through airborne droplets and hematogenous routes, causing pathological changes in the upper respiratory system, while local immunity is reduced and conditions are created for the penetration and reproduction of bacteria in the lower respiratory system, in particular in the lung tissue. Disruption of the microcirculation process in the lung tissue and at the level of the bronchioles leads to functional dysfunction of the entire respiratory system, which is manifested by a weakening of the drainage function of the bronchial system and leads to respiratory failure. The accumulation of pus in the pleural cavity is, in most cases, the result of infection of the effusion against the background of a severe inflammatory process of various origins. Many researchers note that despite the improvement in the quality of diagnosis and the development of new treatment methods for acute pleural empyema in children, the transition of the disease to the purulent-fibrinous stage or to the stage of fibrin organization leads to blockage of the lung drainage system, which requires its rehabilitation and puncture-draining interventions of the pleural cavity with prolonged conservative therapy and physiotherapy procedures [2,8,9,12,13,14].The widespread introduction of modern medical technologies into the clinical practice of pediatric thoracic surgery allowed the use of effective methods of bronchoscopic rehabilitation and videothoracoscopic surgical interventions in the treatment of many purulent-inflammatory diseases of the bronchopulmonary system in the early stages of their development, which in turn prevented the development of severe pulmonary pleural complications, in particular the development of acute pleural empyema [3,5,7,10,11]. Generally accepted puncture methods of treatment in children are effective only at the beginning of the disease. In the purulent-fibrinous stage of pleurisy with a long history of the disease, puncture and drainage of the pleural cavity in most cases do not give a pronounced positive effect. In the presence of negative dynamics, the absence of effect from long-term conservative treatment, the aggravation of respiratory failure due to chronic purulent intoxication and the formation of abscesses, rehabilitation of the pleural cavity, pneumolysis or lung decortication are indicated. Therefore, the early use of video thoracoscopic interventions in this patient population is more effective, as it prevents the transition of acute pleural empyema to chronic.
2. The Purpose of the Study
Improving the treatment results of acute pleural empyema in children by early bronchoscopic and videothoracoscopic rehabilitation.
3. Research Materials and Methods
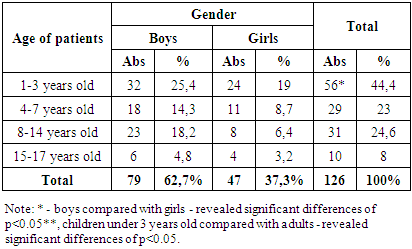
During the period from 2017 to 2024, 126 children aged 1 to 17 years with acute pleural empyema were hospitalized and treated at the Pediatric Surgery Clinic of the Tashkent Pediatric Medical Institute. The distribution of patients by gender and age is shown in Table 1.Table 1. Distribution of patients by gender and age (n=126)
 |
| |
|
In terms of age, the patients were divided into 4 groups, of which the group of patients aged 1 to 3 years prevailed, which amounted to 44.4% of children, which indicates the commitment of young children to the susceptibility of infection and early pulmonary pleural complications, which are accompanied by severe course and rapid development of acute empyema. the pleura. Depending on the prevalence of the purulent-inflammatory process in the pleural cavity, we found a significant difference in the involvement of the pathological process on the affected side, the localization of acute pleural empyema in the right lung was detected in 67 (53.2%) patients, in the left lung in 57 (45.2%), the involvement of both lungs in the pathological process was detected in 2 (1.6%) of patients (Diagram 1.).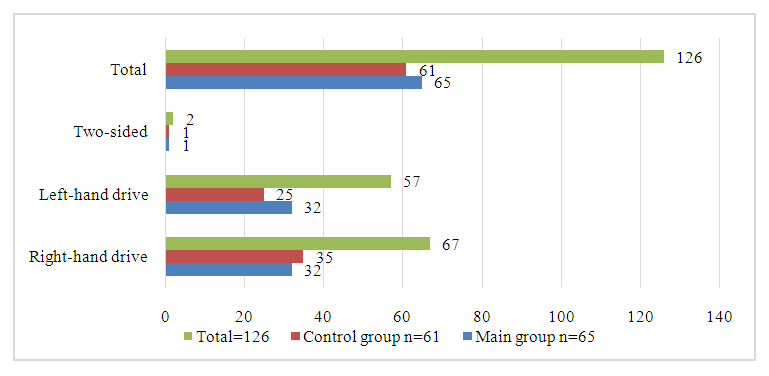 | Diagram 1. Frequency and localization of the pathological process in the lungs |
All hospitalized patients, regardless of age and duration of the disease, underwent chest X-ray examinations, ultrasound of the pleural cavity, MSCT of the chest organs, bronchoscopy and bronchography, clinical and laboratory studies and bacteriological examination of pleural effusion.
4. The Results of the Study
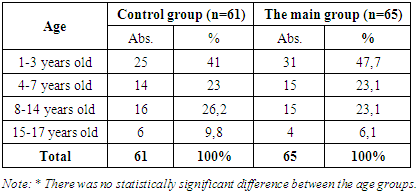
In order to conduct randomized trials over a long period of time and compare the effectiveness of surgical treatment, our patients were divided into two comparable groups. The first control group consisted of 61 (48.4%) patients who underwent punctures and drainage of the pleural cavity, as well as rehabilitation bronchoscopy (bronchoocclusion, if necessary). The second main group, 65 (51.6%) patients, consisted of patients who, in addition to punctures and drainage of the pleural cavity, rehabilitation bronchoscopy with bronchococclusion, also underwent early video thoracoscopic intervention (Table 2).Table 2. Distribution of patients with acute pleural empyema by comparison groups
 |
| |
|
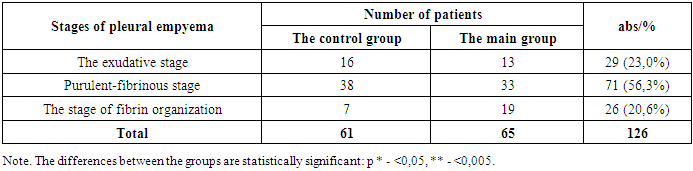
It should be noted that the determination of etiological factors and causes leading to the development of acute pleural empyema in patients contributes to the correct pathogenetic choice of tactics, timing and methods of treatment. For this purpose, purulent-inflammatory processes detected in the lung and pleural cavity were evaluated according to the generally accepted classification of thoracic surgeons of the American Association (Table 3).Table 3. Number of identified patients depending on the stage of pleural empyema (data for 2017-2024) (χ2=10,7; р<0,005)
 |
| |
|
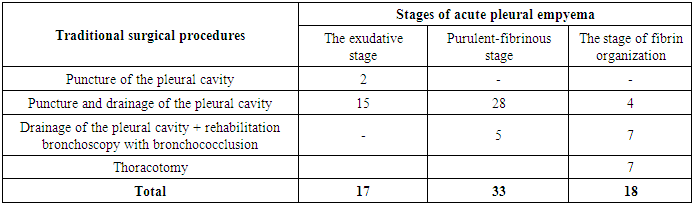
The causes of acute pleural empyema in 103 (81.7%) cases were destructive pneumonia, in 23 (18.3%) cases this was facilitated by the breakthrough of an abscess into the bronchus and pleural cavity. The number and types of primary traditional interventions performed in patients of the control group with acute pleural empyema, as well as performed rehabilitation bronchoscopy with bronchococclusion are presented in Table 4.Table 4. The number and types of traditional interventions performed in patients of the control group with acute pleural empyema
 |
| |
|
In our observations, puncture-drainage interventions of the pleural cavity were performed in 17 (27.9%) cases in patients of the control group with exudative pleurisy. In 44 (72.1%) cases of purulent-fibrinous stage of acute pleural empyema and the stage of fibrin organization, patients underwent additional bronchoscopy with bronchial occlusion in addition to puncture with drainage of the pleural cavity in 12 cases due to the presence of pyopneumothorax. At the same time, the effectiveness of puncture-drainage interventions was noted in 26 (42.6%) patients with exudative and purulent-fibrinous stages of the disease. However, in the remaining 35 (57.4%) patients of the control group, performing only puncture-drainage interventions proved to be not only ineffective, but also insufficient, which manifested itself in the progression of the purulent-inflammatory process in the bronchi and the lack of full-fledged lung aeration. Control chest X-ray and transthoracic scanning performed on 4-5 days after drainage of the pleural cavity indicated the presence of a collapsed lung on the affected side in 23 patients, which was a direct indication for sanitization bronchoscopy. In 12 patients with pyopneumothorax, rehabilitation bronchoscopy was performed with bronchococclusion, which was an obligatory component of the complex traditional treatment of acute pleural empyema (Fig. 1). | Figure 1. Short-term bronchial occlusion in pyopneumothorax |
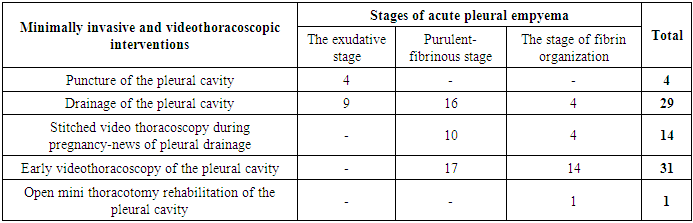
In 7 (11.5%) cases in children of the control group at the stage of fibrin organization, unsatisfactory treatment results were noted despite the differentiated approach in applying the above therapeutic tactics, since many of these patients had previously undergone minimally invasive interventions in the form of pleural drainage during primary hospitalization at their place of residence. Therefore, after preoperative preparation, these patients underwent a more technically complex operation - open thoracotomy rehabilitation of the pleural cavity, which at that time was the main surgical method of treatment in children with acute pleural empyema at the stage of fibrin organization. Improving the material and technical equipment of our clinic with high-tech equipment allowed us to introduce new modern methods of minimally invasive and endosurgical surgical interventions in the treatment of purulent-inflammatory diseases of the lungs and pleural cavity (coverage of patients from 2021 to 2025), in particular acute pleural empyema in children. During this time period, 65 (51.6%) patients of the main group underwent puncture-drainage interventions in 33 (50.8%) observations. The effectiveness of these interventions was noted in 19 (57.6%) patients, in 14 (42.4%) cases, drainage of the pleural cavity did not allow achieving full-fledged sanitation of the obstructed cavities, and therefore these patients underwent delayed (late) videothoracoscopic sanitation of the pleural cavity. Early primary videothoracoscopic surgical intervention was performed in 31 (47.7%) cases in patients of the main group with acute pleural empyema in the purulent-fibrinous stage and the stage of fibrin organization (Table 5).Table 5. The number and types of primary minimally invasive and videothoracoscopic interventions performed in patients of the main group
 |
| |
|
However, in 1 (1.5%) follow-up in a patient of the main group, due to the ineffectiveness of the above interventions, an open mini-thoracotomy of the pleural cavity was a necessary measure.The effectiveness of simultaneous bronchoscopy and videothoracoscopic interventions was significantly higher compared with puncture-drainage interventions. In the main group, 38 (32.5%) patients with purulent-fibrinous stage of acute pleural empyema underwent thoracoscopic sanitation of the pleural cavity with removal of fibrin deposits on the surface of the visceral and parietal pleural leaflets and its subsequent drainage. In 22 (18.8%) patients at the stage of fibrin organization, videothoracoscopic dissection of adhesions, emptying of non-draining purulent cavities, and lung decortication were performed (Fig. 2).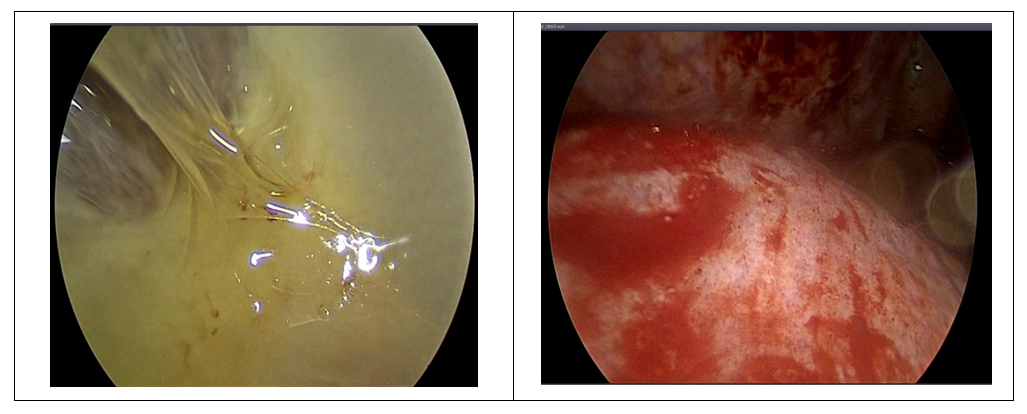 | Figure 2. Videothoracoscopic rehabilitation of the pleural cavity |
5. Conclusions
Thus, the conducted studies allowed us to conclude that bronchoscopic rehabilitation and videothoracoscopic interventions are more effective in the complex treatment of acute pulmonary empyema in children. The advantage of these techniques is minimally invasive intervention, alternative to open thoracotomy, minimizing the duration of hospitalization, and preventing the transition of the disease to a chronic form of the disease.
References
| [1] | Barova N.K. Optimization of surgical treatment of pulmonary pleural forms of acute destructive pneumonia in children: Abstract of the dissertation of the Candidate of Medical Sciences. Krasnodar, 2017. |
| [2] | Bychkov V.A., Manzhos P.I., Gorodov A.V. Basic issues of pediatric surgery. // Textbook - Moscow: RUDN Publishing House, 2011. - 328s. |
| [3] | Dronov A.F., Poddubny I.V., Kotlobovsky V.I. Endoscopic surgery in children. // M.: GEOTAR-MED, 2002. - 440s. |
| [4] | Isakov Yu.F., Dronov A.F. Pediatric surgery: a national guide // M.: GEOTAR-Media, 2009. - 1168 p. |
| [5] | Kaigorodova I.N. Videothoracoscopy in the treatment of pyofibrinothorax in children with bacterial lung destruction: Abstract of the dissertation of the Candidate of Medical Sciences. Irkutsk, 2006. |
| [6] | Kanshin A.S. Diagnosis and treatment of pulmonary pleural complications of acute destructive pneumonia using videothoracoscopy in young children: Abstract of the dissertation of the Candidate of Medical Sciences. Ufa, 2010. |
| [7] | Mamleev I.A., Gumerov P.A., Sataev V.U. and others. Videothoracoscopic treatment of pleural empyema in children. // Endoscopic surgery. - 2000. - No. 2. - p. 42. |
| [8] | Tarakanov V.A., Barova N.K., Shumlivaya T.P., Goloseev K.F., Kiselev A.N., Kolesnikov E.G. and others. Modern technologies in the diagnosis and treatment of acute bacterial destructive pneumonia in children. // Russian Bulletin of Pediatric Surgery, Anesthesiology and Intensive Care Medicine. 2015. - Vol. 5. - No. 1. - pp. 50-56. |
| [9] | Ahmed A.E., Yacoub T.E. Empyema thoracis. // Clin. Med. Insights Circ Respir Pulm Med. - 2010. - Vol. 17. - P. 1-8. |
| [10] | Avansino J.R., Goldman B., Sawin R.S., Flum D.R. Primary operative versus non operative therapy for pediatric empyema: a meta-analysis // Pediatrics. - 2005. - Vol. 115 (6). - Р. 1652-1659. |
| [11] | Cobanoglu U., Sayir F., Bilici S. et. al. Comparison of the methods of fibrinolysis by tube thoracostomy and thoracoscopic decortication in children with stage II and III empyema: a prospective randomized study. // Pediatr Rep. - 2011. - Vol. 3-29. - P. 114-118. |
| [12] | Goyal V., Kumar A., Gupta M. et al. Empyema thoracis in children: Still a challenge in developing countries. // Afr. J. Paediatr. Surg. - 2014. - Vol. (3). - P. 206-210. |
| [13] | Gupta R., Crowley S. Increasing peаdiatric empyema admissions. // Thorax. - 2006. - Vol. 61. - № 2. - P. 179-180. |
| [14] | Long Anna-May, Smith-Williams J., Mayellet S. et al. ‘Less may be best’-Pediatric parapneumonic effusion and empyema management: Lessons from a UK center. // Journal of pediatric Surgeri. -2016. -Vol. 51, N 4. - P. 588-591. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML