-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(4): 1278-1281
doi:10.5923/j.ajmms.20251504.90
Received: Mar. 22, 2025; Accepted: Apr. 23, 2025; Published: Apr. 29, 2025

Diagnosis of Speech Disorders in Children with Down Syndrome: The Role of the Speech Card in the Work of a Defectologist and Neurologist
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDjurabekova Aziza Takhirovna 1, Gulieva Parvina Ibragim Kizi 2, Azizova Sabina Fattakhovna 3
1Doctor of Medical Sciences, Professor, Head of the Department of Neurology, Samarkand State Medical University, Uzbekistan
2Doctoral Candidate at the Department of Neurology, Samarkand State Medical University, Uzbekistan
3Speech Therapist at the Clinic "Speech Therapists of Uzbekistan", Uzbekistan
Copyright © 2025 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The diagnosis of speech disorders in children with Down syndrome represents a significant challenge in clinical practice that requires a comprehensive and multidisciplinary approach. The speech assessment card serves as a crucial diagnostic and monitoring tool, facilitating systematic documentation of speech and language development patterns specific to children with Down syndrome. This standardized method enables defectologists and neurologists to evaluate articulation disorders, vocabulary limitations, grammatical difficulties, and pragmatic communication skills.
Keywords: Down syndrome, Speech disorders, Speech assessment card, Speech diagnostics, Defectology, Neurology, Interdisciplinary approach, Developmental disorders, Speech therapy, Language development, Articulation disorders, Early intervention, Diagnostic protocols, Communication skills, Cognitive development
Cite this paper: Djurabekova Aziza Takhirovna , Gulieva Parvina Ibragim Kizi , Azizova Sabina Fattakhovna , Diagnosis of Speech Disorders in Children with Down Syndrome: The Role of the Speech Card in the Work of a Defectologist and Neurologist, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 1278-1281. doi: 10.5923/j.ajmms.20251504.90.
1. Introduction
- The collaborative use of speech cards allows for more targeted therapeutic interventions, better monitoring of developmental progress, and improved coordination between specialists [1,6]. Early and accurate diagnosis through properly maintained speech assessment cards contributes significantly to the effectiveness of speech therapy, cognitive development, and overall social integration of children with Down syndrome. This approach underscores the importance of specialized diagnostic protocols that account for the unique neurophysiological characteristics of Down syndrome and supports evidence-based intervention strategies [2,7].In the early 1980s, active research was conducted in the field of diagnosis and treatment of speech dysfunctions in children with Down syndrome. In recent years, an increasing number of scientific literature sources present works on speech requirements, reasoning, and communication. For instance, in 2010, Albertini B. and colleagues conducted a study on voice timbre control: low, abnormal crying at birth, and using specific computer programs, identified the coefficient of voice timbre variation [3,8]. During the same period, Bisterveldt and colleagues determined that "the average speech intelligibility score for children with Down syndrome was 83.1% and 80% for connected speech." Many authors attribute this characteristic to anatomical and physiological disorders (deficiency and abnormality of facial sinuses, larynx). Other specialists in this field note peculiarities of the respiratory tract, such as laryngomalacia, tracheomalacia, and bronchomalacia. As seen, the problem of speech disorders is not straightforward and depends on many factors and the level of individual variability [4,9].Karmiloff-Smith and colleagues (2016), who conducted research on a large number of children with Down syndrome, discovered a phenomenon where comprehension exceeds performance organization, which manifests in lexicon, as opposed to execution technique. Accordingly, issues of language barriers in children with Down syndrome remain a priority and should be addressed through comprehensive collaboration of specialists: neurologist, speech therapist, psychologist, otolaryngologist, etc. Furthermore, the approach should not be limited to a single age range, such as early childhood, but should utilize a long-term rehabilitation program with prospects for the older adolescent period [5,10].The aim of the study is to examine and evaluate the effectiveness of the "Speech card" as a tool for diagnosing speech disorders in children with Down syndrome in the complex of defectological and neurological observation.
2. Research Material
- The research material consisted of children with Down syndrome who underwent preventive specialized examinations by neurologists, speech therapists, psychologists, and otolaryngologists at a forum organized by the MESCA Foundation - Switzerland together with doctors from Uzbekistan (September 2024). Children with Down syndrome and their parents were invited to this forum after receiving prior notification and invitation. The total number of participants was 117 children aged from 2 to 15 years; of these, urban children (Samarkand city) comprised 79 children, district children (Samarkand region) 38 children; 62 boys and 55 girls. The examination process of children with Down syndrome took place at the Multidisciplinary Clinic of Samarkand State Medical University, in the department of outpatient functional diagnostics. The inclusion criteria were based on the main principles of the research objective: speech disorder, lack of language skills, division of speech into receptivity and imagery. Consequently, from the total number of participants, children with Down syndrome were selected with an average age category of 9±2 years, having severe speech disorders and children with relatively stable speech, totaling 59 children. In the first stage, as per standard, medical history was collected, questionnaires were filled out (for parents); previous diagnostic studies were checked (based on presented documents: genetic data, previous treatment and rehabilitation, extracts from specialized educational schools); examination by a neurologist, pediatrician, psychologist, speech therapist; diagnostic research: ECG, EEG, MRI. In the second stage, children underwent testing, during which a "Speech card and development card" was compiled (jointly created by a neurologist and defectologist, approved at the department meeting). The card consists of three main sections: the first section contains 21 main points (speech character, tongue mobility, voice strength and timbre, etc.); the second section contains five points (hearing condition, speech comprehension, cognitive tasks); the third section contains eight points (speech structure, sentence formation, thinking development, etc.). For more accurate comparison of indicators, healthy children of identical age and gender were selected from among those who came for preventive examinations and provided written consent for use. All test responses were recorded and scored manually; statistical data analysis was conducted on an individual computer with standard calculation of mean values. The study also used Fisher's exact test, Student's t-test, and linear regression analysis to test differences between children with Down syndrome and healthy children.
3. Results of the Research
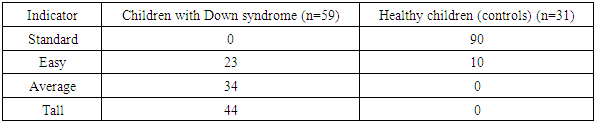
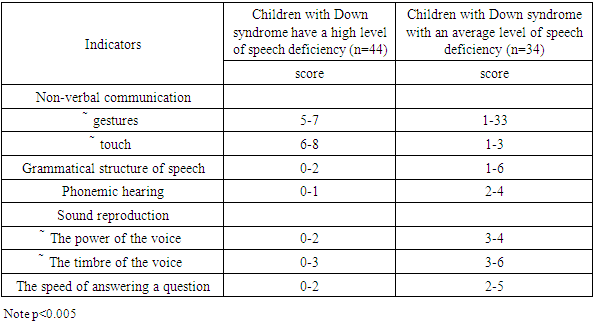
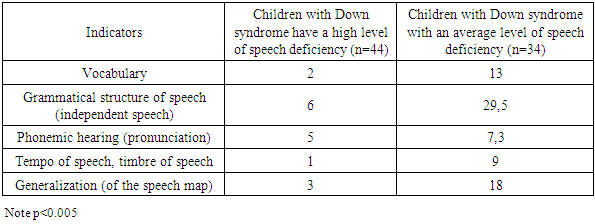
- Thus, based on the purpose and methods of the study, the indicators in the main group (children with Down syndrome) were as follows: the total number of examined children was 59, 34 boys and 25 girls. All children had common characteristics: communication through gestures, touch (especially noticeable when the child tries to express a request to their mother with a special facial expression), meaning non-verbal communication predominated over verbal. It should be noted that children with Down syndrome characteristically respond to requests-questions with short "yes" or "no" answers, so-called "black-and-white" thinking, sometimes without understanding the answer (or corresponding question). Such answers without analysis (the so-called dichotomous process) were detected in patients in 73.1% of cases. Additionally, decreased response speed, slowed thinking, and delayed answers to questions (requiring several repetitions in 56% of cases) were observed, consequently demonstrating difficulty in speech fluency, where p < 0.001 compared to the healthy group of children.As noted above, one of the research tasks in the speech card was to determine the relationship between speech skills and sound pronunciation (voice strength, speech tempo, voice timbre, sound). Each parameter was reproduced several times, and average values were determined. In one case, the patient had to repeat sounds and words after the doctor; all data were recorded in a table (which sound or word is being examined, whether the patient pronounces it in isolation, i.e., between teeth; and in which part of the word: at the beginning, middle, or end). Additionally, it was important to determine what type of disorder was present: sound or word substitution, partial substitution, or distortion. The second method involved showing a picture and asking to name what was in the picture, where the sound in words should be in different positions. A correlation was noted between speech skills and sound pronunciation in all positions, where voice strength was reduced, and considering the low speech skills, the average relationship had a limit of 5 to 6 points (normally 10 or more points). Speech tempo showed small or moderate values, on average 4 points, and when controlling non-verbal mental use from 2 to 3 points.Voice timbre and sound, when controlling correlation values, had a weak degree of significance, indicating no connection with speech skills and cognitive ability to reproduce sound. Nevertheless, the general characteristic of correlation between the four indicators affects the results in the full concept; therefore, voice strength and speech tempo (slowness) are significant for monitoring all four parameters.The evaluation of the research results according to criteria: hearing condition, understanding of surrounding speech, vocabulary, and phonemic hearing, on average, had the following values and are presented by reduced stagnation for each individually, combined with non-verbal deviation of speech skills. Thus, if hearing (biological) and understanding of surrounding speech in percentage ratio with healthy children had a lower level, only 59%, then in the position of correlation with speech skills, indicators varied within 4-6 points, which is a relatively good level, which coincides with literature data. Meanwhile, vocabulary and phonemic hearing had low values from 2 to 3 points, which is statistically significant in the general sample of the result corresponding to p<0.005. The next stage of the research was to determine the difference between emotional and impressionable character traits in combination with grammatical speech construction, thinking abilities, and the state of general and fine motor skills. To ensure comparability of variable calibration, average values were also used. Changes were revealed between the emotional property of character and differences between the level of thinking and grammatical structure of speech (Tables 1-3).
|
|
|
4. Conclusions
- Thus, the result of a study of children with Down syndrome, the topic of discussion of which was language and speech disorders, indicates a high frequency of the formation of polysyllabic speech compared with children of the same age and gender in a healthy group. In addition, a significant relationship was found between speech skills and some symptoms, such as voice strength, voice timbre, and pronunciation. A correlation has been found between hearing and phonemic hearing with understanding of the surrounding speech and grammatical structure of speech, at the same time, independent speech, imagination, and the use of speech depend little on the emotional perception and impressionable nature of patients, which are caused by cognitive insufficiency and decreased fine motor skills. Therefore, the issue of combined observation of specialists of various profiles, children with Down syndrome, remains important, where the lack of speech development and the conclusion of a speech pathologist is considered a priority as a result of forecasting and optimizing therapy. The use of a "speech card" during the examination and dynamic monitoring of patients with Down syndrome will make it possible to identify long-term projects for older adolescents.