-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(4): 1227-1230
doi:10.5923/j.ajmms.20251504.78
Received: Mar. 25, 2025; Accepted: Apr. 19, 2025; Published: Apr. 26, 2025

Aspects of Surgical Treatment of Thyroid Cysts
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMakhmudov Timur Bakhodirovich 1, Sherbekov Ulugbek Ahrorovich 2, Nazarov Shokhin Kuvvatovich 3
1PhD, Assistant, Samarkand State Medical University, Samarkand, Uzbekistan
2DSc, Head of the Department of General Surgery, Samarkand State Medical University, Samarkand, Uzbekistan
3DSc, Professor, Head of the Department of Surgical Disaeses №1 named after Academician K.M. Kurbanov SEI «Avicenna Tajik State Medical University», Dushanbe, Tajikistan
Copyright © 2025 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

We analyzed the surgical treatment of 128 patients with thyroid cysts who underwent surgery due to the presence of cysts measuring 3 centimeters or more in diameter. The surgical treatment of thyroid cysts was analyzed, indications and contraindications for this treatment method were determined, and their effectiveness was assessed. The developed algorithm allows you to choose a treatment method and management tactics for patients with thyroid cysts, depending on the size of the cyst and its morphological picture.
Keywords: Thyroid cyst, Management tactics, Surgical treatment
Cite this paper: Makhmudov Timur Bakhodirovich , Sherbekov Ulugbek Ahrorovich , Nazarov Shokhin Kuvvatovich , Aspects of Surgical Treatment of Thyroid Cysts, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 1227-1230. doi: 10.5923/j.ajmms.20251504.78.
Article Outline
1. Introduction
- Thyroid cyst (TC) refers to nodular formations of the thyroid gland with a cavity that is filled with liquid contents, determined by palpation or using imaging studies [1,3]. Thyroid cysts (nodes) can be asymptomatic for a long time, and when they increase in size, they cause “compression syndrome” of nearby neck structures, disrupting the functioning of the thyroid gland, leading to suffocation, hoarseness, difficulty swallowing and painful sensations [2,5]. A thyroid cyst is a small but common benign tumor with a cavity containing fluid. Such a lesion occurs in almost 50% of the planet's inhabitants, and in people of pre-retirement and retirement age, this pathology is considered practically the norm [4,6,7]. The most dangerous complications of cysts are inflammation and suppuration of the nodes, malignant degeneration [8,11]. Nodules of various morphological forms can develop in the thyroid gland, and most of them are benign in nature (nodular colloid goiter, adenoma, thyroid cyst [9,10]. Cysts (nodules) are the most common pathology of the thyroid gland, and in the female population it occurs 4-8 times more often [12,13]. Despite the widespread prevalence of this disease and various approaches to the treatment of this pathology, the issue of surgical tactics for managing patients with thyroid cysts, depending on their size and morphological forms, remains relevant.Purpose of the study: Conduct a factor analysis and develop an approach to surgical treatment of thyroid cysts depending on the morphological structure and size of the cyst.
2. Material and Research Methods
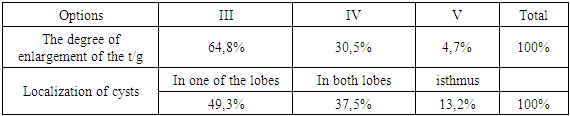
- From 2015 to 2023, 128 patients with thyroid cysts underwent surgical treatment in the surgical departments of the clinic of SamSMU and SamSMO. The age of the patients ranged from 16 to 78 years, most of the patients were of working age from 41 to 60 years. The distribution of patients by gender and age in the study groups was identical.The degree of enlargement of the thyroid gland was assessed according to the classification of Nikolaev O.V. (Figure 1), based on ultrasound and palpation of the thyroid gland. In 83 (64.8%) patients, the examination revealed III degree enlargement of the thyroid gland, 39 (30.5%) patients - IV and 6 (4.7%) - V degree. Depending on the location of the cyst, it was detected in the left or right lobe in 63 (49.3%) patients, in both lobes in 48 (37.5%) and in the isthmus in 17 (13.2%) (Table 1).
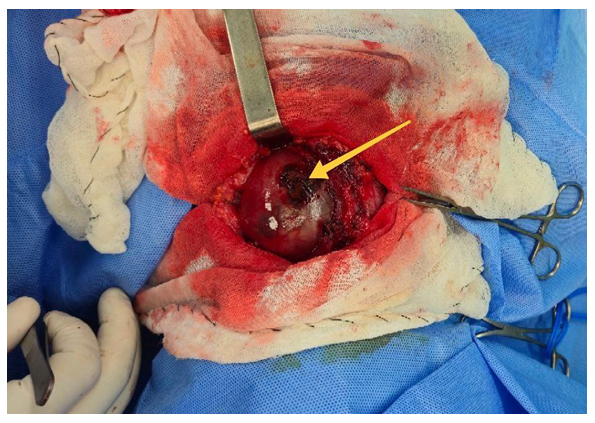
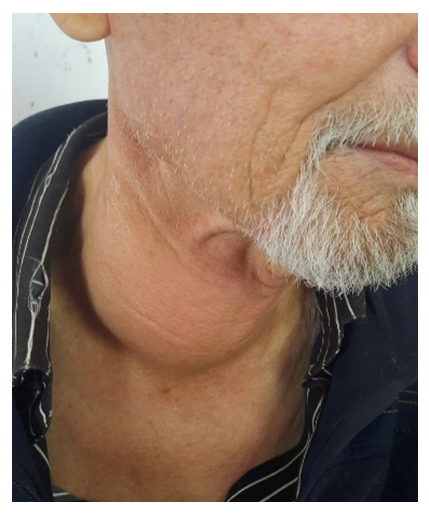 | Figure 1. Patient T., 69 years old. Stage V thyroid cyst |
|
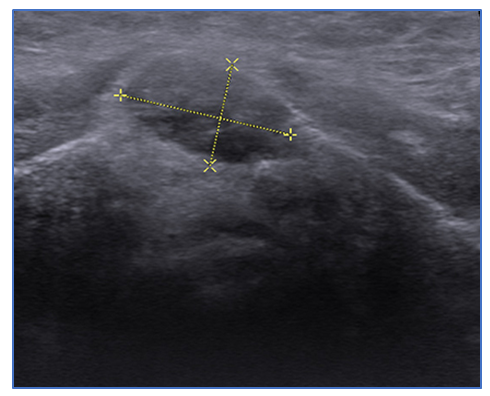 | Figure 2. Patient S., 51 years old. On the echogram, there is a cyst of the right lobe of the thyroid gland, degree II |
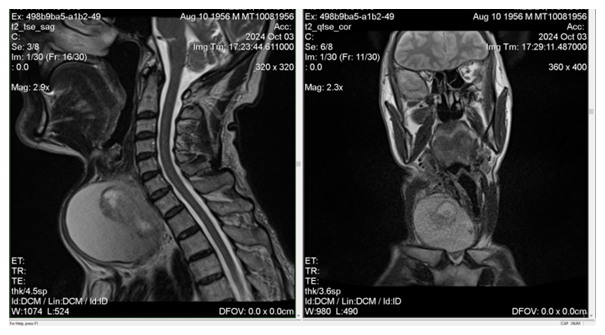 | Figure 3. Patient T., 68 years old. MRI shows a grade V thyroid cyst, with compression of the neck organs |
|
 | Figure 4. Patient Sh., 56 years old. Hemorrhage into the cyst cavity after minimally invasive treatment. An increase in the size of the cyst with symptoms of compression of the neck organs |
|
3. Results and Discussion
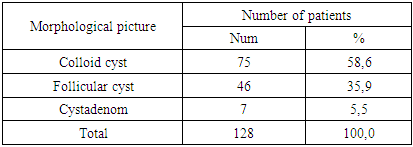
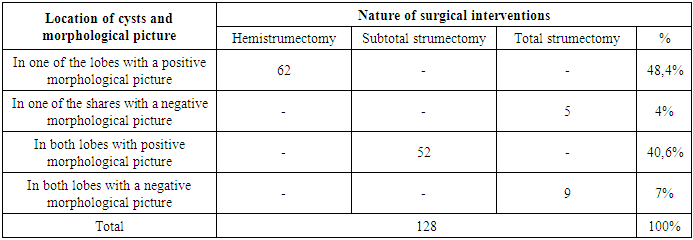
- In a group of patients who underwent surgical treatment in the period from 2015 to 2023, an analysis of the ultrasound and MRI structure of the cavity structure of the thyroid gland was carried out. Of the 128 patients in this group, 86 were diagnosed with simple cysts, and 42 with complex, multilocular formations. Analysis of histological examination of complex cavity formations showed the presence of 33.3% of cases of their malignancy.Comparative analysis of preoperative FNA with data from postoperative histological studies. The effectiveness of TAPB in patients with thyroid cysts was 89.9%.Analysis of the morphological structure showed a predominance of colloid forms of cysts (58.6%), over follicular (35.5%) and cystadenomas (5.5%), respectively.In the group of patients who underwent surgical treatment, the largest number of patients underwent hemistrumectomy (48.4%), the second most performed was subtotal strumectomy (40.6%), total strumectomy accounted for 11% of the total number of surgical interventions.Relapse of the disease was observed only in the group of patients who underwent hemistrumectomy and amounted to 3.2%.Based on our research, we have developed an algorithm for the management of patients with thyroid cysts (Table 4).
|
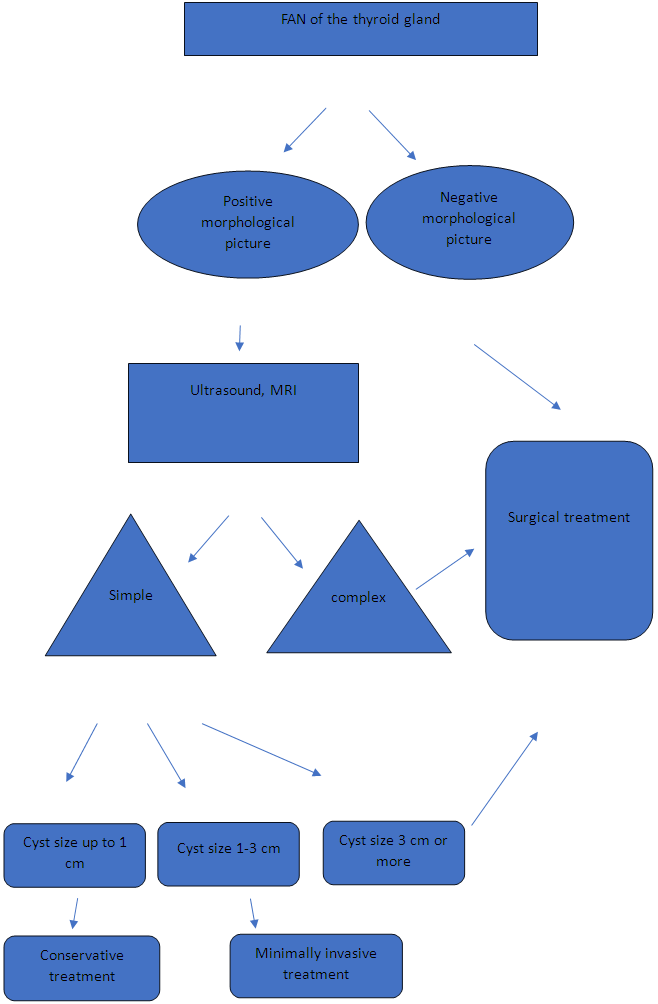
4. Conclusions
- 1. Surgical removal of thyroid cysts is the most effective and at the same time radical treatment method used in the development of cyst complications.2. Staged diagnostic and morphological studies of thyroid cysts allow you to choose the tactics of surgical intervention.3. Instrumental diagnosis of the structure of cysts allows early differentiation between simple cavitary formations and complex multi-chamber formations and choosing the optimal method of treating cysts.4. The developed diagnostic and treatment algorithm for choosing a treatment method for thyroid cysts, based on stage-by-stage diagnostic and morphological studies, has improved the results of treatment of this disease.