-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(4): 1209-1211
doi:10.5923/j.ajmms.20251504.74
Received: Mar. 29, 2025; Accepted: Apr. 20, 2025; Published: Apr. 26, 2025

Visceroptosis: Some Typological Features of Its Course
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBotirov А. K. 1, Khusanov S. М. 2, Маmajonova D. М. 3, Botirov J. А. 4
1Associate Professor, Department of Surgical Diseases, Doctor of Philosophy, Andijan State Medical Institute, Uzbekistan
2Free Applicant for the Department of Surgical Diseases, Andijan State Medical Institute, Uzbekistan
3Assistant, Department of Obstetrics and Gynecology, Tashkent Medical Academy, Uzbekistan
4Head of the Department of Surgical Diseases, Doctor of Medical Sciences, Professor, Andijan State Medical Institute, Uzbekistan
Copyright © 2025 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The authors report that visceroptosis is complicated by chronic colostasis in 30-40% of cases and is one of the most common diseases among the working-age population. Visceroptosis can manifest in various clinical forms. The prevalence rate is unknown, as only 10-20% of cases present with clinical symptoms. The authors conclude that considering typological features in visceroptosis combined with chronic colostasis can help optimize surgical tactics, leading to improved treatment outcomes.
Keywords: Visceroptosis, Chronic colostasis, Typological features, Large intestine
Cite this paper: Botirov А. K. , Khusanov S. М. , Маmajonova D. М. , Botirov J. А. , Visceroptosis: Some Typological Features of Its Course, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 1209-1211. doi: 10.5923/j.ajmms.20251504.74.
Article Outline
1. Introduction
- Visceroptosis has several synonyms (enteroptosis, splanchnoptosis, Glenard’s syndrome; from Greek σπλάγχνα – internal organs and πτῶσις – prolapse). This is a collective term referring not just to a simple mechanical descent of internal organs but to such a displacement or excessive mobility that results in subjective painful sensations and objective functional impairments in these organs [2,6].According to various researchers, visceroptosis is complicated by chronic colostasis in 30–40% of cases and is one of the most common conditions among the working-age population [5]. Visceroptosis can manifest in different clinical forms. The incidence rate is unknown, as the disease presents clinical symptoms in only 10–20% of cases. In most instances, visceroptosis is diagnosed during examinations for other symptoms [1]. Physiological prerequisites for the development of visceroptosis include individual constitutional factors, underdevelopment of the ligamentous apparatus, and incomplete fixation of the colon to the posterior parietal peritoneum [4].The aim of the study was to determine some typological features of the clinical course of visceroptosis.
2. Material and Methods of the Study
- The subject of this study comprised 132 patients with visceroptosis in combination with chronic colostasis (CC), who were undergoing inpatient treatment in the coloproctology department of the Department of Surgery and Civil Defense at the Clinic of Andijan State Medical Institute.In the clinical analysis of the studied patients, we adhered to the age classification adopted by the WHO [3].Inclusion criteria for the study: 1. age over 18 years; 2. verified diagnosis of visceroptosis in combination with colostasis (CC); 3. elective nature of the pathology; 4. absence of acute infectious and inflammatory diseases; 5. written consent from the patient and their relatives for examination and treatment.Exclusion criteria from the study: 1. combination of visceroptosis with nephroptosis or hepatoptosis; 2. urgent intestinal diseases; 3. acute cerebrovascular accidents and myocardial infarction; 4. acute infectious and viral pathology; 5. colonic tumors; 6. refusal of surgical treatment; 7. inability for further follow-up; 8. comorbid conditions in the stage of decompensation. According to the study's objectives and tasks, the patients were conditionally divided into two groups:• comparison group (2018–2022) – 85 patients (64.4%), who underwent a retrospective analysis of surgical treatment outcomes following traditional approaches.• main group (2020–2023) – 47 patients (35.6%), who underwent a prospective study of surgical treatment using an optimized surgical strategy.To achieve the study's objectives, clinical-laboratory, instrumental, and statistical research methods were conducted in accordance with the latest standard techniques, following the examination guidelines approved by the Ministry of Health of the Republic of Uzbekistan. All patients were hospitalized, examined, and operated on in a planned manner. Special attention was given to the examination of all sections of the large intestine, which helped clarify topographic data regarding the condition of the intestines.
3. Results and Discussion
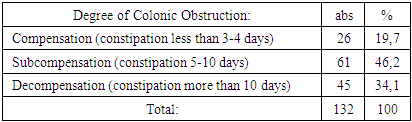
- The uniformity of the primary surgical pathology, equal conditions for providing specialized care, similarity in comorbidities and their frequency, as well as the nature of surgical interventions, allowed for the presentation of quantitative characteristics in a combined manner.An analysis of gender distribution among patients with visceroptosis combined with chronic colostasis under elective surgical conditions showed that men accounted for 28 cases (23.3%), while women constituted 104 cases (78.8%). The conducted analysis revealed that visceroptosis combined with chronic colostasis is predominantly diagnosed in females, with an average ratio of 3.7:1. This observation warranted a more detailed examination of this trend. Visceroptosis combined with chronic colostasis was most frequently diagnosed in the 45–59 age group—67 cases (50.8%), representing the most active segment of the working population, who are more exposed to external factors. Among patients aged 18–44 years, 37 cases (28.0%) were identified, largely associated with congenital developmental anomalies. Patients aged 60 and older accounted for 28 cases (21.2%), which may indicate prolonged conservative treatment before surgical intervention. In cases of visceroptosis combined with chronic colostasis, surgical intervention was performed in 42 patients (31.8%) with a disease duration of 1–5 years, including 37 women (28.9%) and 5 men (3.8%). The disease duration of 6–10 years was observed in 64 patients (48.5%), comprising 47 women (35.6%) and 17 men (12.9%). Of particular concern were patients with a disease duration of over 10 years, accounting for 26 cases (19.7%), including 20 women (15.2%) and 6 men (4.5%). To clarify the causes of visceroptosis, the body type (constitution) of the studied patients was examined. It is important to note that visceroptosis was most frequently diagnosed in individuals with an asthenic body type—84 cases (63.6%), of which 16 cases (12.1%) were men and 68 cases (51.5%) were women. Among patients with a normosthenic body type, the condition was identified in 43 cases (32.6%), including 8 men (6.1%) and 35 women (26.5%). In individuals with a hypersthenic body type, the disease was diagnosed in only 5 cases (3.8%), with 4 men (3.0%) and 1 woman (0.8%).The clinical symptom complex in visceroptosis combined with chronic colostasis consisted of general and local symptoms. Constipation, as the primary manifestation of visceroptosis, was observed in 110 patients (83.3%), while alternating constipation and diarrhea were noted in 22 patients (16.7%). A feeling of heaviness in the abdomen was reported by 102 patients (77.3%), intestinal bloating by 89 patients (67.4%), and varying degrees of pain by 127 patients (96.2%). Abdominal sagging and striae were observed in 25 patients (18.9%), diastasis of the anterior abdominal wall muscles in 9 patients (6.8%), and symptoms of intoxication (weakness, dizziness, nervousness) in 129 patients (97.7%).In cases of visceroptosis combined with chronic colostasis, we analyzed the degree of colonic obstruction, as excessively prolonged conservative treatment exacerbates the condition, affecting patients' quality of life (Table 1).
|
|
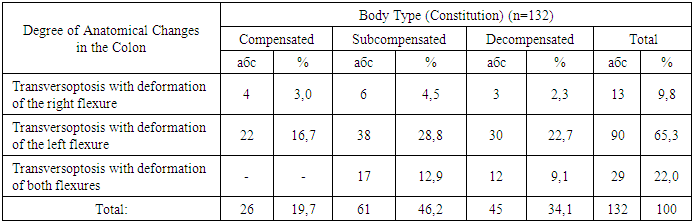
4. Conclusions
- The study identified certain typological features of visceroptosis, including a significant predominance of female patients, with a male-to-female ratio of 3.7:1, and a high incidence in middle age. Diagnosis at a young age indicates a developmental anomaly, whereas in older age, it suggests excessively prolonged conservative treatment, which exacerbates the condition. The clinical symptom complex consisted of general and local symptoms, with the primary manifestations being constipation, alternating constipation and diarrhea, as well as dyspeptic symptoms and signs of intoxication.The largest group of patients had transverse colon ptosis with deformation of the left colonic flexure 65.3% of cases. Transverse colon ptosis with deformation of both flexures was observed in 22.0%, and deformation of the right colonic flexure in 9.8% of cases. Comorbid therapeutic pathology was noted in 40.1% of cases, with cardiovascular diseases accounting for 18.9%. The analysis suggests that multiple pregnancies (cesarean section 18.9%) and large ventral hernias with diastasis of the abdominal muscles 9.8% play a role in the development and progression of visceroptosis. Thus, in cases of visceroptosis combined with chronic colostasis, considering typological features will help optimize surgical tactics, leading to improved treatment outcomes.