-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(4): 1201-1205
doi:10.5923/j.ajmms.20251504.72
Received: Mar. 30, 2025; Accepted: Apr. 23, 2025; Published: Apr. 26, 2025

Dynamics of Stress Hormone Levels with Low-Opioid Anesthesia During Thoracoplasty in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIsmailova M. U. , Ashurova D. T.
Tashkent Pediatric Medical Institute, Uzbekistan
Copyright © 2025 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The study conducted a detailed study of the quality of anesthesia when using small doses of fentanyl in combination with propofol and sevoflurane during thoracoplastic operations in children. The experiment involved 52 patients who were hospitalized with diagnoses of funnel-shaped chest deformity 2 \ -3 st Patients were divided into two groups: the group receiving anesthesia using fentanyl, propofol and sevoflurane; the group receiving anesthesia using fentanyl and propofol. During the study, the following parameters were analyzed: heart rate, average blood pressure, cortisol, triiodothyronine and thyroxine\levels.
Keywords: Opioids, Pectus excavatum, Thoracoplasty, Fentanyl, Propofol, Sevoflurane
Cite this paper: Ismailova M. U. , Ashurova D. T. , Dynamics of Stress Hormone Levels with Low-Opioid Anesthesia During Thoracoplasty in Children, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 1201-1205. doi: 10.5923/j.ajmms.20251504.72.
1. Introduction
- Pectus excavatum (PE) is the most common congenital chest wall anomaly, with an incidence of 1/400 births (0.25%). Although a specific pathological mechanism has not been established, contributing factors may include disproportionate proliferation of costal cartilages, histopathological changes in the collagen content of the costal cartilages, and abnormal posterior attachment of the diaphragm to the sternum.The defect may also be asymmetrical, often associated with rotation of the sternum and associated scoliosis. Additional factors associated with pectus excavatum include a family history of chest wall deformity and connective tissue disorders such as Marfan syndrome (up to 5% of patients). Pectus excavatum affects males four times more often than females, usually manifesting in early childhood.The etiology remains unclear, but it appears to be polygenetic and inherited in an autosomal dominant, autosomal recessive, X-linked, or sporadic manner.The defect is thought to result from unbalanced growth of the costochondral areas of the anterior thorax, resulting in symmetrical and asymmetrical abnormalities. Regardless of the etiology, CHD has an adverse impact on the lives of many patients. The most common symptoms include dyspnea (especially with exertion), exercise intolerance, and chest pain. Patients often experience embarrassment about their body image, which may lead to adverse psychological symptoms and decreased quality of life.All patients with significant CHD should undergo echocardiography, especially those scheduled for surgery, as this may reveal mitral valve prolapse, compression of the right ventricular outflow tract.Surgical interventions performed for thoracoplasty are multi-stage and highly traumatic. At the same time, general anesthesia methods must meet the requirements of reliability, low invasiveness, create adequate conditions for the work of the operating team and ensure effective, safe pain relief [9]. From this position, opioid analgesics are widely used, which have long been the leading drugs in many surgical interventions, as the "gold standard" [6]. However, excessive use of opioids is accompanied by the development of a number of negative effects and complications [1]. Inappropriate intraoperative analgesia causes chronic pain after surgery and complications. This, in turn, affects the length of the patient's stay in the hospital and the funds spent on treatment [4,7].Two drugs have become the mainstay of general anesthesia in recent decades: the opioid analgesic fentanyl and sevoflurane. The former has become the main component of many combined general anesthesia protocols [2], the latter, sevoflurane, is used to maintain and even induce general anesthesia [10]. But they can cause opioid-induced hyperalgesia during the post-administration phase. Numerous scientific studies have shown that the more opioid is administered during surgery, the more intense the post-operative secondary hyperalgesia [8].These observations have prompted the development of opioid-sparing technologies; combinations of opioid and non-opioid analgesics contribute to early patient rehabilitation and reduce treatment costs. At the same time, interest in perioperative non-opioid adjuvant drugs such as dexamethasone among others has increased, with reports of beneficial analgesic and antihyperalgesic properties that have extended to the postoperative period. Preoperative administration of dexamethasone is more effective than its intraoperative administration [3]. Dexamethasone affects the intensity of pain after surgery, reducing it, as well as the need for analgesics. The final choice of the opioid analgesic fentanyl and adequate combinations when performing general anesthesia for thoracoplasty in children is most relevant.The aim of the work is to improve the quality of anesthesia by the combined use of small doses of the opioid fentanyl in thoracoplasty in children.
2. Materials and Methods
- The study was conducted in 52 children (3-12 years old) hospitalized in the TashPMI clinic for surgical treatment for grade 2 and 3 funnel-shaped chest deformity. The objective status of the patients according to ASA corresponded to class II-III. Criteria for inclusion in the study group:- age from 3 to 12 years;- informed consent of parents for surgical intervention;Criteria for exclusion in the study group:- age of patients under 3 years and over 12 years;- patients with grade 4 funnel-shaped chest with respiratory failure;- patients with keel-shaped chest deformity.According to the plan of the conducted studies and the method of anesthesia, the patients were divided into 2 groups: Group 1 consisted of 27 (52%), who were anesthetized with fentanyl, propofol and sevoflurane; Group 2 consisted of 25 (48%), who were anesthetized with fentanyl and propofol.- Number of patients (n);- Average age of patients in years (Me) (%).
|
3. Results and Discussion
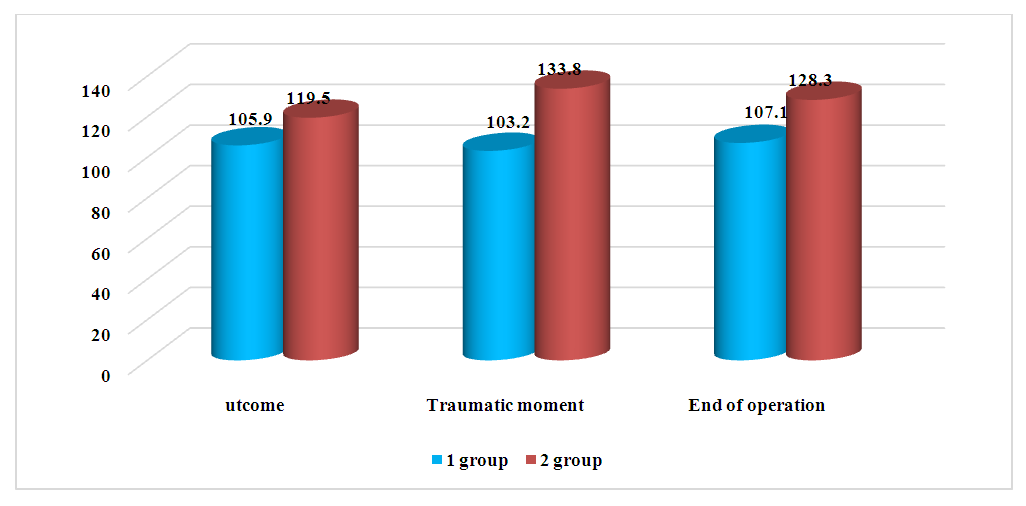
- The conducted analysis of the heart rate in children of group 1 at the stages of anes thesia and surgery, at the premedication stage, its reliable increase was noted (by 12.9% of the initial), which was considered as an insignificant increase that did not provide for correction. Already at the stage of induction into anesthesia, a more significant increase was observed (by 15% of the initial). The main stage of the operation, as the most painful, was characterized by a tendency to decrease in heart rate (by 8% of the initial), while remaining within the average physiological norms. Quite distinctive was considered the final stage of anesthesia, when the heart rate was slightly reduced (by 9.1% of the initial), but in most cases did not require deepening of anesthesia.Thus, it can be noted that the heart rate at almost all stages of surgical treatment of orthopedic pathologies in children was evenly distributed within the average physiological parameters.
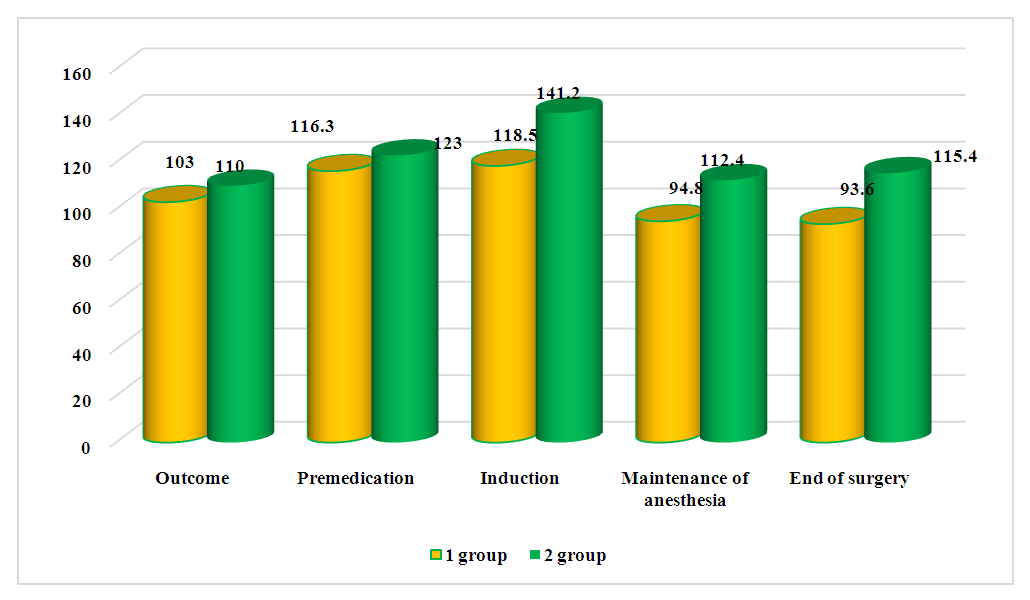 | Figure 1. Dynamics of heart rate parameters at different stages of the study |
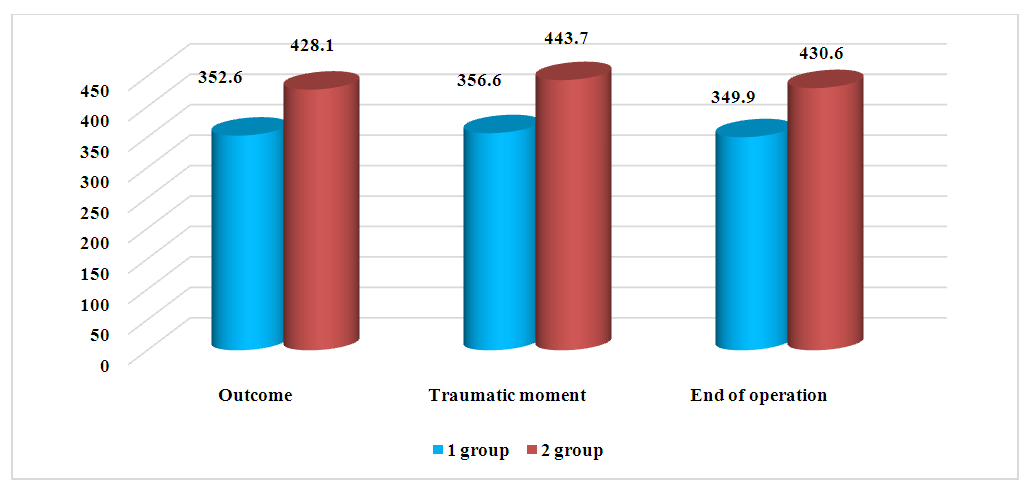 | Figure 2. Dynamics of cortisol indicators at the stages of the study |
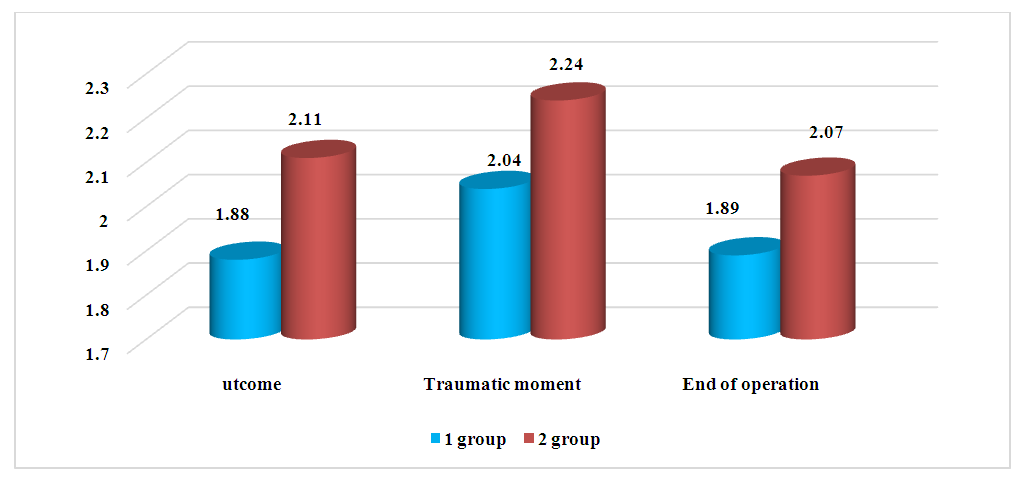 | Figure 3. Changes in T3 values at different stages of the study |
 | Figure 4. Dynamics of T4 indicators at different stages of the study |
4. Conclusions
- 1. Combined general anesthesia based on low doses of fentanyl, sevoflurane and propofol is characterized by a smooth clinical course and the preservation of stability of systemic hemodynamic parameters in children during thoracoplastic surgeries.2. Moderate increase in triiodothyronine (T3) with suppression of cortisol release at the stage of the traumatic moment of the operation confirms sufficient anti-stress protection under conditions of general anesthesia with sevoflurane, fentanyl and propofol.