-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(4): 1192-1194
doi:10.5923/j.ajmms.20251504.69
Received: Mar. 28, 2025; Accepted: Apr. 23, 2025; Published: Apr. 26, 2025

An Improved Surgical Method for Treating Knee Flexion Contractures in Children with Cerebral Palsy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhamroev Farhod 1, Eshmatov Mirlaziz 2, Kholiqov Shavkatbek 3
1DSc., Professor, Republican Children’s Neuropsychiatric Hospital, Uzbekistan
2Senior Lecturer, Andijan State Medical Institute, Uzbekistan
3PhD., Associate Professor, Andijan State Medical Institute, Uzbekistan
Correspondence to: Eshmatov Mirlaziz , Senior Lecturer, Andijan State Medical Institute, Uzbekistan.
| Email: |  |
Copyright © 2025 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article analyzes a new anatomically-based and minimally invasive surgical method for treating knee flexion contractures in children with cerebral palsy (CP). The study included 122 patients divided into two groups according to the treatment method: traditional and newly proposed. The method based on aponeurosis dissection, used in the main group, demonstrated superior clinical and functional outcomes, preserved muscle function, reduced spasticity, and accelerated rehabilitation. This technique is recommended as an effective and modern surgical approach.
Keywords: Cerebral palsy, Knee joint contracture, Aponeurosis dissection method
Cite this paper: Khamroev Farhod , Eshmatov Mirlaziz , Kholiqov Shavkatbek , An Improved Surgical Method for Treating Knee Flexion Contractures in Children with Cerebral Palsy, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 1192-1194. doi: 10.5923/j.ajmms.20251504.69.
1. Introduction
- Cerebral palsy (CP) is one of the leading neurological conditions causing disability in children. In particular, knee flexion contractures resulting from the spastic form of CP limit independent walking, complicate rehabilitation, and place a heavy burden on both families and medical staff [1,5,6].Conservative treatments (casting, orthoses, botulinum toxin injections) may provide temporary relief, but surgery is often necessary in severe and persistent cases [2,3,4]. Traditional surgical methods often involve muscle and tendon lengthening or cutting, which can sometimes lead to overcorrection, loss of balance, or reduced function. Therefore, a new anatomically and physiologically sound method involving aponeurosis dissection is being developed as a relevant direction in modern traumatology and orthopedics.
2. Materials and Methods
- The study involved 122 children with spastic CP and knee flexion contractures. They were divided into two clinical groups based on the surgical method. In the control group (n = 68), traditional methods involving muscle cutting and stretching were used. In the main group (n = 54), patients underwent a newly proposed minimally invasive surgical method based on aponeurosis dissection.All patients were evaluated preoperatively and at 3, 6, and 12 months postoperatively. Assessment included clinical examination and gait analysis (mobility, balance, knee flexion angle, muscle tone and activity, contracture characteristics). Knee joint deformities, flexion angles, bone structure, and growth points were evaluated radiographically. Electroneuromyography (ENMG) was used to assess the activity, conductivity, and spasticity of rectus femoris and hamstring muscles preoperatively and 6 months postoperatively. Spasticity was evaluated using the Modified Ashworth Scale at 3, 6, and 12 months postoperatively. Knee flexion angles were measured with a goniometer, and all data were statistically analyzed using t-tests and chi-square (χ²) tests. Results were presented as mean ± standard deviation, with p<0.05 considered statistically significant.
3. Results and Discussion
- The study confirmed that the newly developed, minimally invasive surgical method involving aponeurosis dissection provided superior clinical and functional results in children with CP and knee flexion contractures. Of 122 patients, 68 in the control group underwent traditional methods, while 54 in the main group received surgery based on the patented method “Surgical correction method for knee flexion contracture” (FAP № 02190, 17.03.2022) (see Figure 1).
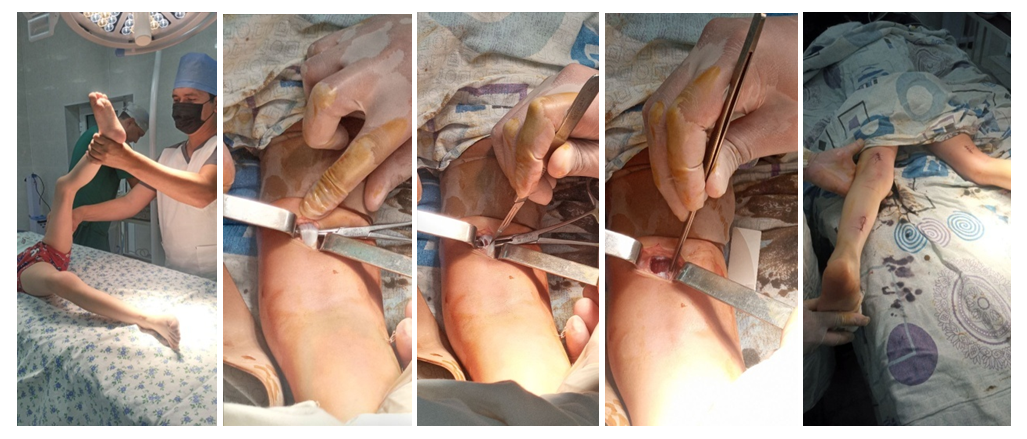 | Figure 1. Surgical correction of knee flexion contracture |
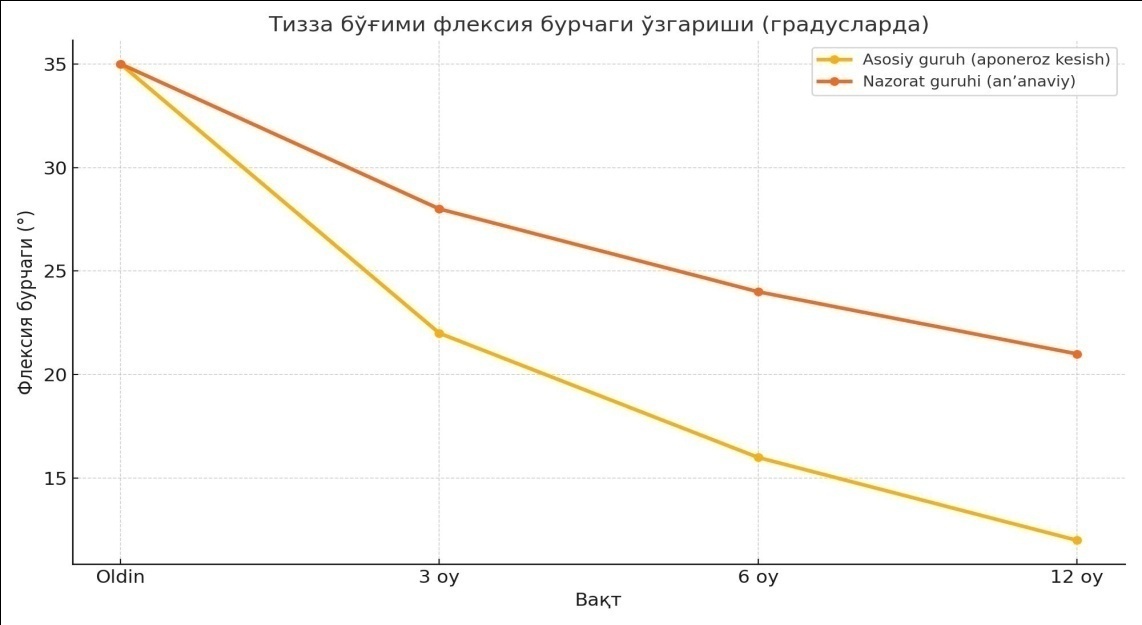 | Diagram 1. Changes in knee flexion angle post-surgery in control and main groups |
4. Conclusions
- The proposed method can be considered one of the pathogenetically justified, highly effective techniques for treating knee flexion contractures in children with cerebral palsy. By selectively dissecting the aponeurosis, preserving antagonist muscles, and applying minimally invasive techniques, this method ensures quicker recovery and improved gait. This individualized approach meets modern orthopedic and neurosurgical standards, enhances treatment outcomes, and reduces the risk of recurrent contractures.