-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(4): 1104-1107
doi:10.5923/j.ajmms.20251504.51
Received: Feb. 28, 2025; Accepted: Mar. 21, 2025; Published: Apr. 16, 2025

Traditional Treatment of Stroke at the Level of Innovation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdambaev Z. I.1, Mirjuraev E. M.2, Khalikov S. V.2
1Urgench Branch of the Tashkent Medical Academy, Uzbekistan
2Centre for Development of Professional Qualification of Medical Workers under the Ministry of Health of RUz
Correspondence to: Adambaev Z. I., Urgench Branch of the Tashkent Medical Academy, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

We examined 120 patients in the early rehabilitation period of ischaemic stroke. There were 73 men and 47 women. The average age of the patients was 61.6±0.9 years in men and 61.4±1.4 years in women. The patients were divided into 2 groups: main group (MG) - 80 patients and control group (CG) - 40 patients. CG patients received complex therapy aimed at restoration of disturbed functions according to the standards of medical care for patients with stroke (hypotensive, antiaggregate, hypolipidemic, anticoagulant, sugar-reducing, antiarrhythmic, neurometabolic drugs were prescribed). MG patients in addition to standard therapy received the phytopreparation NeuroAid II at a dose of 800 mg 3 times a day for 3 months. The phytopreparation NeuroAid II has wide therapeutic properties, possibly influencing all pathogenetic links of stroke development and pathogenetically promoting recovery after stroke.
Keywords: Ischaemic stroke, Early recovery period, Phytotherapy, NeuroAid II
Cite this paper: Adambaev Z. I., Mirjuraev E. M., Khalikov S. V., Traditional Treatment of Stroke at the Level of Innovation, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 1104-1107. doi: 10.5923/j.ajmms.20251504.51.
Article Outline
1. Introduction
- Acute cerebral circulatory disorders (ACCD) are a major cause of disability and mortality in adults [4]. Worldwide, the incidence of acute ischemic stroke is 203 (189-218) per 100,000 people, resulting in a significant number of neurological impairments affecting daily activities [4]. According to WHO, there are 13.7 million new cases of acute ischemic stroke annually, with a total number of 80.1 million prevalent cases worldwide. Among them, 41.1 million cases were in women and 39.0 million in men, with a total number of deaths amounting to 5.5 million [3]. The regions with the highest rates were East Asia and Central and Eastern Europe [2].Recently, the lack of effective therapeutic strategies for the treatment of stroke has led to a growing interest in natural medicines (herbal medicines or phytopreparations). Recently, the general effects of some medicinal herbs in stroke have been studied. Studies have shown that medicinal herbs can improve cerebral microcirculation, protect against ischemic/reperfusion injury by reducing oxidative stress and neuroinflammation, and modulate microglia polarization [12].It is proved that the main role in stroke rehabilitation is due to such processes as neurotrophic and neuroplasticity [7,8].Some natural compounds extracted from natural medicinal formulas seem to have a high potential to protect the brain from ischemia-reperfusion injury by reducing neuroinflammation during the acute stage of stroke [11]. Interestingly, recent studies have also shown that some medicinal herbs exert neuroprotective effects in stroke by regulating microglia polarization [6]. The achievements of Chinese medicine, although well-known, have not been associated with the problem of neuroprotection until recently, largely due to the lack of experimental and clinical studies performed in accordance with current global standards of evidence-based medicine. However, recent experimental studies of a number of Chinese traditional medicine preparations, performed using the most modern molecular biological, neurochemical and pharmacological approaches, and clinical studies in compliance with the formats of international standards of clinical trials, have allowed, in particular, to substantiate the feasibility of using an innovative agent called NeuroAid or MLC 901 as a neuroprotective agent in neurological practice [10].Purpose of the study. To study the efficacy of the drug NeuroAid II in complex treatment on the dynamics of neurological deficit in patients in the early recovery period of ischemic stroke at the outpatient-polyclinic stage of treatment.
2. Material and Research Methodology
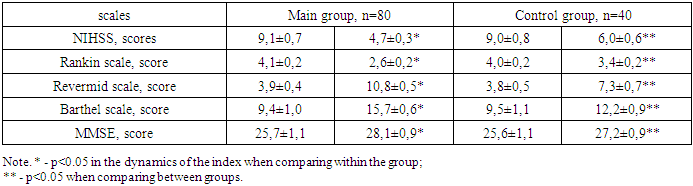
- We observed 120 patients (47 women and 73 men) in the early rehabilitation period of ischemic stroke at the outpatient-polyclinic stage of treatment. The mean age of women was 61.4±1.4 years, men - 61.6±0.9 years. Patients with IS after inpatient treatment were examined and continued treatment in outpatient clinics of Andijan city. The diagnosis was established in accordance with the requirements of the World Health Organization on the basis of clinical picture and neuroimaging data.The National Institute of Health Stroke Scale Score (NIHSS) was used to assess the severity of IS, the severity of focal neurologic deficit and to evaluate the dynamics of clinical indicators of neurologic status. Interpretation of the results: 0 points correspond to the patient's satisfactory condition; 1-4 points - mild stroke; 5-15 points - moderate stroke; 16-20 points - condition between moderate and severe stroke; 21-42 points - severe stroke.The degree of functional recovery was determined using a modified Rankin scale, which assesses the absence of manifestations (0 points) to gross impairment (5 points).Mobility index according to the Rivermead scale, which allows to rank the degree of impairment of motor functions (mobility) of the patient from 0 (inability to perform voluntary movements independently) to 15 (ability to run 10 meters in 4 seconds without limping).Barthel index of daily motor activity. At a level of motor activity of 11 points, the patient can be discharged home, provided that maximum care is provided; motor activity corresponding to 16 points implies the need for partial care of the patient; the level of motor activity of 20 points indicates the patient's independence from others.The assessment of cognitive functions was determined by the MMSE (Mini-mental State Examination) scale: normal values (≥28 points), differentiating cognitive disorders into: mild (24-27 points), dementia of mild (20-23 points) and moderate (11-19 points) degree, severe dementia (0-10 points).Patients of the control group (CG) (n=40) at the outpatient and polyclinic level received complex therapy aimed at the restoration of disturbed functions according to the standards of medical care for patients with Stroke (hypotensive, antiaggregate, hypolipidemic, anticoagulant, sugar-reducing, antiarrhythmic, neurometabolic drugs were prescribed). Patients of the main group (OG) (n=80) in addition to standard therapy received the phytopreparation NeuroAid II at a dose of 800 mg 3 times a day for 3 months.
3. Research Results
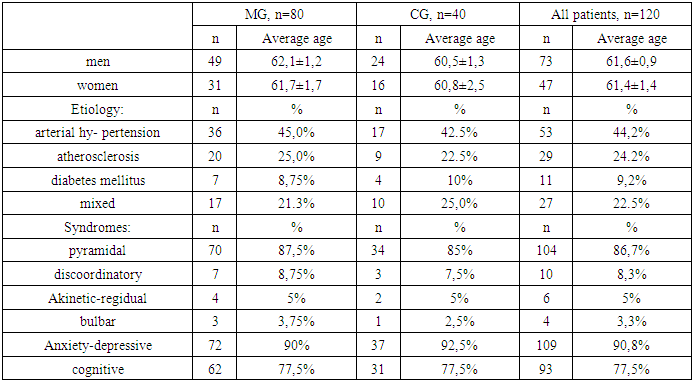
- As can be seen from Table 1, the average age of the patients in men was 61.6±0.9 years, and in women - 61.4±1.4 years. Among etiologic diseases that led to IS were arterial hypertension, atherosclerosis and diabetes mellitus, and among neurologic manifestations in our patients pyramidal, discoordinatory, akinetic-regidual and bulbar syndromes, as well as anxiety-depressive and cognitive disorders were revealed (Table 1), and the subgroup by age composition and neurologic manifestations were comparable.
|
|
4. Discussion
- As can be seen from the above, herbal collection NeuroAid II has a wide range of therapeutic effects, the main of which in the treatment of AI is due to the selected complex herbal composition, which affect the majority of risk factors for the development of ischemic strokes, namely to have the following properties: blood thinning action (like aspirin), reducing blood pressure due to antispasmodic (vasodilator) action, antilipidic (cholesterol lowering) action, antioxidant and neurometabolic (improving metabolic processes in the brain and heart) action, immunomodulatory (anti-allergic, anti-tumor) action, sugar-reducing action, sedative (antidepressant) action, a slight laxative effect, increasing the overall tone of the body.All the above-mentioned components of this remedy pharmacologically complement each other optimally, allowing to realize its unique mechanisms of action, aimed specifically at the processes of neuroplasticity and trophic support in the CNS. The most important aspect of NeuroAid action is activation of expression of a number of genes responsible for biosynthesis of leading proteins - markers of plasticity and trophic processes in the brain.The activation of neurogenesis and synaptogenesis, which, however, is subject to very rapid depletion, is directly related to the formation of neurological and cognitive deficits. Under the influence of NeuroAid, activation of neurogenesis processes in hippocampal dentate gyrus and cortex neurons is observed through stimulation of expression of one of the main markers of this process - dablcortin (DBX) protein [9], as well as activation of synaptogenesis processes through stimulation of expression of synaptotagmin - synaptic vesicle protein involved in the process of synaptogenesis and synapse function [1]. In addition, NeuroAid directly affects the molecular mechanisms of sprouting processes (as mentioned above - the most important mechanism of reparative processes in the brain during the recovery period of an IS) by stimulating the expression of GAP 43 - a protein that determines axon growth, the direction of the growth cone, and the intensity of interneuronal contacts [5].The above mentioned effects of NeuroAid, on the one hand, are extremely peculiar, not peculiar to any of the known neuroprotectants, and on the other hand - to the maximum extent ensuring the recovery of brain functions after a stroke.Thus, the selected herbal composition of NeuroAid phytopreparation has wide therapeutic properties, possibly influencing all pathogenetic links of stroke development and pathogenetically promoting recovery after stroke.
5. Conclusions
- The results of our research indicate that in patients with ischemic stroke in the early recovery period at the outpatient-polyclinic stage the addition of the phytopreparation NeuroAid II, which has a wide therapeutic effect, to the complex rehabilitation has a faster recovery of neurological deficit in this category of patients.
ACKNOWLEDGEMENTS
- The authors express their gratitude to the staff of the neurology department of the Andijan Clinical Hospital for their assistance in selecting patients for diagnosis and treatment; to Prof. Adambaev Z.I. from the Urgench branch of the Tashkent Medical Academy for writing the article; to Prof. Mirjuraev E.M. for editing the article. The authors declare that there is no conflict of interest in writing this article. The work was performed within the framework of the dissertation work. The authors used their own funds to fulfill the scientific work.