-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(4): 1094-1098
doi:10.5923/j.ajmms.20251504.49
Received: Feb. 17, 2025; Accepted: Mar. 10, 2025; Published: Apr. 16, 2025

Modern Approaches to Preparing Patients with Tuberculosis of the Hip Joint for Total Endoprosthesis Surgery
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRustamov Farrukh Halmuminovich
Department of Osteoarticular Tuberculosis of Rebuplican Specialized Scientific Practical Medical Center of Phtiziology and Pulmonology, Tashkent, Uzbekistan
Correspondence to: Rustamov Farrukh Halmuminovich, Department of Osteoarticular Tuberculosis of Rebuplican Specialized Scientific Practical Medical Center of Phtiziology and Pulmonology, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Twenty-eight patients (mean age of 41.75 ± 2.13 years) with hip joint tuberculosis (HJTB) received comprehensive examination and treatment at the department of osteoarticular tuberculosis. The results showed that in patients with HJTB, muscle contracture and deformities occur frequently and can lead to unsatisfactory treatment outcomes. However, complex diagnostic measures, conservative therapy, and a combination of spine and hip surgical procedures improve treatment results.
Keywords: Hip joint tuberculosis, Endoprosthetics, EMG
Cite this paper: Rustamov Farrukh Halmuminovich, Modern Approaches to Preparing Patients with Tuberculosis of the Hip Joint for Total Endoprosthesis Surgery, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 1094-1098. doi: 10.5923/j.ajmms.20251504.49.
Article Outline
1. Introduction
- Bone and joints tuberculosis (TB) is the most common form of extra pulmonary TB. Hip joint tuberculosis (HJTB) is the second in prevalence after TB of the spinal column, accounting for 25% of cases [2]. Etiological agent of the TB in the human body is Mycobacterium tuberculosis. Bone marrow rich bones are more susceptible to TB infection. A specific process begins with primary infection in the bone marrow regions of the bones forming the hip joint [7]. The synovial membrane of the joint has resistance to the hematogenous spread of TB infection, the secondary infection of the synovium occurs after spreading of TB infection from bone foci into the joint [4,6].The basis of the treatment of tuberculosis of the hip joint is anti-tuberculosis chemotherapy depending on the drug sensitivity of mycobacteria [3,8].But diagnosis of HJTB is complicated by underdeveloped clinical manifestations. Even when the process spreads to the joint gap, and occur clinical symptoms like swelling and sharp pains in the joint appear, increasing with the slightest movement, and radiologically bone destruction, sequestration, narrowing of the joint space, synovitis are revealed, differential diagnostics of tuberculosis of the hip joint, aseptic necrosis, osteoarthritis and arthritis of various etiologies, including autoimmune arthritis, are necessary. Even diagnostic samples taken from paraarticular abscesses do not always allow for an accurate diagnosis due to the oligobacillary phenomenon of extrapulmonary tuberculosis [10]. Late diagnosis of tuberculosis of the hip joint leads in many cases to the development of complicated forms and disability in 67% of patients [5], with leg shortening, scoliotic deformity and muscle contracture.As a result, surgical treatment of complicated forms of tuberculosis of the hip joint has become one of the most important and urgent problems of phthisiology and orthopedics.Currently, the most optimal method for restoring the function of a destroyed hip joint is its total endoprosthetics, which has become increasingly used in phthisioorthopedics [6].In HJTB, after its total endoprosthetics, the mechanical load on the resected surface of bone tissue increases [5,8], for the complete restoration of which metabolic and immune reserves of the body are required [9]. In addition, deformities and muscles contracture in HJTB lead to development of hip-spine syndrome [10], that worsens total hip endoprosthetics surgery outcomes.Thus, to prevent unsatisfactory outcomes of total endoprosthetics of the hip joint in patients with complicated forms of HJTB requires further improvement.
2. Purpose
- To improve outcomes of total endoprosthetics of the hip joint in patients with complicated forms of HJTB.
3. Materials and Methods
- The research was carried out at the Republic Specialized Scientific-Practical Medical Center of Phthisiatry and Pulmonology, involving 28(100%) patients diagnosed with HJTB between 2020 and the end of 2024. The patients' ages varied from 27 to 65 years, with a mean age of 41.75 ± 2.13 years.Before surgery, a comprehensive examination of patients is conducted, which included orthopedic examination and assessment of range of motion in affected hip joint, contractures, leg shortening and deformities.Plain radiography and CT of the lumbar spine, pelvis and hip bones performed to evaluate spine scoliosis, pelvic rotational deformities, sequestration and bone structure beyond affected hip joint. MRТ was performed to identify abscesses, synovitis and soft tissue around the hip joints.EMG mean amplitude and frequency of oscillation repetition values of MGMax and MGMed on both sides measured to evaluate muscular and neurologic function before and after surgery.Radiologically revealed excessive destructive lesions of the joint surfaces, complete resorption or destruction of the femoral head along with the neck, significant joint deformities caused by specific inflammation, that cannot be restored reconstructive surgery like necrectomy and autogenous bone grafting were indications for total hip endoprosthesis surgery. Rigid scoliotic deformities with Cobb’s angle more than 20 degrees were indication for surgical correction and fixation. For total hip endoprosthetics we used standard direct lateral approach. For spinal fusion we used piramesh cages by lateral trans-psoas approach from the concave side of the deformity. The diagnosis of HJTB was established through a combination of medical history, disease progression, histological and bacteriological evaluation of surgical samples, joint puncture samples, immunological, and radiological evaluations.
4. Results
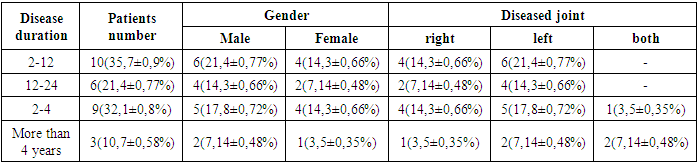
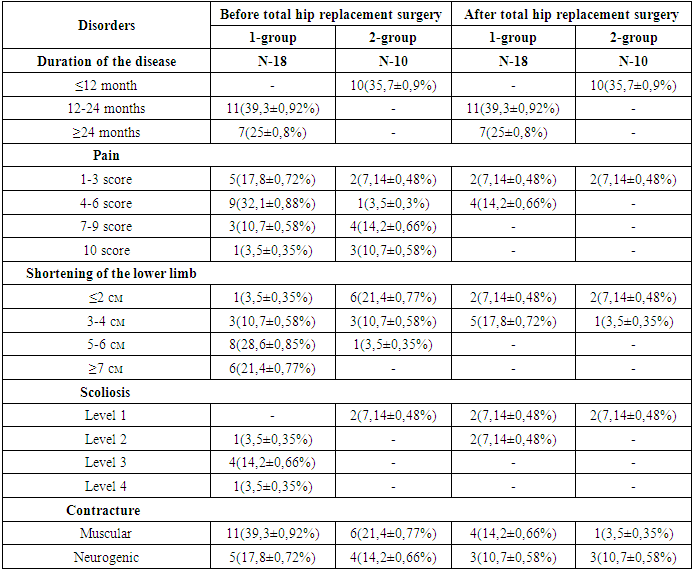
- Prior to total endoprosthesis surgery, 28(100%) (17(60,7±0,92%) male, 9(39,2±0,9%) female patients) patients underwent EMG and ENMG testing. Bilateral HJTB presented in 3(10,7±0,6%), 13(46,4±0,94%) patients were diagnosed with right HJTB and 12(42,9±0,93%) patients had left HJTB. Mild anemia presented in 12 (42.8±0,93%) patients, while 5(17,9±0,7%) had moderate anemia. Administration of intravenous iron (III) hydroxide sucrose complex at a dose of 100 mg daily for 5-10 days, along with erythropoietin 4000 IU three times a week, promoted erythropoiesis and alleviated anemia.Seven (25,0±0,8%) suffered from type II diabetes mellitus, and 2(7,14±0,48%) patients received insulin therapy, others were on sugar reducing drugs (metformin, gliclazide). Three (10,7±0,58%) diabetic patients suffered from leg pain, EMNG tests revealed peripheral neyropathy, thioctic acid 600 mg intravenously and antioxidant therapy (arginine, meldonium), and gabapentin administration reduced the pain. Based on radiological examinations, 8(28,6±0,8%) patients had metatuberculosis changes in their lungs. None of the patients diagnosed with drug-resistant TB or had a history of it. All patients were administered the first-line anti-tuberculosis therapy: isoniazid 5-10 mg/kg, rifampicin 15-25 mg/kg, ethambutol 15-25 mg/kg, and pyrazinamide 15-20 mg/kg based on body weight. No adverse effects of these drugs were observed in the patients.Based on the disease duration, these patients were divided into two groups: the first (main) group included 18(64,3±0,9%) patients (mean age 47.8), who had disease progression for over 12 months and were subsequently diagnosed with HJTB. The second (control) group included 10(35,7±0,9%) patients (mean age 43.9), whose diagnosis was made within a year (Table 1).
|
|
|
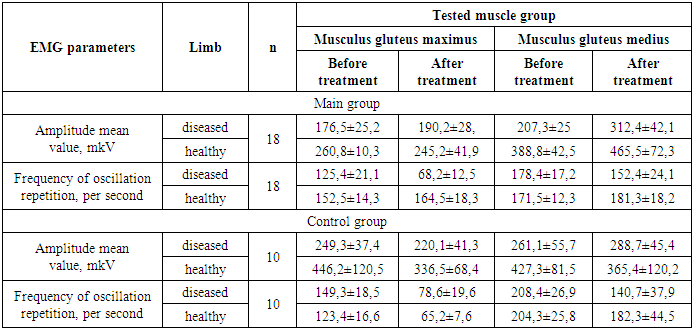
5. Discussion
- Hip spine syndrome refers to the clinicopathological association between osteoarthritis of the hip and lumbar spine pain. The term was first described by Offierski and MacNab, almost 4-decades ago, in a retrospective study that described 35 patients with combined symptomatic osteoarthritis of the hip and lower back pain [14]. Gorobets K. A. et al, 2020 analyzed medical condition of 30 patients with scoliosis after hip endoprosthetics and found that 67% of patients had lumbar pain [13]. Aftab Younus et al, 2021 in their case series highlighted the association between osteoarthritis of the hip and degenerative lumbar stenosis, and that patients with hip spine syndrome are best managed through a multi-disciplinary approach [14].Nociceptive impulses emanating from the damaged part of the hip joint slow down the activity of the muscles and their spinal cord centers. This protective system slows down the activity of the muscles directly involved in joint movements and increases the activity of other muscle systems. The bioelectric activity of the muscles of the affected hip joint before surgery is lower than the bioelectric activity of the muscles of the contralateral side. In the period after total hip replacement, the bioelectric activity of the gluteus maximus and medius muscles decreases and returns to normal over time [11,12].In our study both EMG mean amplitude and frequency of oscillation repetition values of MGMax and MGMed significantly improved postoperatively in both groups.
6. Conclusions
- The results show that in patients with HJTB, muscle contracture and deformities occur frequently and can lead to unsatisfactory treatment outcomes. However, complex diagnostic measures, conservative therapy, and a combination of spine and hip surgical procedures improve treatment results.