-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(4): 1085-1089
doi:10.5923/j.ajmms.20251504.47
Received: Jan. 17, 2025; Accepted: Feb. 13, 2025; Published: Apr. 16, 2025

Assessment of Quality of Life in Patients with High and Low Risk of Vascular Access Thrombosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLE. A. Khatamov, M. A. Sabirov, N. N. Sultonov
Republican Specialized Scientific and Practical Medical Center of Nephrology and Kidney Transplantation, Tashkent, Uzbekistan
Correspondence to: N. N. Sultonov, Republican Specialized Scientific and Practical Medical Center of Nephrology and Kidney Transplantation, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

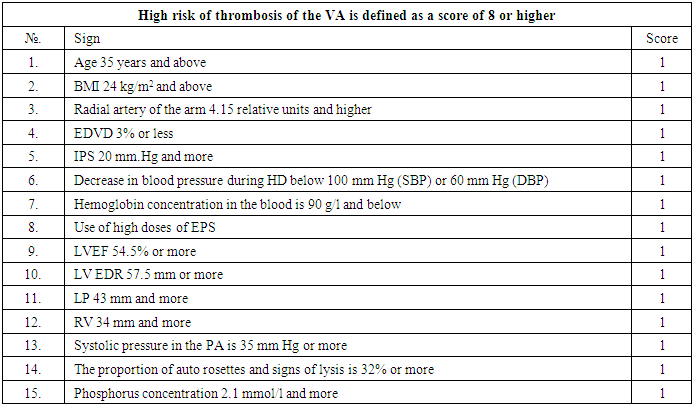
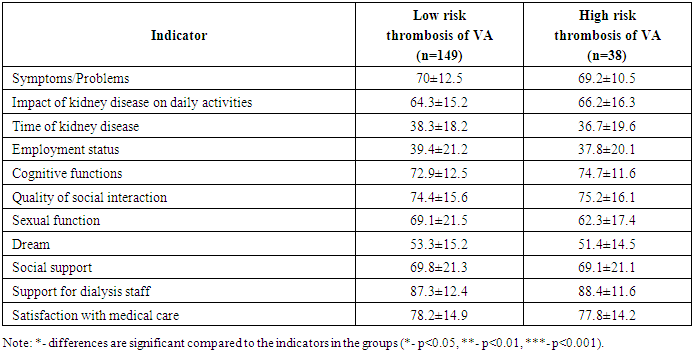
The patients were examined according to the proposed protocol using a scale developed earlier at the RSSPMTCNKT. The average score calculated according to the proposed scale for these patients was 6.11±2.44 points. Thus, a group of patients with a high risk of VA thrombosis was identified, defined as a score of 8 or more, which amounted to 38 patients - 20.32%. This category of patients was identified and marked as the first study group with a high risk of VA. The remaining patients, with a score below 8 - 149 patients (79.68%) made up the second study group and were marked as a group with a low risk of VA thrombosis. The results of the KDQOL SF V1.3 survey show that the consequences of kidney failure on the daily life of older patients are associated with the lowest quality of life scores. The following results were established when assessing the quality of life of the patients studied using scales designed for dialysis patients. The average indicators among patients of both groups were comparable with each other, some of the low indicators were: the consequences of the burden of disease associated with hemodialysis in the group with a low risk of thrombosis of VA was -38.3±18.2, and in the group with a high risk of thrombosis of VA - 36.7±19.6; the labor status in the group with a low risk of thrombosis of VA was -39.4±21.2, and in the group with a high risk of thrombosis of the VA -37.8±20.1; as well as sleep disorders in the group with a low risk of thrombosis of the VA and in the group with a high risk of thrombosis of the VA 53.3±15.2 and 51.4±14.5, respectively. At the same time, one of the indicators with a high score was in the group with a low risk of thrombosis of the VA and in the group with a high risk of thrombosis of the VA were respectively: support of dialysis staff 87.3±12.4 and 88.4±11.6 and satisfaction with medical care-78.2±14.9 and 77.8±14.2, which indicatesquality of social interaction. There were no significant differences between the two patient groups in terms of duration of hemodialysis, although patient surveys indicated a desire for more energy to participate in activities and less time on dialysis.
Keywords: Hemodialysis, Diabetes mellitus, Chronic kidney disease, Vascular access, Arteriovenous fistula
Cite this paper: E. A. Khatamov, M. A. Sabirov, N. N. Sultonov, Assessment of Quality of Life in Patients with High and Low Risk of Vascular Access Thrombosis, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 1085-1089. doi: 10.5923/j.ajmms.20251504.47.
Article Outline
1. Introduction
- In the modern world, due to progress in medical science and technology, as well as changes in lifestyle and the epidemic situation, the number of patients requiring hemodialysis for the development of chronic kidney disease (CKD) is increasing. On average, up to 0.15% of the population needs hemodialysis [5]. Hemodialysis can improve the survival and quality of life of patients with CKD [1,2,6]. Hemodialysis can be performed using a catheter, arteriovenous shunt and arteriovenous fistula. Vascular access (VA) failure in 85% of cases is associated with thrombosis. According to the literature, vascular access thrombosis develops from 0.5 to 80% per year [5,8]. Vascular access thrombosis is associated with interruption of the hemodialysis program, increased cardiovascular risk, increased hospitalization and mortality rates, the need for temporary catheter placement and associated bacteremia, as well as a significant increase in financial costs for treatment [4,9] associated with the establishment of new access, hemodialysis through temporary access, treatment of complications associated with impaired vascular access function and interruption of the hemodialysis program [3,7]. An epidemiological study of VA failure shows that the frequency of this complication worsens the quality of life of patients several times [10].Purpose of the study: assess the quality of life of patients undergoing programmed hemodialysis depending on the risk of developing vascular access thrombosis.
2. Material and Research Methods
- The study included patients receiving program hemodialysis at the Tashkent City Center for Nephrology and Kidney Transplantation. All patients underwent hemodialysis using a VA in the form of an arteriovenous fistula (AVF) formed in the surgical department of that center. The time from the operation to the start of hemodialysis (the fistula "maturation" period) ranged from 3 to 6 months. Patients were assessed depending on the risk of VA thrombosis. This division of patients into groups was carried out using the risk scale for the development of vascular access thrombosis (Table 1), developed in our center.
|
|
3. Research Results and Discussion
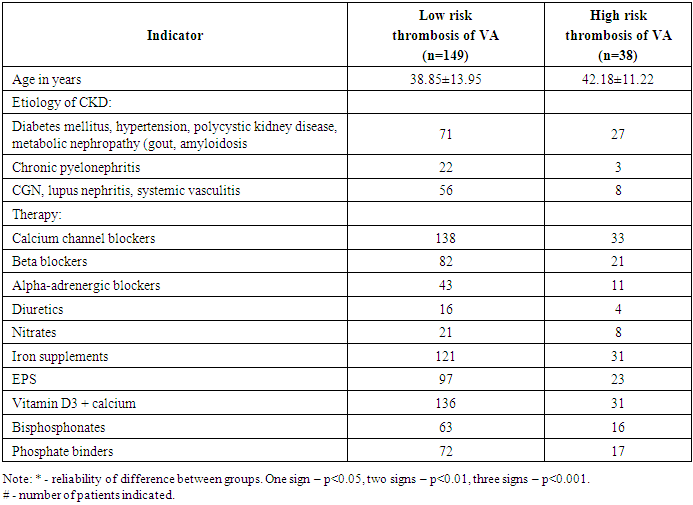
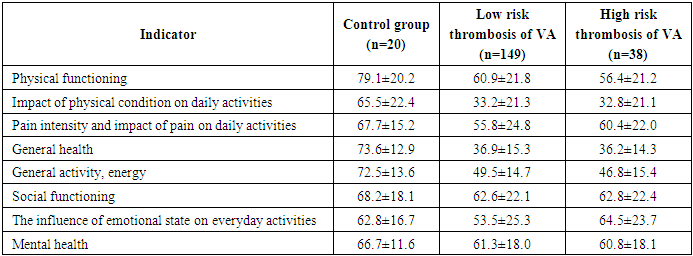
- The patients were examined according to the proposed protocol using a scale developed on the basis of a retrospective study. The average score calculated according to the proposed scale in these patients was 6.11±2.44 points. Thus, a group of patients with a high risk of VA thrombosis was identified, defined as a score of 8 or more, which amounted to 38 patients - 20.32%. This category of patients was identified and marked as the first study group with a high risk of VA. The remaining patients, with a score below 8 - 149 patients (79.68%) made up the second study group and were marked as a group with a low risk of VA thrombosis. The average age of patients was 42.64 ± 3.58 years. Also in the high-risk group there were 25 men (65.79%), and 13 women (34.21%), while in the low-risk group there were 94 men (63.09%) and 55 women (36.91%).The results of the KDQOL SF V1.3 survey show that the consequences of renal failure for the daily life of elderly patients are associated with the lowest quality of life scores. It should be noted that the scores were comparable and did not differ statistically significantly between the study groups and depending on the data in the control group. Assessment of the quality of life in the studied patients using scales intended for dialysis patients, the following results were established (Table 3). The average indicators among patients of both groups were comparable with each other, some of the low indicators were: the consequences of the burden of disease associated with hemodialysis in the group with a low risk of thrombosis of VA was -38.3±18.2, and in the group with a high risk of thrombosis of VA - 36.7±19.6; the labor status in the group with a low risk of thrombosis of VA was -39.4±21.2, and in the group with a high risk of thrombosis of the VA -37.8±20.1; as well as sleep disorders in the group with a low risk of thrombosis of the DM and in the group with a high risk of thrombosis of the VA 53.3±15.2 and 51.4±14.5, respectively. At the same time, one of the indicators with a high score was in the group with a low risk of thrombosis of the VA and in the group with a high risk of thrombosis of the VA were respectively: support of dialysis staff 87.3±12.4 and 88.4±11.6 and satisfaction with medical care-78.2±14.9 and 77.8±14.2, which indicatesquality of social interaction.
|
|
4. Conclusions
- During the study, using a scale developed earlier to identify a high-risk group for vascular access thrombosis among patients undergoing PH, it was found that patients who received 8 points or more had a high risk of vascular access thrombosis of 93.55% with a relative risk level 27.13 times higher, i.e. patients with a score of more than 8 points should be included in the high-risk group for vascular access thrombosis for preventive measures and they are characterized by a deterioration in quality of life.