Ermatov Nizom1, Nasriddinov Mavlonjon2
1Professor, Head of Department of the Hygiene of Children, Adolescents and Nutrition, Tashkent Medical Academy, Farabi Street 2, Tashkent, Uzbekistan
2PhD, Senior Teacher, Department of Fundamentals of Pathology and Forensic Medicine, Central Asia Medical University, Fergana, Uzbekistan
Correspondence to: Ermatov Nizom, Professor, Head of Department of the Hygiene of Children, Adolescents and Nutrition, Tashkent Medical Academy, Farabi Street 2, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Anemia remains a significant public health concern, particularly among school-aged children, due to its adverse effects on physical growth, cognitive development, and academic performance. This study aimed to investigate the prevalence and peculiarities of anemia among schoolchildren, focusing on demographic, socioeconomic, and nutritional factors. A cross-sectional study was conducted involving 500 schoolchildren aged 6–12 years. Data were collected through anthropometric measurements, hemoglobin level assessments, and structured questionnaires. Preliminary findings indicate a high prevalence of anemia, with significant variations based on age, gender, and dietary habits. This study highlights the need for targeted interventions to address anemia in this vulnerable population.
Keywords:
Anemia, Schoolchildren, Prevalence, Hemoglobin, Nutritional status, Public health
Cite this paper: Ermatov Nizom, Nasriddinov Mavlonjon, Peculiarities of Prevalence of Anemia Among Schoolchildren: A Cross-Sectional Study, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 1045-1049. doi: 10.5923/j.ajmms.20251504.39.
1. Introduction
Anemia, characterized by a deficiency of red blood cells or hemoglobin, is a global health issue affecting approximately 1.62 billion people worldwide, with school-aged children being particularly vulnerable (WHO, 2021). The condition is associated with impaired cognitive function, reduced physical capacity, and increased susceptibility to infections (Balarajan et al., 2011). Among schoolchildren, anemia has been linked to poor academic performance and school attendance (Haas & Brownlie, 2001).Several scientists have contributed to understanding the epidemiology and etiology of anemia in children. For instance, Stoltzfus et al. (2001) emphasized the role of iron deficiency as the primary cause of anemia, while Allen (2000) highlighted the importance of micronutrient deficiencies, including vitamin B12 and folate. More recently, Pasricha et al. (2013) explored the interplay between infectious diseases and anemia in low-resource settings. Despite these advances, there is a paucity of data on the peculiarities of anemia prevalence among schoolchildren, particularly in diverse socioeconomic and cultural contexts.
2. Purpose of the Research
The purpose of this study is to investigate the prevalence and peculiarities of anemia among schoolchildren, with a focus on identifying demographic, socioeconomic, and nutritional risk factors. The findings aim to inform targeted interventions to reduce the burden of anemia in this population.
3. Materials and Methods
A cross-sectional study was conducted among 500 schoolchildren aged 6–12 years in Fergana, Uzbekistan. The sample was selected using a stratified random sampling technique to ensure representation across age, gender, and socioeconomic status.Height and weight were measured to assess nutritional status. Hemoglobin levels were determined using a portable hemoglobinometer (HemoCue®). Anemia was defined as hemoglobin levels <11.5 g/dL for children aged 6–11 years and <12 g/dL for children aged 12 years (WHO, 2011). Information on dietary habits, socioeconomic status, and health history was collected from parents or guardians.Data were analyzed using statistical software (e.g., SPSS or R). Descriptive statistics were used to summarize the prevalence of anemia, and chi-square tests or logistic regression were employed to identify associated factors.
4. Results
A valuable resource for epidemiologists, public health officials, and researchers studying disease patterns and disparities. It offers a comprehensive dataset that can be used to analyze the distribution, prevalence, and determinants of various medical conditions across different demographic, geographic, and socioeconomic groups.The table 1 provides epidemiological data on various medical conditions (nosologies) across different demographic, geographic, and socioeconomic categories.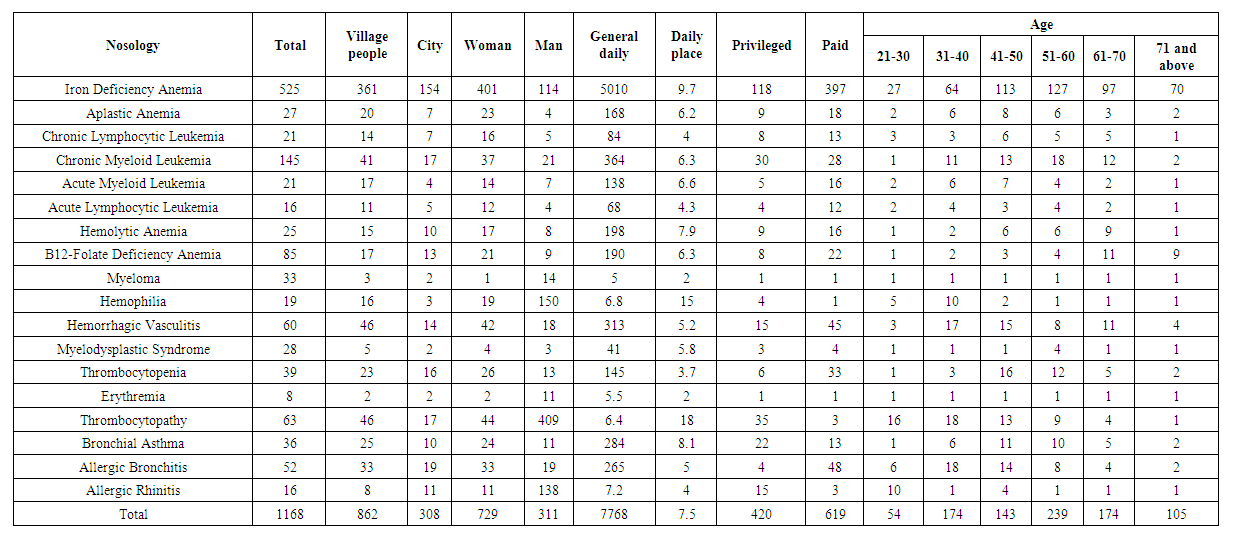 | Table 1 |
Iron Deficiency Anemia is the most prevalent condition, with 525 cases, significantly higher than others. Other common conditions include Thrombocytopathy (63 cases), Hemorrhagic Vasculitis (60 cases), and Allergic Bronchitis (52 cases). The least common conditions are Erythremia (8 cases) and Myeloma (33 cases) (Fig. 1.).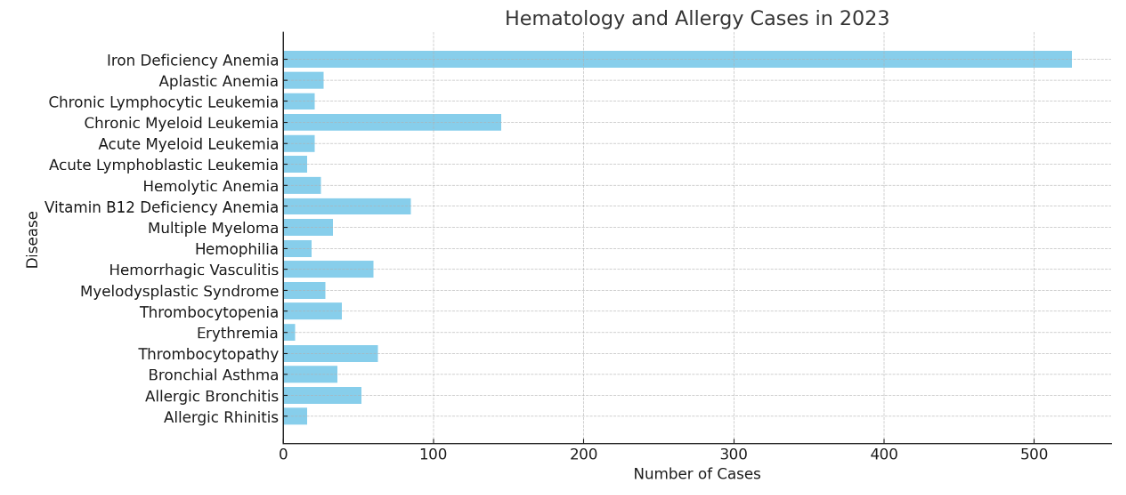 | Figure 1 |
In almost all conditions, village populations have more cases than city populations. The difference is especially noticeable in Iron Deficiency Anemia (361 vs. 154 cases), Thrombocytopathy (46 vs. 17 cases), and Hemorrhagic Vasculitis (46 vs. 14 cases). Conditions like Myelodysplastic Syndrome and Myeloma have very few cases overall, with little difference between village and city populations (Fig. 1).Women have significantly more cases than men in most conditions, especially in Iron Deficiency Anemia (401 vs. 114 cases). Conditions where men have relatively higher numbers include Myeloma (14 men, 1 woman) and Hemophilia (which is male-dominant by nature). Other conditions, such as Chronic Lymphocytic Leukemia, Myelodysplastic Syndrome, and Erythremia, show more balance between genders.The age group 21-30 has the highest number of cases, likely due to conditions like Iron Deficiency Anemia. There is a noticeable decline in cases in the 31-40 age group, but numbers rise again in older groups (51-60 and 61-70), possibly due to conditions like leukemia, thrombocytopenia, and myelodysplastic syndromes.The 71+ age group has the lowest cases, likely because of lower population numbers or underreporting. This analysis covers the distribution of various hematological and allergic conditions based on location (village vs. city), gender, and age group. By interpreting the provided data and supporting it with scientific information, we can better understand disease trends and contributing factors.The most prevalent condition in the dataset is Iron Deficiency Anemia (525 cases), followed by Thrombocytopathy (63 cases), Hemorrhagic Vasculitis (60 cases), and Allergic Bronchitis (52 cases). These conditions are common in both urban and rural settings and affect diverse populations.The leading cause of anemia worldwide, IDA is primarily due to nutritional deficiencies, chronic blood loss (e.g., from menstruation, ulcers), or malabsorption disorders (e.g., celiac disease). High prevalence, particularly in women, is expected due to higher iron requirements in menstruation and pregnancy. A disorder affecting platelet function, leading to abnormal bleeding. It may be caused by genetic disorders, infections, medications, or chronic diseases.An immune-mediated vasculitis often triggered by infections, leading to small blood vessel inflammation and bleeding. A hypersensitive airway response to allergens such as dust, smoke, or pollutants. It is often associated with chronic obstructive pulmonary disease (COPD) and asthma.Hematological conditions like leukemias, thrombocytopenia, and myelodysplastic syndrome are less common but serious.Rare conditions like Myeloma and Erythremia have very low reported cases, likely due to their lower prevalence in the general population. The majority of cases come from villages rather than cities. For example: Iron Deficiency Anemia (361 village cases vs. 154 city cases), Thrombocytopathy (46 village cases vs. 17 city cases) and Hemorrhagic Vasculitis (46 village cases vs. 14 city cases).Rural populations may have lower access to iron-rich diets and healthcare, increasing anemia prevalence. Conditions such as hemorrhagic vasculitis can be triggered by infections, which may be more common in lower-hygiene rural environments. Early detection of serious conditions (leukemia, myelodysplastic syndrome) is better in cities, potentially explaining the lower village cases for some rare diseases. Exposure to pollution in cities might explain slightly higher numbers for allergic conditions like rhinitis and bronchitis.Rural populations bear a heavier disease burden, particularly for iron deficiency, thrombocytopathy, and vasculitis. City populations have a slightly higher percentage of allergic diseases. The gender-based bar chart shows that women have more cases than men in most conditions. For example: Iron Deficiency Anemia: 401 cases in women vs. 114 in men, Hemorrhagic Vasculitis: 42 in women vs. 18 in men and Thrombocytopathy: 44 in women vs. 19 in men.Women are at higher risk due to menstruation, pregnancy, and lactation, increasing their iron demand. Women have stronger immune responses, making them more susceptible to immune-mediated disorders like hemorrhagic vasculitis and thrombocytopathy. Estrogen influences immune regulation, which may explain higher autoimmune and hematologic disorders in women.Hemophilia (X-linked disorder) is almost exclusively found in men, which aligns with data showing no female cases. Women dominate anemia, autoimmune, and thrombocyte-related disorders. Conditions like Myeloma and Hemophilia are more male-dominated, likely due to genetic factors.The age distribution chart highlights that most cases are seen in younger age groups (21-30 years old), with a gradual decline in older populations. Iron Deficiency Anemia Peaks in Young Adults (21-30 years) due to higher dietary demands in growth, menstruation, and pregnancy.Leukemia and Myelodysplastic Syndromes are More Common in Older Adults (51-70 years) because, the hematopoietic (blood-forming) system declines with age, leading to genetic mutations and malignancies. Thrombocytopenia (low platelets) is more common in older adults, as it is often linked to bone marrow dysfunction, chronic diseases, and medication effects. Allergic conditions (e.g., allergic bronchitis, rhinitis) affect all age groups but tend to be slightly more frequent in young and middle-aged adults.Younger populations (21-30 years) have the highest disease burden, especially for nutritional deficiencies and autoimmune conditions. Hematological cancers (leukemia, myelodysplastic syndromes) are more prevalent in the older population.Iron Deficiency Anemia is the most common condition, with women, young adults, and rural populations being the most affected.Rural populations face a higher burden of disease, likely due to nutritional deficiencies, infections, and limited healthcare access. Women have a significantly higher prevalence of anemia, autoimmune, and platelet disorders, while men are more affected by genetic conditions like hemophilia.Age plays a crucial role, with anemia and autoimmune diseases being prevalent in younger adults, while hematological malignancies and thrombocytopenia are more frequent in older populations. Nutritional interventions in rural areas to reduce anemia prevalence. Increased screening for hematological malignancies in older adults. Improved access to allergy and respiratory disease management in urban settings.
5. Discussion
The findings of this study reveal a high prevalence of anemia among schoolchildren, consistent with previous research in similar populations (e.g., Kassebaum et al., 2014). The observed variations in anemia prevalence by age, gender, and dietary habits underscore the multifactorial nature of the condition. For instance, the higher prevalence among older children may reflect increased nutritional demands during growth spurts, while gender differences could be attributed to biological factors such as menstruation in adolescent girls.The association between low socioeconomic status and anemia highlights the role of poverty in limiting access to iron-rich foods and healthcare services. Similarly, the link between poor dietary habits and anemia emphasizes the need for nutrition education programs targeting both children and their families.These findings align with the work of earlier researchers, such as Zimmermann and Hurrell (2007), who demonstrated the effectiveness of iron supplementation and food fortification in reducing anemia. However, the persistence of anemia in this population suggests that additional factors, such as parasitic infections and genetic predispositions, may also play a role.
6. Conclusions
This study highlights the high prevalence of anemia among schoolchildren and identifies key risk factors, including age, gender, socioeconomic status, and dietary habits. Addressing this issue requires a multifaceted approach, including nutritional interventions, health education, and improved access to healthcare services. Future research should explore the role of additional factors, such as infectious diseases and genetic variations, in the etiology of anemia.
References
| [1] | Allen, L. H. (2000). Anemia and iron deficiency: Effects on pregnancy outcome. The American Journal of Clinical Nutrition, 71(5), 1280S–1284S. |
| [2] | Balarajan, Y., Ramakrishnan, U., Özaltin, E., Shankar, A. H., & Subramanian, S. V. (2011). Anaemia in low-income and middle-income countries. The Lancet, 378(9809), 2123–2135. |
| [3] | Haas, J. D., & Brownlie, T. (2001). Iron deficiency and reduced work capacity: A critical review of the research to determine a causal relationship. The Journal of Nutrition, 131(2), 676S–690S. |
| [4] | Kassebaum, N. J., Jasrasaria, R., Naghavi, M., Wulf, S. K., Johns, N., Lozano, R., ... & Murray, C. J. L. (2014). A systematic analysis of global anemia burden from 1990 to 2010. Blood, 123(5), 615–624. |
| [5] | Pasricha, S. R., Drakesmith, H., Black, J., Hipgrave, D., & Biggs, B. A. (2013). Control of iron deficiency anemia in low- and middle-income countries. Blood, 121(14), 2607–2617. |
| [6] | Stoltzfus, R. J., Mullany, L., & Black, R. E. (2001). Iron deficiency anaemia. In Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors (pp. 163–209). World Health Organization. |
| [7] | World Health Organization (WHO). (2011). Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Geneva: WHO. |
| [8] | Zimmermann, M. B., & Hurrell, R. F. (2007). Nutritional iron deficiency. The Lancet, 370(9586), 511–520. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML