-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(4): 993-996
doi:10.5923/j.ajmms.20251504.30
Received: Mar. 2, 2025; Accepted: Mar. 26, 2025; Published: Apr. 10, 2025

Experimental Modeling of the Adhesive Process in the Abdominal Cavity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLXakimov M. Sh.1, Xayitov A. A.1, Sadikov R. A.2, 3, Mardonov J. N.2, 3, Fayzullaev B. B.1
1Tashkent Medical Academy, Tashkent, Republic of Uzbekistan
2GH “The Republican Specialized Scientific and Practical Medical Center for Surgery named after Academician V. Vakhidov”, Tashkent, Republic of Uzbekistan
3Tashkent State Dental Institute, Tashkent, Republic of Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The authors developed an experimental model of adhesive disease, which consisted in performing a median laparotomy up to 2 cm long on experimental animals. A gauze ball with a diameter of 1.5 cm moistened with a 30% acetic acid solution was applied to the parietal peritoneum of the anterior abdominal wall on the right for 2 minutes, without touching the intestinal loops. Then, for 1 minute, the same ball was in contact with the intestinal loops, after which it was removed. Experimental animals were slaughtered on days 3, 7, 10, and 14. The efficiency of the experimental model was 100%.
Keywords: Adhesive process, Abdominal cavity, Experimental model, Acetic acid, Intestinal obstruction
Cite this paper: Xakimov M. Sh., Xayitov A. A., Sadikov R. A., Mardonov J. N., Fayzullaev B. B., Experimental Modeling of the Adhesive Process in the Abdominal Cavity, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 993-996. doi: 10.5923/j.ajmms.20251504.30.
Article Outline
1. Introduction
- Adhesive disease remains one of the most complex and still unresolved problems of abdominal surgery. To date, the incidence of acute adhesive intestinal obstruction (ACN) ranges from 50 to 93.3% of all types of mechanical obstruction of non-tumor origin. With the achievements of modern surgery and intensive care, the results of the treatment of SSCN cannot be considered satisfactory. As is known, among all acute surgical diseases of the abdominal organs, intestinal obstruction is accompanied by a high mortality rate, reaching up to 15%. The main reasons for such a high mortality rate, as well as a large number (18.7 – 41.8%) of postoperative complications, are the late treatment of patients, the predominance of elderly and senile people, and a significant percentage of diagnostic and tactical errors at all stages of treatment of acute renal failure [1,10,11,18].Treatment of adhesive disease remains an urgent problem of abdominal surgery [1,6,8,14]. The complexity of its solution is related both to the physiological need to limit the inflammatory process in the abdominal cavity, and to the effectiveness of the mechanisms of resorption of adhesions after the elimination of inflammation [3,7,13]. Thus, the methods of prevention and treatment of adhesive disease should be strictly differentiated. In many respects, the study of the processes of development and resorption of adhesions can be implemented in experimental studies, but in laboratory animals these processes proceed much faster and more efficiently than in humans [4]. Currently, a search and comparative evaluation of the effectiveness of various models of adhesive disease in experimental animals is being conducted [5,7].Considering the above, the aim of the study was to develop an experimental model of adhesive disease in rats to study the processes of development and prevention of the adhesive process.
2. Research Material
- Experimental studies were performed in the Department of Experimental Surgery of the State Institution "Vakhidov Russian National Research Medical Center". Studies were conducted on outbred white rats (2-4 individuals) of both sexes, weighing 240±20 g. The animals were kept in separate cages of 2 individuals. The food was balanced in terms of calories and vitamins, and water was provided in unlimited quantities. Surgical operations and manipulations were performed under anesthesia in accordance with the international requirements established by the European Convention for the Protection of Vertebrates (Strasbourg, 18.03.1986, with confirmation in Strasbourg on 15.06.2006).3 series (8 experimental animals in each series) of experiments were conducted using 20%, 30% and 35% acetic acid solution. As a result of the research conducted нby nmi, an experimental model of adhesive disease is proposed. After achieving anaesthetic sleepизофлюрана, a median laparotomy of up to 2 cm in length was performed with isoflurane vapor under mask anesthesia. A gauze ball with a diameter of 1.5 cm moistened with a 30% acetic acid solution was applied to the parietal peritoneum of the anterior abdominal wall on the right for 2 minutes, without touching the intestinal loops. Then, for 1 minute, the same ball was in contact with the intestinal loops, after which it was removed. The abdominal wall was sutured with a double-row continuous 3/0 nylon suture. Postoperative pain relief was provided by adding 500 mg of ibuprofen per 100 ml of drinking water.Photodocumentation of the animals' condition and macro-changes in the abdominal cavity was carried out with a digital camera with a sensitivity of at least 20 MP.The density and elasticity of the formed adhesions were investigated by studying the degree of fusion (at break) using a special device on which the strength of the gap or separation of the adhesions from the attached or linked organs could be determined by the strength of the adhesions.To determine the strength of implant adhesion, a standard technique was used. To do this, a device was used, which is an equal-shoulder rocker arm, for one of the shoulders of which the studied spike sample was attached, and a load cup was attached to the other. By placing standard weights on the cup, we determined the force at which the junction will detachfrom the test surface. The results of the study were recorded and processed. The adhesive strength was calculated in Pa (1 pascal [Pa] = 0.01019716 grams-force per square centimeter [gs/ cm2]).Histological studies of biopsies of tissues and organs of the abdominal cavity were performed by fixation in 10% neutral забуференном поLily-buffered formalin for at least 24 hours. After dehydration in alcohols of ascending concentration according to the generally accepted method, the material was poured into paraffin, sections with a thickness of 5-7 microns were stained with hematoxylin-eosin. Light-optical micrographs were obtained using a “DN-300M " microscope coupled with a digital camera and computer. All microphotographs were processed and stored on a computer using Microsoft "Windows 10 pro" application programs.Statistical analysis of numerical data was performed using the Statistica-7 software (StatSoft, Inc., USA) using standard descriptive statistics methods.
3. The Results Obtained
- Experimental studies have shown that the most optimal model is one using 30% acetic acid.In most experimental modelsнаибольшая выра, the highest expressionенность of the adhesive process is observed 3-7days after the initiation of the adhesive process. In the next1-0-1-4days, the adhesive process undergoes resorption due to well-expressed repair processes in rats. As a result, only a part of the adhesions that occurred on day 7 remain, which persist for a longer period of time. Таким Thus, studies on the possibility of preventing the development of adhesions should be conducted up to 7 days after the initiation of adhesions, and when developing methods to accelerate the resorption of already formed adhesions, it is advisable to conduct studies after 7 days of the experiment.On day 7 after damage to the parietal and visceral peritoneum with a swab containing 30% acetic acid, the adhesiveprocess in the righthalf of the abdominalcavity occurred in 12 (100%) rats that underwent repeated laparotomies under general anesthesia. The most pronounced adhesions occurred with the parietal peritoneum, whereи подпаяны the omentum, small and large intestines were soldered. The adhesions were mostly planar in nature with an adhesion strength of 81.0,0±0.6 Pa (Fig. 1).
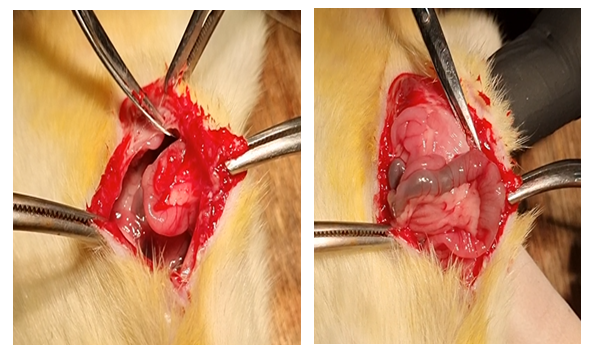 | Figure 1. Planar adhesions of the intestine with the parietal peritoneum of the anterior abdominal wall |
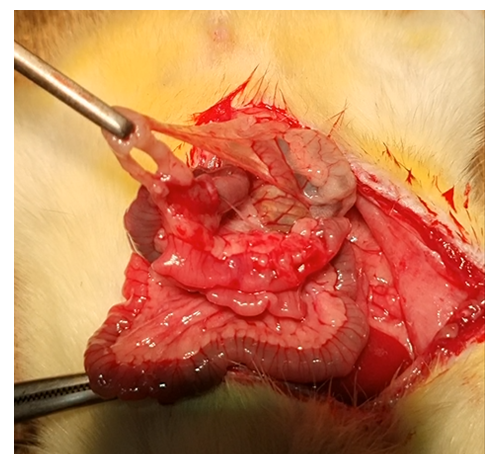 | Figure 2. Inter-intestinal adhesions in the form of strands |
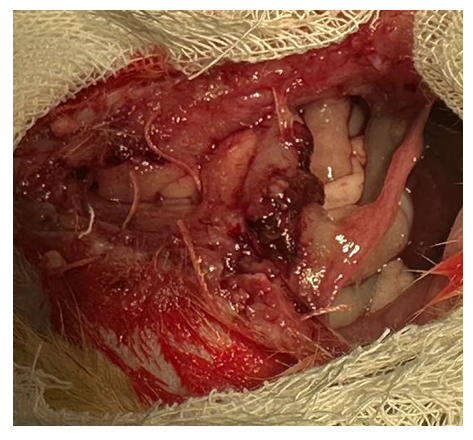 | Figure 3. 10 days. Conglomerate of intestinal adhesions, omentum with parietal peritoneum |
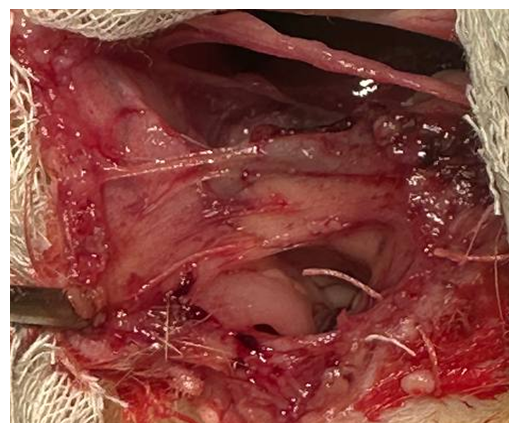 | Figure 4. 14 days. Dense formed adhesions of the parietal peritoneum with the anterior abdominal wall |
4. Discussion of the Results
- To study the development of the pathological process, evaluate the effectiveness of the methods used for diagnosis and treatment of various diseases, various experimental models are traditionally used [1,9,12,15]. The development of a model of the adhesive process in the abdominal cavity is currently an urgent problem. Many methods of modeling adhesion formation have been proposed, but so far none of them is universal in application, since surgery at the present stage of development is not only high-tech, but also invasive, which increases the polyvalence of factors damaging the peritoneum.Given this fact, the aim of the study was to create an optimal model of adhesive disease.The existing modelscan be grouped as follows, depending on the factors that lead to spiking.1. Mechanical: trauma to the peritoneum during dissection, gripping it with tools, wiping it with gauze napkins, excising areas of the peritoneum during surgical intervention [2,10];2. Physical: drying of the peritoneum with air, exposure to high temperature (burns) when using an electric knife, laser radiation, plasma scalpel, hot solutions during surgery [11,17];3. Infectious: penetration of infection into the abdominal cavity by endogenous (inflammation of the abdominal organ with the development of local and general inflammation of the peritoneum) and exogenous (with injury, perforation, opening of the hollow organ) ways [6,9];4. Implantation: aseptic inflammation of the peritoneum as a result of leaving tampons, drainage tubes, non-absorbable or long-term absorbable suture material, talcum powder from gloves, hemorrhages in the peritoneum during suturing [4,5,19];5. Chemical: action of substances that cause chemical burns and aseptic inflammation of the peritoneum (iodine, alcohol, concentrated solutions of antibiotics, furacilin, etc.) [16,18,20].The conducted studies allowed us to establish that changes in the adhesive process in the abdominal cavity in rats can be caused with a fairly high probability and duration. On the 7th day after initiation fromrations by burning the parietal (2 minutes) and visceral peritoneum (1 minute) with a tampon with 30% vinegar, planar adhesions develop, while we did not note any cases of death or absence of formed adhesions. At the same time, the use of acetic acid in a higher concentration (35%) caused purulent-necrotic complications and perforation of hollow organs. Lower concentrations of vinegar did not always lead to the development of adhesions in the abdominal cavity. The severity of adhesions was greatest by 7 days after peritoneal injury, and the strength of adhesionof adhesions was greatest to the anterior abdominal wall and amounted to 81.0±0.60 Pa. On day 14 after surgery, the area of formed adhesions decreased, while the strength of the adhesions increased-120±0.4 Pa. The phenomena of intestinal obstruction in the form of the formation of double-barrelled small intestine and the expansion of its lumen occurred in 20% of patientson the 7th day after surgery, and by the 14th day there were no signs of intestinal obstruction.Thus, we have developed an experimental modelaimedая at creating an adhesive disease, that is as closeas possible to clinical practice.
5. Conclusions
- Experimental model of adhesive disease has been developed, which consists in applying a 1.5 cm diameter gauze ball moistened with a 30% solution of acetic acidtothe parietal peritoneum of the anterior abdominal wall on the right for 2 minutes without touching the intestinal loops, and then for 1 minute the same ball is in contact with the parietal peritoneum of the anterior abdominal wall. with bowel loops, it has 100% experimental efficacy.