-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(4): 947-951
doi:10.5923/j.ajmms.20251504.21
Received: Mar. 2, 2025; Accepted: Mar. 28, 2025; Published: Apr. 6, 2025

Clinical and Neurological Features of Patients with Chronic Lymphocytic Leukemia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEshchanova Guzal Bakpolatovna1, Babadjanov Jasurbek Kamiljanovich1, Matmurdov Rustambek Jumanazarovich2, Jumanazarova Shakhzoda Rustambekovna2
1Urgench Branch of Tashkent Medical Academy, Urgench, Uzbekistan
2Tashkent Medical Academy, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

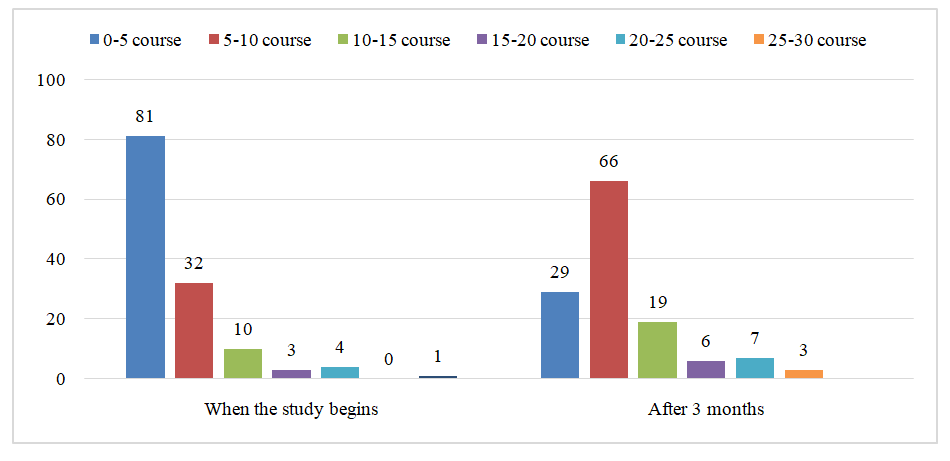
The prevalence of chronic lymphocytic leukemia in the Republic of Uzbekistan is 5.24 per 100,000 population. According to various literature data, damage to the nervous system in chronic lymphocytic leukemia, unlike other lymphoproliferative diseases, is diagnosed very rarely. Objective. To study the clinical and neurological characteristics of patients with chronic lymphocytic leukemia. Material and methods.130 patients with chronic lymphocytic leukemia were examined at the Khorezm branch of the Republican Scientific Research Center of Hematology and Transfusiology of the Ministry of Health of the Republic of Uzbekistan (Khorezm branch of the Republican Scientific Research Center of Hematology and Transfusiology of the Ministry of Health of the Republic of Uzbekistan). The scientific research was based on the results of patients with CLL who were treated as inpatients from 2014 to 2023. Of these, 71 were men (54.6%) and 59 were women (45.4%). The ratio of men to women was 1.2:1.Results. All patients in the study underwent various courses of polychemotherapy. Patients underwent 3 courses of polychemotherapy during the follow-up period. Before the start of the study, patients had received an average of 4 courses of polychemotherapy (maximum 24 times and minimum 1 time). In our study, 29 patients underwent their first course of PCT. After 3 months, the average number of PCT courses patients had undergone was 7 (maximum 27 times and minimum 4 times) (Fig. 1). Patients with chronic lymphocytic leukemia mainly complained of general weakness, tremor and unsteadiness, hearing loss, dizziness, memory loss, and headache. Only 17 of 130 patients (13.08%) did not complain during the anamnesis collection. In 36 (26.67%) patients, no changes were found in the neurological examination. Vestibulo-atactic syndrome was the majority of neurological disorders in 57 (43.85%) patients. Sensory disturbances were observed in 7.69% of patients, including polyneuropathy in 5.38% and hemihypeesthesia in 2.31%.Conclusion: The development of neurological syndromes is influenced not only by comorbidities, but also by the CLL disease itself and the complications of polychemotherapy. Neurological symptoms in patients do not appear as a result of true neurological pathology, but rather during treatment and as a result of CLL intoxication.
Keywords: Chronic lympholeicosis, Neurological complications, Damage to the nervous system
Cite this paper: Eshchanova Guzal Bakpolatovna, Babadjanov Jasurbek Kamiljanovich, Matmurdov Rustambek Jumanazarovich, Jumanazarova Shakhzoda Rustambekovna, Clinical and Neurological Features of Patients with Chronic Lymphocytic Leukemia, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 947-951. doi: 10.5923/j.ajmms.20251504.21.
1. Introduction
- Lymphoproliferative diseases are malignant and benign neoplasms that develop from lymphoid cells at various stages of differentiation [1]. One of the most common diseases in this group is chronic lymphocytic leukemia (CLL). The prevalence of chronic lymphocytic leukemia in the Republic of Uzbekistan is 5.24 per 100,000 population [2,4]. According to various literature data, nervous system damage in chronic lymphocytic leukemia, unlike other lymphoproliferative diseases, is diagnosed very rarely and is noted in approximately 1% of cases [3,7]. However, there are reasons to believe that nervous system damage is more common. First, nervous system damage is underestimated, since their manifestation in chronic lymphocytic leukemia is not specific, and it is difficult for specialists (neuropathologists and hematologists) to distinguish nervous system damage in CLL from other neurological diseases. Secondly, in most cases, damage to the nervous system in CLL is asymptomatic and is detected only at autopsy [5,6]. The diagnosis of neurological complications of CLL, especially in the early stages, is not given sufficient attention and is often diagnosed after the development of severe neurological focal complications, which leads to disability of patients. Neurological complications of CLL associated with polychemotherapy are the most studied in the world and local literature, and they usually affect the peripheral nervous system. Damage to the nervous system in CLL often occurs "hidden", which in turn can escape the attention of neurologists and other specialists. In patients with chronic lymphocytic leukemia, in addition to neurological disorders, the appearance of neuropsychological disorders (anxiety and depression) increases, leading to a decrease in quality of life and a decrease in social adaptation [2,5]. The dynamic development of modern oncohematology has led to an increase in the survival rate of patients with chronic lymphocytic leukemia. All this determines the relevance and purpose of the study of issues related to the diagnosis and treatment of nervous system diseases in patients with chronic lymphocytic leukemia.In modern oncohematology, polychemotherapy is the main and most successful method of treatment. Due to the increase in the average life expectancy of patients with CLL, when choosing a treatment strategy, it is necessary to take into account not only its effectiveness, but also delayed side effects.Purpose. Study of clinical and neurological characteristics of patients with chronic lymphocytic leukemia.
2. Material and Methods
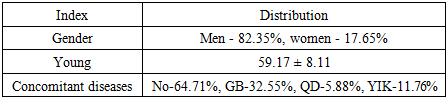
- 130 patients with chronic lymphocytic leukemia were examined at the Khorezm branch of the Republican Scientific Research Center of Hematology and Transfusiology of the Ministry of Health of the Republic of Uzbekistan (Khorezm branch of the Republican Scientific Research Center of Hematology and Transfusiology of the Ministry of Health of the Republic of Uzbekistan). The scientific research was based on the results of patients with CLL who were treated as inpatients from 2014 to 2023. Of these, 71 were men (54.6%) and 59 were women (45.4%). The ratio of men to women was 1.2:1.were aged 46 to 86 years, including 13 patients (15.5%) aged 13 to 44 years, 25 patients (29.8%) aged 45 to 59 years, 37 patients (44.0%) aged 60 to 74 years, and 9 patients (10.7%) older than 75 years. The mean age of the patients was 64.07±9.56 years (p<0.05).When the patients were studied according to the time of onset of the disease, the following situation was found: up to 6 months - 32 patients (24.62%), from 6 months to 1 year - 17 patients (13.08%), from 1 to 3 years - 31 patients (23.84%), from 3 to 5 years - 30 patients (23.08%), over 5 years - 20 patients (15.38%). 25.38% (33) of the patients have higher education, and the remaining 74.62% (97) have secondary and vocational secondary education.
3. Results
- All 130 patients underwent clinical examinations by evaluating their anamnesis, complaints and neurological status.All patients in the study underwent various courses of polychemotherapy. Patients underwent 3 courses of polychemotherapy during the follow-up period. Before the start of the study, patients had received an average of 4 courses of polychemotherapy (maximum 24 times and minimum 1 time) [2]. In our study, 29 patients underwent their first course of PCT. After 3 months, the average number of PCT courses patients had undergone was 7 [5] (maximum 27 times and minimum 4 times) (Figure 1).
 | Figure 1. Distribution of patients receiving polychemotherapy treatment courses at baseline and 3 months later |
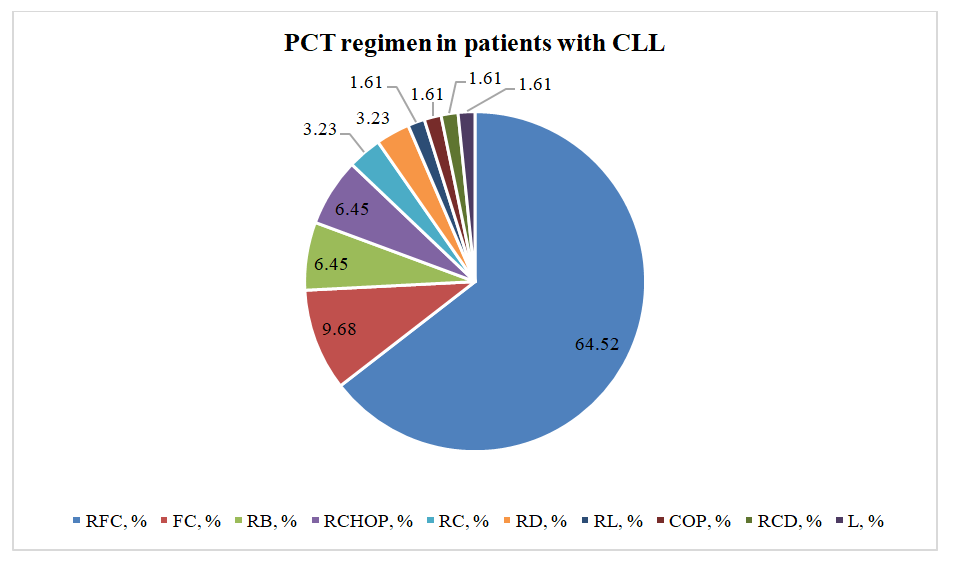 | Figure 2. Distribution of polychemotherapy regimens in patients with chronic lymphocytic leukemia |
|
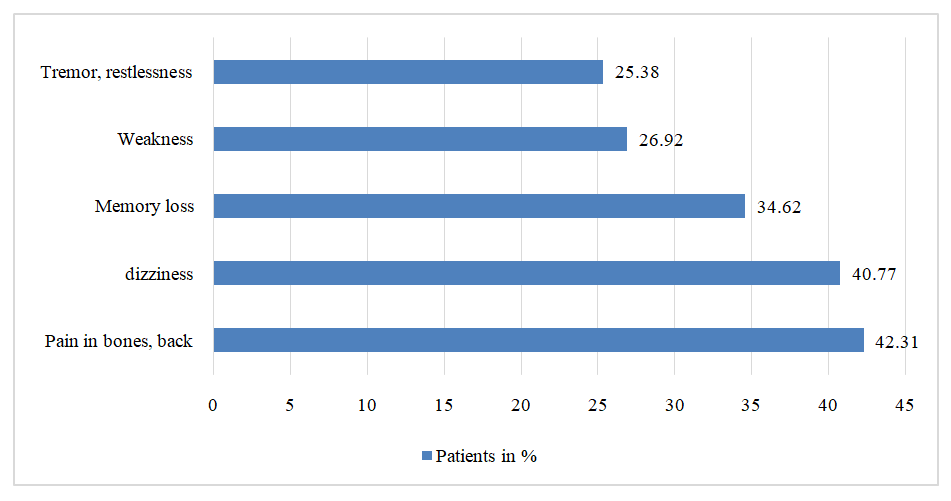 | Figure 3. Patient's main complaints (n =130) |
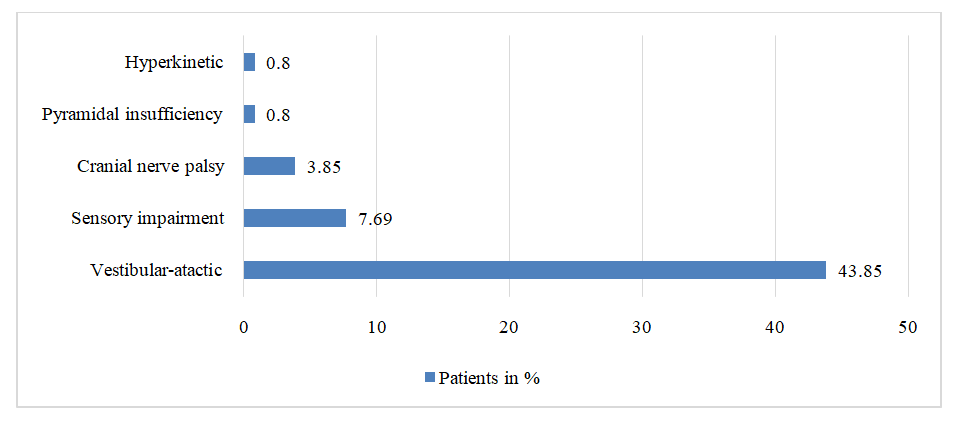 | Figure 4. Prevalence of neurological syndrome in patients (n=130) |
4. Conclusions
- The development of neurological syndromes is influenced not only by concomitant diseases, but also by the CLL disease itself and the complications of polychemotherapy. Complaints such as dizziness, general weakness, headache, hearing loss, tremor, memory loss and headache in patients do not arise as a result of a true neurological pathology, but rather arise during treatment and as a result of CLL intoxication.The development of sensory disturbances in our patients occurred after the acute cerebral circulation disorder (before the onset of lymphoproliferative disease), as well as polyneuropathy as a complication of polychemotherapy.