-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(3): 825-827
doi:10.5923/j.ajmms.20251503.70
Received: Feb. 11, 2025; Accepted: Mar. 20, 2025; Published: Mar. 28, 2025

Assessment of the Functional State of the Kidneys in Children Against the Background of Community-Acquired Pneumonia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLLola Daminova Turgunpulatovna1, Dilnoza Muminova Alisher Qizi2, Nigora Aliyeva Rustamovna3
1Tashkent State Dental Institute, Tashkent, Uzbekistan
2Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
3Department of Hospital Pediatrics No. 1, Folk Medicine, Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
Correspondence to: Dilnoza Muminova Alisher Qizi, Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Acute respiratory infections, including pneumonia, often lead to kidney damage, which often determines the course and prognosis of the primary disease. [3,7] Patients with community-acquired pneumonia, the diagnosis of AKI may be difficult due to the lack of information on premorbid serum creatinine levels. [10] A short episode of AKI in terms of long-term prognosis is associated with an increased risk of developing CKD. [8] In our research, we investigated the prevalence and prognostic factors of AKI in children with community-acquired pneumonia.
Keywords: Community-acquired pneumonia, Acute kidney injury (AKI), Chronic kidney disease (CKD), Serum creatinine (Cr) and cystatin C (CysC)
Cite this paper: Lola Daminova Turgunpulatovna, Dilnoza Muminova Alisher Qizi, Nigora Aliyeva Rustamovna, Assessment of the Functional State of the Kidneys in Children Against the Background of Community-Acquired Pneumonia, American Journal of Medicine and Medical Sciences, Vol. 15 No. 3, 2025, pp. 825-827. doi: 10.5923/j.ajmms.20251503.70.
1. Introduction
- Pneumonia is the leading single infectious cause of death among children worldwide. According to WHO, 740,180 children under five years of age died from pneumonia in 2019, accounting for 14% of all deaths in children under five years of age, and among children aged one to five years, pneumonia accounted for 22% of all deaths. [1] In recent years, morbidity and mortality due to pneumonia have been increasing, while acute kidney injury (AKI) remains one of the causes of high mortality in pneumonia. The kidneys are sensitive to hypoxia, ischemia, infectious-toxic influences, nephrotoxic effects of drugs and disorders of systemic hemodynamics. Therefore, during severe community-acquired pneumonia (CAP), there is a high probability of developing renal dysfunction. [7]
2. Aims
- The main purpose of our study was to assess the functional state of the kidneys in children with community-acquired pneumonia.
3. Method
- Our research was conducted at the 1st City Children’s Clinical Hospital of Tashkent in the period 2024-2025. The study included children aged 5 to 7 years with community-acquired pneumonia, the main group (MG) of 120 patients, and the control group (CG) of 20 healthy children. The diagnosis of community-acquired pneumonia was made based on clinical symptoms and chest radiography. All study participants had their serum creatinine (Cr) and cystatin C (CysC) levels measured. Acute kidney injury (AKI) was defined as an increase in serum creatinine concentration of 26.5 μmol/L (0.3 mg/dL) within 3 days; or increase in serum creatinine to ≥1.5 times baseline within the prior seven days; or urine volume ≤0.5 mL/kg/hour for six hours (Kidney Disease Improving Global Outcomes (KDIGO) classification, 2012.) [2]
4. Results
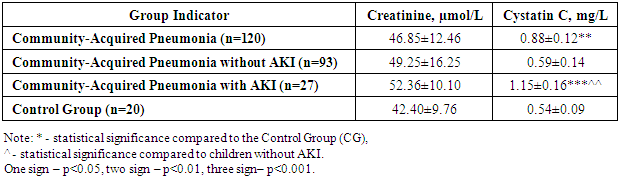
- The results of the study (Table 1) showed that the initial blood creatinine concentration in children with community-acquired pneumonia was comparable to that of healthy children (46.85±12.46 µmol/L vs. 42.40±9.76 µmol/L, the difference was not significant). At the same time, a different pattern was observed in the analysis of serum cystatin C concentration: overall, the average cystatin C level in the serum of children with pneumonia was significantly higher than that of the control group (0.88±0.12 mg/L vs. 0.52±0.09 mg/L, p<0,001) Quantitative analysis showed that the cystatin C concentration in the blood of 39 (32.5%) children with pneumonia exceeded the control values, with an average of 0.95±0.24 mg/L. Among them, 5 children had cystatin C levels exceeding the reference values (1.2 mg/L), with an average of 1.25±0.11 mg/L. Thus, already from the first day, nearly a third (32.5%) of children with community-acquired pneumonia showed signs of kidney dysfunction, according to the serum cystatin C concentration level.
|

|
5. Conclusions
- Thus, the conducted study showed that in children with community-acquired pneumonia, 32.5% (39 children) of cases exhibited impaired kidney function from the first days of the illness, manifested by an increase in serum cystatin C levels. Acute kidney injury was registered in 27 (22.5%) children. In children with pneumonia complicated by AKI, the average cystatin C concentration in the blood was significantly higher than in those without AKI (p<0.001).