-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(3): 822-824
doi:10.5923/j.ajmms.20251503.69
Received: Feb. 20, 2025; Accepted: Mar. 21, 2025; Published: Mar. 28, 2025

Complex Treatment of Maxillary Sinus Cysts
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhayitov A. A., Nasretdinova M. T.
Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Khayitov A. A., Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction Chronic cystic maxillary sinusitis (HCMS), which occupies one of the leading places from the list of chronic nasal pathology. There is still no consensus on the modern approach to the diagnosis and treatment of cysts. In modern otorhinolaryngology, the problem of choosing an adequate treatment for chronic cystic maxillary sinusitis remains urgent. The purpose of our study is to develop proposals and recommendations aimed at improving the surgical treatment of maxillary sinus cysts. Materials and methods The research work was based on the examination of 153 patients with chronic cystic maxillary sinusitis, who were divided into 2 groups depending on the presence of pathological changes in the ostiomeatal complex. All patients underwent an otorhinolaryngological examination, which consisted of an endoscopic examination of the nasal cavity and nasopharynx, pharyngoscopy, otoscopy and laryngoscopy, MSCT of the paranasal sinuses. Surgical treatment to remove the maxillary sinus cyst was performed in one and two stages, as well as using three approaches, depending on the location of the cyst in the sinus. Results The use of differentiated endoscopic surgery significantly improved the quality of the treatment of maxillary sinus cysts, reduced the severity and number of complications after surgery. Conclusions with different locations of cysts in the maxillary sinus, it is necessary, in our opinion, to choose a tactic that will provide better visualization of the cyst in the sinus and less trauma.
Keywords: Chronic cystic maxillary sinusitis, Ostiomeatal complex, Quality of life, Endoscopy, Paranasal sinuses
Cite this paper: Khayitov A. A., Nasretdinova M. T., Complex Treatment of Maxillary Sinus Cysts, American Journal of Medicine and Medical Sciences, Vol. 15 No. 3, 2025, pp. 822-824. doi: 10.5923/j.ajmms.20251503.69.
Article Outline
1. Relevance
- In otorhinolaryngologic practice, chronic cystic maxillary sinusitis (CCMS) is often encountered, which occupies the leading position among chronic sinusitis. The incidence of this disease has been increasing over the last 20 years. Inflammation of paranasal sinuses (PNS) is the most frequent disease in the structure of ENT pathology. According to studies, CRS significantly affect the quality of life of patients [1,4,8,14]. The origin of nasal paranasal sinus cysts is usually associated with chronic inflammatory process in the perinasal sinuses of the nose, and according to some authors, the etiology of PNS cysts is more related to allergy, so they are considered as a manifestation of allergic sinusitis [3,6,10,12,13]. To date, there is no standardized opinion on the symptomatology of the course of cystic sinusitis, and interest in this pathology is not decreasing. A unified standard of modern diagnostics and treatment of cystic sinusitis has not been created. Modern rhinosurgery in otorhinolaryngology is looking for new, adequate principles of solving the problem of choosing an appropriate treatment for chronic cystic maxillary sinusitis [2,5,7,9,11]. At present, finding ways to improve the quality of surgical treatment of cysts of the maxillary sinus is of great importance.The aim of our study was to substantiate the choice of differentiated approach in surgical treatment of maxillary sinus cysts.
2. Materials and Methods of the Study
- The basis of our study consisted of 153 patients with chronic cystic maxillary sinusitis (CCMS), who were on outpatient and inpatient observation in the clinic of OOO “Golden medical group”, in the period from 2018-2023. All patients underwent surgical intervention to remove cysts from the maxillary sinus. When collecting anamnesis, one of the main complaints in all patients was headache (98%), 70% of patients complained of nasal discharge of mucous character. General weakness was detected in 61% of patients. 34.5% of patients reported a feeling of pressure in the area of the affected sinus. Most of the patients were found to have mucous flowing down the posterior wall of the nasopharynx and oropharynx. The study began with an otorhinolaryngologic examination, which consisted of endoscopic rhinoscopy, pharyngoscopy, otoscopy and laryngoscopy, and tomographic examination of the perinasal sinuses.All patients underwent computed tomography, which was performed on Siemens Somatom Sensation Cardiac (Germany). The study was performed in axial, coronal and sagittal projections. Computed tomography data were an important navigational material for the most accurate, gentle and safe surgical interventions. In the majority of cases (n=131 86%), unilateral involvement of the maxillary sinuses was detected.The study was conducted in different groups, divided by the localization of cysts in the MS, as well as by the presence of pathological changes in the ostiomeatal complex (OMC). Among such changes we found such changes as nasal septum curvature in the form of a ridge at the level of the middle shell, bullous hypertrophy or curved middle shell, hypertrophy of the lattice bladder, anomalies of the hook-shaped process, the presence of Galer cells and an additional accessory sinus of the maxillary sinus. Based on these data, we divided all patients into 2 large groups. Group A included patients with pathologic changes in the OMC (n=87), and group B without pathologic changes in the OMC structures (n=66). Each group was divided into subgroups 1, 2 and 3 depending on the location of cysts in the maxillary sinus. Thus, groups A1 (n=51) and B1 (n=37) included patients with cysts located on the inferior wall of the MS. Group A2 (n=29) and B2 (n=19) included patients with cysts located on the posterior wall of the MS. Group A3 (n=7) and B3 (n=10) included patients with cysts located on the anterior and superior walls of the MS (Fig. 1).
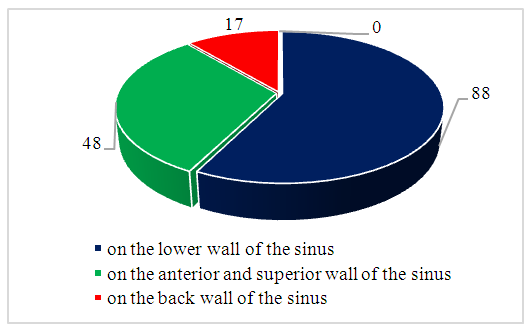 | Figure 1. Localization of the cyst in the maxillary sinus |
3. Results of Clinical Studies
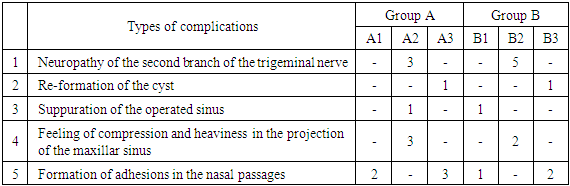
- All patients underwent surgical treatment for cyst removal. The surgical intervention was performed under general anesthesia with additional local anesthesia, and in some cases by patients' consent only under local infiltration anesthesia. In patients of group A (n=87) the surgical intervention consisted of 2 stages, the first stage consisted of correction of intranasal structures and pathologic changes of the ostiomeatal sinus (partial resection of the middle shell, hook-shaped process, joining of the additional joint with the main one, opening of the Haller cells). At the second stage, the maxillary sinus was opened depending on the cyst localization. Patients from group B (n=66) underwent only the second stage of surgical intervention.When cysts were localized on the inferior wall of the MS, patients in groups A1 and B1 underwent sinus opening using our improved technique through the inferior nasal passage. Our technique consisted in the fact that after breaking and luxation, medialization of the lower nasal shell, a “L” shaped incision of soft tissues of the lateral wall of the lower nasal passage with the length of 1.5 -2 centimeters was made. Soft tissues were cut off with the help of a raspator, after exposing the bony wall, a boron was used to create a joint sufficient for simultaneous insertion of the endoscope tip and shaver nozzle. After visualization of the cysts with the endoscope, they were removed with forceps. The sinus was washed with warm physiologic solution. Upon completion of manipulations in the sinus, a syntomycin swab was placed in the lower nasal passage and removed after 1-2 days.When cysts were localized on the posterior wall of the MS, patients in groups A2 and B2 underwent sinus opening through the anterior wall of the MS. Patients in groups A3 and B3 underwent opening of the MS through the middle nasal passage.Endoscopic optics of 2.7 and 4 mm, with angles of vision from 00 to 700; video equipment with HD monitor and necessary instruments were used during surgical interventions.In early and late postoperative periods, endoscopic examinations and, if necessary, dressings were performed, and the dynamics of changes in the postoperative inflammatory process was recorded in different periods of the postoperative period (up to 2 years).On 7-10 days after surgical interventions, the maxillary sinus was rinsed with warm physiologic solution, with the addition of antibiotic, antiseptic and proteolytic enzyme. Endoscopic and retgenologic examination of the maxillary sinus was performed on day 30, after 3, 6 and 12 months. If necessary, fibrin films and traction, crusts and scabs after coagulation were removed. All patients were treated with antibiotic therapy depending on the results of bacteriologic culture with determination of sensitivity to one or another antibiotic. As a local desensitizing therapy a local glucocorticoid drug of combined action Rialtris was prescribed for a duration of a year to 2 years. The composition of Rialtris includes mometasone furoate and olopatadine, these active substances are representatives of 2 different classes of drugs (synthetic glucocorticosteroid and H1-histamine receptor antagonist).As a result of our study, we found the following complications in our patients: trigeminal neuropathy, cyst recurrence, suppuration of the maxillary sinus, a feeling of heaviness in the area of the anterior sinus wall, adhesions in the middle and lower nasal passages.
|
4. Conclusions
- The choice of tactics of surgical treatment of maxillary sinus cysts should always be left to the operating surgeon. Comparison of the results of our study on the choice of the course of surgical intervention suggests that at different locations of cysts in the maxillary sinus it is necessary, in our opinion, to choose the tactics with which there will be better visualization of the cyst in the sinus and less traumatization of the surrounding tissues.