Mukhitdinova Kamola Oybekovna1, Aleynik Vladimir Alekseevich2, Najmutdinova Dilbar Kamariddinovna3
1Andijan State Medical Institute, Andijan, Uzbekistan
2Institute of Human Immunology and Genomics of the Academy of Sciences of the Republic of Uzbekistan
3Tashkent Medical Academy, Uzbekistan
Correspondence to: Mukhitdinova Kamola Oybekovna, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The results of the study highlighted the significance of alarmins, which are endogenous molecules released during cellular stress or tissue injury. In the context of early pregnancy, these alarmins may serve as critical signaling molecules that activate the immune system, potentially leading to a heightened pro-inflammatory response. This response, while usually protective, can paradoxically contribute to the complications seen in miscarriages, as the presence of inflammation can disrupt the delicate balance necessary for embryo implantation and development. It was concluded that in women without genital infections, appropriate inflammation is necessary for a successful pregnancy outcome, which can be accompanied by an increase in pro-inflammatory and a decrease in anti-inflammatory interleukins. Also, an increase in alarmins involved in sterile inflammation. The heightened proinflammatory immune response, along with a marked rise in alarmins that play a role in intensifying sterile inflammation during the initial phases of pregnancy, can lead to adverse conditions for early gestation and increase the risk of miscarriages.
Keywords:
Sterile inflammation, Excessive proinflammatory immune response, Interleukins, Alarmins, Early pregnancy, Miscarriage
Cite this paper: Mukhitdinova Kamola Oybekovna, Aleynik Vladimir Alekseevich, Najmutdinova Dilbar Kamariddinovna, The Role of Sterile Inflammation in Early Pregnancy Among Women Experiencing Miscarriage and an Elevated Pro-Inflammatory Immune Response, American Journal of Medicine and Medical Sciences, Vol. 15 No. 3, 2025, pp. 817-821. doi: 10.5923/j.ajmms.20251503.68.
1. Introduction
Inflammation is a defensive reaction of the host against foreign enemies. Inflammation that is not usually associated with a pathogenic infection is called sterile inflammation. In the field of reproductive immunity, pathological inflammation is the cause and pathology of various obstetric and gynecological complications. Simultaneously, within the realm of reproduction, inflammatory responses are deemed essential for processes such as implantation, placentation, defense against foreign pathogens, and childbirth [8]. Nevertheless, an overabundance of inflammation can lead to several complications during pregnancy, including infertility [3], recurrent pregnancy loss [4], premature delivery [2], and preeclampsia [9].In recent years, sterile inflammation has been closely associated with various diseases. It is triggered and induced by endogenous molecules such as highly mobile box group 1 (HMGB1), IL-1a, IL-33, heat shock proteins and S100 proteins, uric acid, which are all released from cells into the extracellular region upon cell damage. These molecules, which are collectively associated with damage, are called inflammatory "alarms" [7].In the context of cellular stress or injury, HMGB1 is released into the extracellular space, where it functions as a potent pro-inflammatory cytokine. This release is often a response to various stimuli, including oxidative stress, ischemia, or necrosis, leading to the activation of distinct immune pathways. HMGB1 interacts with several cell surface receptors, such as the receptor for advanced glycation end-products (RAGE) and Toll-like receptors (TLRs), triggering a cascade of inflammatory responses. This mechanism underlines HMGB1’s dual role within the cell—acting as a critical nuclear component and functioning as an alarm signal in the extracellular environment. In vitro and in vivo, HMGB1 administration causes inflammation [12].In recent years, uric acid has also been widely considered as a signaling agent of sterile inflammation due to the high cytosolic concentration released during cell death [10].The complexity of the interleukin-1 family extends beyond IL-1α and IL-1β. Other members, such as IL-1Ra, provide a regulatory mechanism, acting as an antagonist that competes with IL-1α and IL-1β for the IL-1R1 receptor. This balance between pro-inflammatory and anti-inflammatory signals is critical in preventing excessive inflammation, which could lead to tissue damage and chronic inflammatory diseases. The dynamic interplay among these cytokines is vital for maintaining homeostasis within the immune system. In addition, the signaling pathways activated by IL-1 cytokines involve several key transcription factors, including NF-κB and AP-1. These transcription factors orchestrate the expression of various genes responsible for inflammation, thus influencing the systemic response to infection or injury. Moreover, the effects of IL-1 signaling are not limited to acute inflammation; they also play a role in chronic conditions such as autoimmune diseases and metabolic disorders. Recent studies have highlighted the importance of IL-1 family cytokines in various disease contexts, paving the way for potential therapeutic interventions. Targeting IL-1 signaling pathways with monoclonal antibodies or receptor antagonists has shown promise in clinical trials, demonstrating the therapeutic potential of modulating this critical branch of the immune response [6].Interleukin (IL)-33 is a new member of the IL-1 cytokine superfamily. IL-33 can function as a traditional cytokine and as a nuclear factor regulating gene transcription. Thus, the effects of IL-33 are either pro- or anti-inflammatory, depending on the disease and the model [5].
2. Main Body
2.1. Purpose of the Study
The study aimed to explore the influence of sterile inflammation during the early phases of pregnancy in women who have experienced miscarriages, particularly looking at the intensity of an enhanced pro-inflammatory immune response while ruling out any occurrences of genital infections.
2.2. Material and Methods of Research
This investigation involved 44 females, categorized into two distinct groups. Group 1 comprised 26 women who successfully carried their pregnancies to term and delivered without any prior genital infections before they conceived. Conversely, Group 2 consisted of 18 women who had undergone miscarriages within the first 12 weeks of pregnancy; like those in Group 1, these participants also had no histories of genital infections prior to conception. Blood samples were taken from the participants before conception and again at the 6-week and 12-week points during their pregnancies. The analysis utilized ELISA to measure specific parameters: the pro-inflammatory markers IL-1b (interleukin-1 beta) and TNF-α (tumor necrosis factor-alpha), along with the anti-inflammatory marker IL-10 (interleukin-10). The test kits used for this analysis were sourced from JSC Vector-Best, located in Russia. In addition, indicators of alarms involved in sterile inflammation were studied in the blood. The ELISA method was used to study the level of highly mobile boxing group 1 (HMGB1), interleukin-1a (IL-1a) using Cusabio Biotech test systems in the USA, interleukin-33 (IL-33) with the Cloud Clone Corp test system in the USA, as well as HUMAN uric acid levels in Germany.Enzyme-linked immunosorbent assay (ELISA) is a laboratory immunological method for detecting antigens and antibodies, based on the determination of the "antigen-antibody" complex by introducing an enzymatic label into one of the reaction components, followed by its detection using an appropriate substrate that changes its color. The basis for conducting ELISA is the determination of the products of enzymatic reactions during the study of test samples in comparison with negative and positive controls.Data analysis was performed using variation statistics. Within the framework of this study, mean values and standard errors were calculated, and the coefficient of significance of differences was determined using the Student-Fisher method (t).
2.3. The Results Obtained and Their Discussion
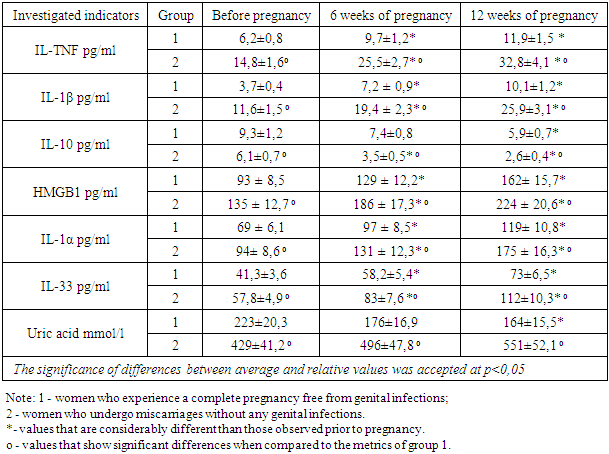
The research results revealed that among women in group 1, the TNF-α concentration in the bloodstream at the sixth week of pregnancy was significantly heightened, measuring at 9.7 ± 1.2 pg/ml, as compared to levels observed before conception. By the twelfth week of gestation, this value increased to 11.9 ± 1.5 pg/ml, which did not represent a substantial rise from the sixth week. Nevertheless, this level was markedly higher than the baseline recorded prior to pregnancy, which stood at 6.2 ± 0.8 pg/ml, as illustrated in the accompanying table. (Table 1).Table 1. Variations in TNF-α, IL-1β, IL-10, HMGB1, IL-1α, IL-33, and uric acid levels in the bloodstream of women across the studied groups
 |
| |
|
In the women from group 2, the TNF-α levels measured at 3.7 ± 0.4 pg/ml prior to pregnancy were significantly 2.3 times elevated compared to those in group 1. By the 6th week of gestation, women in group 2 exhibited a TNF-α level of 25.5 ± 2.7 pg/ml, which was also significantly and notably higher, exceeding 2.6 times that of group 1, as well as being markedly elevated from their pre-pregnancy levels of 14.8 ± 1.6 pg/ml. At the 12th week, TNF-α levels in group 2 reached 32.8 ± 4.1 pg/ml, representing a significant increase of 2.8 times when compared to group 1 and showing a notable rise of 2.2 times relative to their earlier pre-pregnancy values. (Table 1).During the IL-1b study, changes in the findings were noted that closely resembled those of TNF-α. This was particularly evident in group 2 women, who displayed significantly increased metrics both before conception and at 6 and 12 weeks into their pregnancies when compared to the figures from group 1. Moreover, these results were considerably higher than the pre-pregnancy data for group 2, as illustrated in the table. The results indicate a likely interaction between IL-1β and TNF-α in regulating immune responses in early pregnancy. The increased concentrations of these cytokines in group 2 point to a pronounced inflammatory setting, which may impact both the health of the mother and the development of the fetus. Previous studies have shown that an optimum balance of pro-inflammatory cytokines is crucial for successful implantation and placentation. Therefore, the observed elevations may reflect adaptive immune mechanisms aiming to protect the fetus during the early stages of gestation. Additionally, the significance of tracking these inflammatory markers cannot be overstated. As group 2 women demonstrated higher metrics consistently throughout the initial weeks of pregnancy, it opens up avenues for further exploration into whether such elevations could serve as biomarkers for complications like preeclampsia or gestational diabetes. By establishing a clearer understanding of these cytokine profiles, clinicians might be better equipped to identify at-risk individuals and intervene promptly. Further research is warranted to delineate the precise roles of IL-1β and TNF-α in the context of pregnancy. Understanding their shared pathways and divergent influences could lead to targeted therapeutic strategies aimed at fostering healthier pregnancies and better maternal-fetal outcomes. Ultimately, this knowledge may prove invaluable in guiding clinical practices and improving monitoring protocols for expectant mothers. (Table 1).By the sixth week of gestation, the concentration of IL-10 in the blood of women in group 1 (7.4 ± 0.8 pg/ml) was significantly reduced in comparison to levels observed prior to pregnancy (9.3 ± 1.2 pg/ml). For these same women, at 12 weeks of pregnancy, the IL-10 (5.9 ± 0.7 pg/ml) level - did not show a statistically significant decrease from the 6-week mark, yet it remained significantly lower than the pre-pregnancy levels. Conversely, in women of group 2 before becoming pregnant, IL-10 (6.1 ± 0.7 pg/ml) levels were found to be significantly 1.6 times lower than those in group 1. Furthermore, these levels were notably 1.8 times lower than the 6-week results (3.5 ± 0.5 pg/ml) and 2.2 times lower than the 12-week (2.6 ± 0.4 pg/ml) results - when compared to the pre-pregnancy values of the same group. At both the 6-week and 12-week stages of pregnancy, women in group 2 exhibited significantly lower IL-10 levels compared to those in group 1, with reductions of 2.1 and 2.3 times, respectively (Table 1).The investigation into the alarmin HMGB1 levels in the blood of women from group 1 indicates that at the sixth week of pregnancy, concentrations of HMGB1 (129 ± 12.2 pg/ml) were considerably elevated compared to pre-pregnancy levels (93 ± 8.5 pg/ml). Additionally, for those in the same group at the twelfth week, HMGB1 (162 ± 15.7 pg/ml) levels - did not exhibit a statistically significant rise compared to the sixth week, yet they remained considerably elevated compared to pre-pregnancy measurements. The significant increase in HMGB1 at the sixth week may reflect the physiological changes required to support the developing embryo and protect it from potential immunological threats. This elevation in HMGB1 could also be linked to the remodeling of the maternal immune system, which is essential for successful implantation and fetal development. (Table 1).In group 2, the baseline HMGB1 levels prior to pregnancy (135 ± 12.7 pg/ml) were significantly elevated compared to group 1. By the 6th week of pregnancy, women in group 2 exhibited HMGB1 levels (186 ± 17.3 pg/ml) that were 1.4 times greater than those in group 1 and also higher than their pre-pregnancy values. Furthermore, during the 12th week, group 2 exhibited an HMGB1 measurement of 224 ± 20.6 pg/ml, which was notably 1.4 times elevated compared to group 1 and 1.7 times above their levels prior to pregnancy. (Table 1).The study on the alarmin IL-1a demonstrated that in women categorized as group 1, the levels of IL-1a at the 6th week of pregnancy (97 ± 8.5 pg/ml) were significantly higher than their pre-pregnancy levels (69 ± 6.1 pg/ml). However, by the time they reached the 12th week of pregnancy, the IL-1a levels in the same group (119 ± 10.8 pg/ml) did not display a notable increase from those at week 6, although they remained considerably elevated in comparison to the baseline values recorded before pregnancy (Table 1). Similarly, in group 2, a comparable pattern was noted; their IL-1a levels before pregnancy (94 ± 8.6 pg/ml) were significantly 1.4 times greater than those in first group. At the six-week mark of pregnancy, group 2 demonstrated an IL-1a level of 131 ± 12.3 pg/ml, which was 1.4 times higher than that recorded in group 1 and significantly exceeded their values from before pregnancy. By the twelfth week, the IL-1a concentration for women in group 2 reached 175 ± 16.3 pg/ml, indicating a considerable 1.5-fold increase compared to group 1 and a 1.9-fold rise relative to their pre-pregnancy measurements (Table 1).The research regarding the alarmin IL-33 demonstrated that for women in first group, the levels measured were 58.2 ± 5.4 pg/ml at the 6-week of gestation. This indicated a notable increase when compared to their levels before pregnancy, which were 41.3 ± 3.6 pg/ml. Interestingly, by the twelfth week, the IL-33 level for the same group (73 ± 6.5 pg/ml) did not exhibit a significant increase from what was recorded at the sixth week, but still showed a considerable rise from the pre-pregnancy figures (see Table 1). Conversely, women in group 2 demonstrated a similar trend, with pre-pregnancy IL-33 values (57.8 ± 4.9 pg/ml) notably 1.4 times higher than those in group 1. At the sixth week of pregnancy, women in group 2 exhibited IL-33 levels (83 ± 7.6 pg/ml) that were significantly 1.4 times higher than group 1 and 1.5 times greater than their pre-pregnancy results. At the twelfth week, the level of IL-33 in group 2 (112 ± 10.3 pg/ml) was significantly higher, being 1.5 times that of group 1 and double their initial measurements (refer to Table 1). The rise in IL-33 concentrations indicates a varied reaction to pregnancy among the two groups of women, underscoring the possible role of this alarmin in the physiological adjustments that occur during gestation. The higher baseline levels in group 2 indicate a pre-existing advantage in immune modulation, which may influence their pregnancy trajectory. This disparity raises intriguing questions about the mechanisms driving these variations and their implications for maternal and fetal health. Moreover, the stability of IL-33 levels in group 1 from the sixth to the twelfth week suggests a plateau effect, potentially indicating a distinct regulatory mechanism at play once a certain threshold is reached. In contrast, the continual rise observed in group 2 could suggest an enhanced immune response or a different hormonal environment that favors elevated IL-33 production. The findings also underline the importance of tracking these alarmin levels throughout pregnancy as potential biomarkers for assessing maternal health and predicting outcomes. Future studies should explore the functional consequences of elevated IL-33, particularly its role in placentation, inflammation, and overall maternal-fetal interactions. (Table 1).When analyzing uric acid concentrations, especially in relation to alarms, it was observed that women in group 1 displayed levels of 176 ± 16.9 mmol/L by the sixth week of pregnancy. This figure was not significantly lower than their pre-pregnancy average of 223 ± 20.3 mmol/L. By week twelve, the uric acid levels in group 1 reached 164 ± 15.5 mmol/L, indicating no major decrease since week six, although these levels were still considerably above their pre-pregnancy values (Table 1). In contrast, women in group 2 presented with an average uric acid level of 429 ± 41.2 mmol/L prior to pregnancy, which was 1.9 times higher than that of group 1. At the 6th week of pregnancy, the uric acid level for group 2 reached 496 ± 47.8 mmol/L, reflecting a significant increase of 2.8 times compared to group 1. By the 12th week, their levels were at 551 ± 52.1 mmol/L, indicating a substantial difference, specifically 3.4 times higher than those in group 1, and not a significant increase from their pre-pregnancy levels (Table 1).The data collected suggests that a favorable pregnancy outcome relies on the presence of appropriate inflammation, characterized by elevated levels of pro-inflammatory interleukins coupled with reduced levels of anti-inflammatory interleukins. Additionally, there is an increase in alarmins that contribute to sterile inflammation. A significant increase in pro-inflammatory immune responses and a significant increase in danger signals leading to severe infertile inflammation in early pregnancy — without sexual infections - can lead to early pregnancy conditions and increase the risk of miscarriage. This, suggests that while inflammation appears essential for successful pregnancy, an excessive or misregulated inflammatory response could be detrimental, potentially harming the progression of early gestation and leading to adverse outcomes. Thus, maintaining the right balance of inflammatory mediators is crucial for healthy pregnancy advancement.
3. Conclusions
In women who do not have genital infections, a proper inflammatory response is essential for a favorable pregnancy outcome, often marked by a rise in pro-inflammatory interleukins and a reduction in anti-inflammatory ones. Additionally, there is an elevation of alarmins associated with sterile inflammation. The initial phases of pregnancy feature a fragile equilibrium within the immune system, shifting from a preparedness to respond to potential threats to a state that fosters fetal growth and development. However, the notable rise in pro-inflammatory immune reactions can disrupt this balance. These heightened reactions often manifest as increased levels of cytokines and other inflammatory markers, signaling a response that, while necessary in some contexts, can paradoxically threaten the viability of the embryo. Instead of fostering a supportive environment, acute inflammatory responses may lead to a hostile intrauterine ecosystem. Moreover, sterile inflammation, characterized by the absence of pathogens, suggests that the immune system reacts excessively to physiological changes. This phenomenon can elevate the risk of complications in early pregnancy, as the detection of warning signals, including tissue damage cues, drives the immune system into an overactive state. Such an environment can result in heightened uterine contractility and alterations in maternal blood flow, further compromising the essential conditions for embryo implantation and growth. Given these risks, understanding the underlying mechanisms of pro-inflammatory responses is crucial. Identifying potential triggers—ranging from environmental factors to stressors—may provide insight into preventing adverse outcomes such as miscarriages. Effective management of the maternal immune response during this critical period is essential for promoting successful pregnancies and safeguarding maternal and fetal health. The integration of immunological research into prenatal care could pave the way for novel therapeutic strategies aimed at mitigating these inflammatory reactions.
References
| [1] | Celona, B., Weiner, A., Di Felice, F., Mancuso, F. M., Cesarini, E., Rossi, R. L., ... & Agresti, A. Substantial histone reduction modulates genomewide nucleosomal occupancy and global transcriptional output // PLoS biology. – 2011. – Т. 9. – №. 6. – С. e1001086. |
| [2] | Christiaens, I., Zaragoza, D. B., Guilbert, L., Robertson, S. A., Mitchell, B. F., & Olson, D. M. Inflammatory processes in preterm and term parturition // Journal of reproductive immunology. – 2008. – Т. 79. – №. 1. – С. 50-57. |
| [3] | Gupta, S., Goldberg, J. M., Aziz, N., Goldberg, E., Krajcir, N., & Agarwal, A. Pathogenic mechanisms in endometriosis-associated infertility // Fertility and sterility. – 2008. – Т. 90. – №. 2. – С. 247-257. |
| [4] | Laird, S. M., Tuckerman, E. M., Cork, B. A., Linjawi, S., Blakemore, A. I. F., & Li, T. C. A review of immune cells and molecules in women with recurrent miscarriage // Human reproduction update. – 2003. – Т. 9. – №. 2. – С. 163-174. |
| [5] | Miller A. M. Role of IL-33 in inflammation and disease // Journal of inflammation. – 2011. – Т. 8. – С. 1-12. |
| [6] | Nadeau-Vallée, M., Obari, D., Palacios, J., Brien, M. È., Duval, C., Chemtob, S., & Girard, S. Sterile inflammation and pregnancy complications: a review // Reproduction. – 2016. – Т.152. – №.6. – С. R277-R292. |
| [7] | Negishi, Y., Shima, Y., Kato, M., Ichikawa, T., Ino, H., Horii, Y., ... & Morita, R. Inflammation in preterm birth: Novel mechanism of preterm birth associated with innate and acquired immunity // Journal of Reproductive Immunology. – 2022. – Т. 154. – С. 103748. |
| [8] | Negishi, Y., Shima, Y., Takeshita, T., & Morita, R. Harmful and beneficial effects of inflammatory response on reproduction: sterile and pathogen-associated inflammation // Immunological medicine. – 2021. – Т.44. – №.2. – С. 98-115. |
| [9] | Redman C. W. G., Sacks G. P., Sargent I. L. Preeclampsia: an excessive maternal inflammatory response to pregnancy // American journal of obstetrics and gynecology. – 1999. – Т.180. – №. 2. – С. 499-506. |
| [10] | Shi Y., Evans J. E., Rock K. L. Molecular identification of a danger signal that alerts the immune system to dying cells // Nature. – 2003. – Т.425. – №. 6957. – С. 516-521. |
| [11] | Štros M. HMGB proteins: interactions with DNA and chromatin // Biochimica et Biophysica Acta (BBA) - Gene Regulatory Mechanisms. – 2010. – Т. 1799. – №.1-2. – С. 101-113. |
| [12] | Yang, H., Wang, H., Czura, C. J., & Tracey, K. J. The cytokine activity of HMGB1 // Journal of leukocyte biology. – 2005. – Т.78. – №. 1. – С. 1-8. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML