-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(3): 739-743
doi:10.5923/j.ajmms.20251503.53
Received: Feb. 27, 2025; Accepted: Mar. 11, 2025; Published: Mar. 15, 2025

Specific Features of the Facet Joint in Women of Different Ages
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDilmurod Abdurasulovich Gaipov1, Sayyora Mukhamadovna Akhmedova2
1Independent Researcher, Tashkent Medical Academy, Tashkent, Uzbekistan
2Doctor of Medical Sciences, Professor, Tashkent Medical Academy, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The methodological article is devoted to the current problem of morphometric changes in the facet joints in the female body. The study was conducted on 224 women aged 16 to 75 years, and based on their computed tomography data, the articular growths of the upper and lower lumbar vertebrae were studied. According to the results of the study, with the increase in the age of women, a change in the height of the facet joints of the lumbar vertebrae was observed. Age–related morphometric changes were especially noticeable during adolescence and early puberty. Also, changes in the facet joints may be associated with osteochondrosis and other diseases, which is of great importance in improving women’s health and preventive work.
Keywords: Facet joint, Women, Different ages, Morphometric changes, Female body, Articular growths, Lumbar vertebrae, Adolescence, Osteochondrosis, Diseases, Medicine, Morphology, Anatomy, Traumatology, Orthopedics
Cite this paper: Dilmurod Abdurasulovich Gaipov, Sayyora Mukhamadovna Akhmedova, Specific Features of the Facet Joint in Women of Different Ages, American Journal of Medicine and Medical Sciences, Vol. 15 No. 3, 2025, pp. 739-743. doi: 10.5923/j.ajmms.20251503.53.
Article Outline
1. Introduction
- Today, in modern society, there is growing interest in the health problems of older women. The world’s female population is not only growing, but also their age index is increasing. Today, about 15% of them are women of menopausal age. Every year, 25 million people are added to their number, and by 2020 this figure will increase to 47 million [2,3]. Possessing traditions, experiences, spiritual values, and possessing great creative and intellectual potential, older women make a great contribution to the life of the family and society. Therefore, maintaining women’s health during menopause, preventing and correcting the consequences of systemic vascular and metabolic diseases associated with estrogen deficiency and the onset of menopause are of urgent and economic importance for public health. They can also contribute to or complicate the adaptation of a woman in transition. In the perimenopause period, most women already have one or more somatic diseases, which can significantly affect the quality of life of women, which makes menopause more difficult and complicated [1,5]. At the same time, the incidence of dystrophic diseases of the spine has been increasing recently, in the development of which the age–related deterioration of the facet joints and the yellow ligament plays an important role, but in–depth research and studies have not yet been conducted in this area [7,9,10]. Analysis of the literature, works devoted to the facet joint have not been comprehensively studied by age, gender, bilaterally [6,8]. It follows that morphological study of age–related changes in the facet joint and the yellow ligament in women during the fertile and menopausal periods will serve as a basis for identifying pathological conditions observed in them, developing new selective preventive and therapeutic measures [4]. Facet joints are small mobile joints between the vertebrae, which are responsible for maintaining the stability of the body and controlling its movements. These joints are a pressing issue for doctors and researchers because their degeneration and injuries can lead to various conditions, including osteochondrosis, spondylosis, and various traumas. Therefore, the study of facet joints, their mechanisms of functioning, and disease prevention is one of the most relevant areas in medicine. Taking the above into account, we set ourselves the goal of studying the specific morphometric changes in the facet joints of women of different ages at different ages.
2. Materials and Methods
- To achieve our goal, we studied the height and width of the upper and lower lumbar vertebrae in a total of 224 women aged 16 to 75 years based on computed tomography data. The selection of women was strictly controlled. In the selected women, radiculopathy, myelopathy, signs of trauma to the spinal column and other diseases were excluded during X–ray examinations. We divided the women taken for observation into 2 groups. The first group was the control group, which consisted of 109 women, women in this group led a normal lifestyle and did not regularly take calcium and vitamin D products. The second group was the main group, which consisted of 115 women of different age groups. We selected women in this group who regularly took the Calcium D 3 Nycomed preparation (500/200 IU) and followed a healthy lifestyle.The average height of women in adolescence (16–20 years) was 158.3±0.5 mm, and their body weight was 56.6±0.5 kg. The average height of women in the first puberty period (20–35 years) was 163±0.3 mm, and their weight was 59±0.5 kg. The average height of women in the second puberty period (35–55 years) did not change significantly compared to the previous period and was 163.3±0.6 mm on average, while their body weight was relatively higher, averaging 66±0.5 kg. The average height of women in old age (55–75 years) was 162.5±0.2 mm, and their body weight was 65.3±0.5 kg (Figure 1).
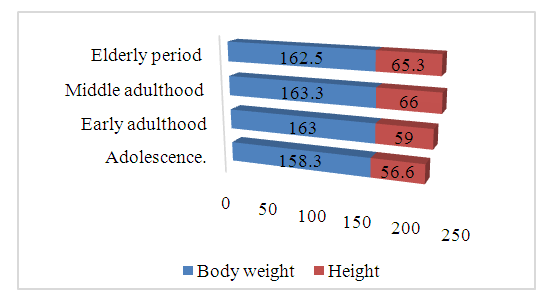 | Figure 1. Changes in height and body weight of women by age |
|
|
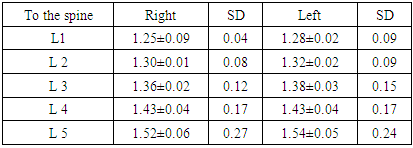
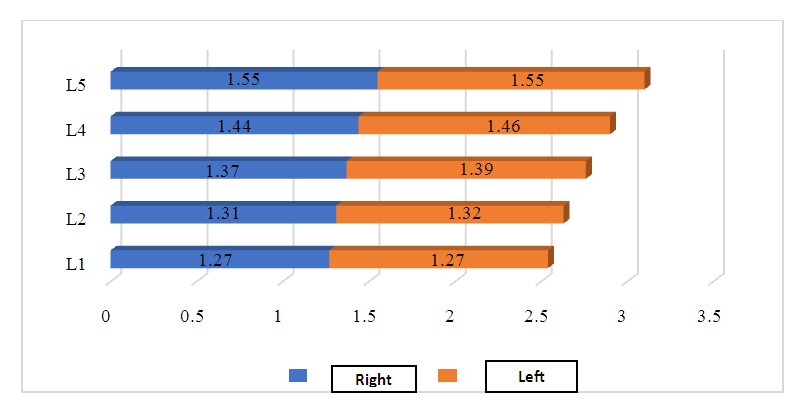 | Figure 2. Indicators of the height of the upper joint tumor in the second maturity period |
|
|
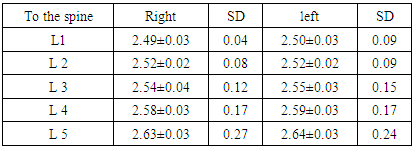
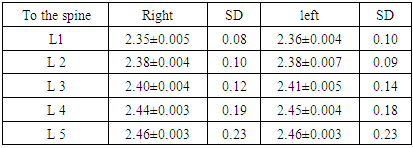
3. Discussion of the Obtained Data
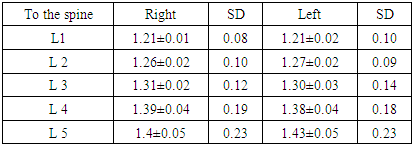
- When comparing the lumbar spine parameters of the control and main groups, all parameters of the lumbar spine of women in the main group were characterized by superiority over those of the control group, and by old age, a significant decrease in the height of the upper and lower intervertebral discs was detected compared to the previous period. A significant increase was observed in the width of the intervertebral discs, the transverse longitudinal index, and by old age. From adolescence to the second period of maturity, the height, width of the upper and lower intervertebral discs, the distance between the intervertebral discs, and their angle increased. In the study, the upper and lower intervertebral discs of the lumbar spine were measured from top to bottom, and their growth processes were studied at different periods. The results of this study analyzed the height between the right and left intervertebral discs at different ages, its variation, growth dynamics, and the tendency to decrease in old age. The upper intervertebral discs of the lumbar vertebrae have a dorsal and lateral orientation, and their surfaces are located dorsally and medially. As a result of the study, no significant difference was found between the right and left intervertebral discs, which indicates the symmetrical development of the two sides. During adolescence, the upper intervertebral discs increased on average from 1.21±0.01 cm to 1.4±0.2 cm on the right side from L1 to L5. On the left side, the average values increased from 1.21±0.02 cm to 1.43±0.05 cm and did not differ significantly from those on the right. The coefficient of variation of height was found to vary from 6.8% to 16.8% on the right side, and from 8.5% to 16.1% on the left side. During the first puberty, height on the right side increased from 1.25±0.009 cm to 1.52±0.05 cm from L1 to L5, and from 1.28±0.02 to 1.52±0.05 cm on the left side. Between adolescence and the first puberty, the growth rate increased from 3% to 9%. During the second puberty, an unreliable change was found compared to the previous period, with height on the right side increasing on average from 1.27±0.007 cm to 1.55±0.06 cm. Similar results were observed on the left side. In old age, the height of the joint growths decreased significantly, increasing from 1.19±0.02 to 1.37±0.05 cm on the right side and from 1.20±0.02 to 1.38±0.05 cm on the left side. No reliable differences were observed between right and left joint tumors during this period either. Lower joint tumors also showed similar growth and decline trends as upper joint tumors. The lower articular processes are directed downwards and outwards, and their surface faces outwards and forwards. During adolescence, the lower joint masses increased from L1 to L5 on the right side from 2.35±0.05 to 2.462±0.003 cm, and on the left side from 2.36±0.004 to 2.46±0.003 cm. No significant differences were found on either side. During the first maturation period, the lower joint masses increased from 2.49±0.03 to 2.63±0.03 cm on the right side and from 2.50±0.03 to 2.64±0.03 cm on the left side. During the second maturation period, similar growth was observed in the lower joint masses as in the upper joint masses. On the right side, it increased from 2.54±0.005 to 2.69±0.007 cm, and on the left side, it increased from 2.55±0.006 to 2.7±0.01 cm. In old age, the lower joint height decreased significantly compared to previous periods, from 2.50±0.02 to 2.64±0.02 cm on the right side and from 2.50±0.02 to 2.64±0.05 cm on the left side. According to the results of the study of the second group of women, the height of the joint height in women who regularly took the vitamin D Nycomed product and played sports achieved stability, which allowed them to significantly grow in bone structures and not suffer from various diseases even as they grew older. In particular, those who took vitamin D maintained higher bone density than those who did not. The height of the lumbar spine increases from adolescence to the second stage of puberty and decreases until old age. These changes in bone structure change with age and require bone health measures. Taking vitamin D and regular physical activity can stabilize these changes and reduce the risk of disease.
4. Conclusions
- 1. When we studied the structure of the facet joint, 2 different types were distinguished: the flat shape of the joint surface; the upper articular surface is convex and the lower articular surface is concave, at this time the shape of the articular groove is S–shaped.2. In women, as they age, the parameters of the lumbar spine change and the asymmetry on both sides increases. Age-related changes are manifested in a decrease in the height and width of the articular processes of the lumbar vertebrae, as well as in the distance between the vertebrae. The diameter of the vertebral foramina, articular surfaces. An increase in the cross-sectional areas of the vertebral foramina is observed. These changes are most pronounced in old age.3. There are flat, flat, and convex types of articular growths in the lumbar spine, and the clinical significance of the shape of the articular growth surfaces should be taken into account.4. As we age, the shape of joint structures changes, which affects joint mobility. These changes can lead to limitations in movement, chronic diseases, and poor posture.5. It has been observed that in women, the transition of the shape of the articular surface from flat to convex leads to the development of inflammatory diseases and degenerative changes.