-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(3): 542-546
doi:10.5923/j.ajmms.20251503.11
Received: Jan. 29, 2025; Accepted: Feb. 20, 2025; Published: Mar. 8, 2025

Oral Hygiene in Patients with Chronic Kidney Disease Receiving and Not Receiving Hemodialysis: A Comparative Analysis of Traditional and Innovative Approaches
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhabibova N. N.1, Olimova D. V.2
1DSc., Professor, Bukhara State Medical Institute, Bukhara, Uzbekistan
2Basic Doctoral Student, Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Khabibova N. N., DSc., Professor, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Chronic kidney disease (CKD) significantly affects the dental health of patients, leading to complications such as xerostomia, uremic stomatitis, and periodontal diseases. This study analyzed 158 patients divided into three groups: the main group (hemodialysis), the comparative group (CKD without hemodialysis), and the control group. The results demonstrated that CKD patients, particularly those undergoing hemodialysis, exhibited more pronounced dental issues, including reduced salivary pH and increased viscosity. Traditional treatment methods showed moderate results, while innovative therapy using sodium bicarbonate and xylitol significantly improved oral health. Innovative treatments contributed to the normalization of pH levels, reduced inflammation, and enhanced salivation. Based on the findings, incorporating sodium bicarbonate and xylitol into clinical practice for CKD patients is highly recommended.
Keywords: Chronic kidney disease, Hemodialysis, Xerostomia, Uremic stomatitis, Sodium bicarbonate, Xylitol, Periodontal diseases, Saliva
Cite this paper: Khabibova N. N., Olimova D. V., Oral Hygiene in Patients with Chronic Kidney Disease Receiving and Not Receiving Hemodialysis: A Comparative Analysis of Traditional and Innovative Approaches, American Journal of Medicine and Medical Sciences, Vol. 15 No. 3, 2025, pp. 542-546. doi: 10.5923/j.ajmms.20251503.11.
1. Introduction
- Chronic kidney disease (CKD) is a major global health problem affecting millions of people worldwide. According to the World Health Organization, the number of patients with end-stage CKD is constantly growing, which is associated with the increasing prevalence of diabetes, hypertension and other metabolic disorders. End-stage CKD requires renal replacement therapy, the most common of which is hemodialysis [2,3,5,8].However, the impact of CKD is not limited to renal failure. This disease causes numerous systemic complications, including cardiovascular disorders, decreased immunity and changes in mineral metabolism, which directly affects the condition of the oral cavity. The oral cavity is a unique mirror of the body's condition, and its diseases can both reflect and aggravate systemic pathologies [1,5,6,7].In patients with CKD, the most common dental problems are:• Xerostomia is a severe dry mouth caused by decreased salivation. This condition occurs in more than half of patients with CKD and leads to difficulties in speaking, eating, and performing hygiene procedures [6,10].• Uremic stomatitis is an inflammation of the oral mucosa associated with the accumulation of urea and its conversion to ammonia under the action of bacterial enzymes. Uremic stomatitis causes severe irritation, ulcers and bad breath [1,13,14].• Periodontal diseases – gingivitis and periodontitis, characterized by inflammation of the gums, bleeding and destruction of periodontal tissues [2,3,11].The reasons for the development of these diseases in patients with CKD include:1. Disruption of the composition of saliva – reduction of its protective properties, change in pH and increase in viscosity.2. Systemic inflammatory processes – chronic inflammation in the body intensifies pathological changes in the tissues of the oral cavity.3. Immunodeficiency – a decrease in local and systemic immunity makes oral tissues more vulnerable to infections.4. Medication burden – patients with CKD take a large number of medications that can negatively affect the oral cavity [3,4].Particular attention should be paid to patients receiving hemodialysis. This method of therapy allows to prolong the life of patients, but it is associated with additional risks for the oral cavity. Such patients are more likely to have xerostomia and uremic stomatitis, which is associated with a violation of water-salt metabolism and the use of drugs that suppress salivation [11,13,14].Oral hygiene plays a key role in the prevention and treatment of dental diseases in patients with CKD. Regular hygiene, the use of special means for normalizing salivation and pH control, as well as the elimination of inflammatory processes can significantly improve the quality of life of these patients [7].Modern research shows the potential of using innovative approaches to treating dental problems in patients with CKD. One such approach is the use of sodium bicarbonate and xylitol. Sodium bicarbonate helps to normalize the acid-base balance in the oral cavity, reducing the risk of developing inflammatory processes. Xylitol, in turn, helps to moisturize the mucous membrane and restore salivation, and also has an antimicrobial effect.Thus, the need to study and implement innovative methods in dental practice for patients with CKD becomes obvious.The aim of the study is to examine the oral hygiene status of patients with chronic kidney disease, compare the indicators in patients receiving and not receiving hemodialysis, and evaluate the effectiveness of traditional and innovative treatment methods.
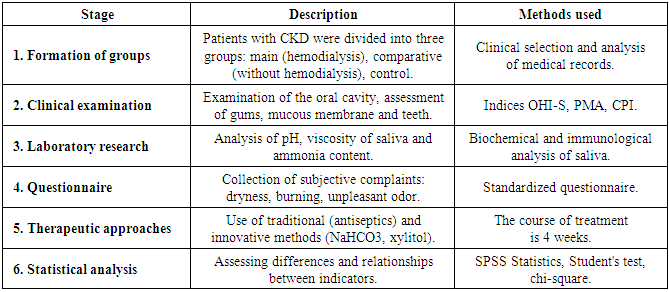
2. Methods
- This study was conducted between 2022 and 2025 at the Bukhara State Medical Institute. The main focus was on the study of the dental condition of patients with chronic kidney disease (CKD), as well as a comparative analysis of traditional and innovative approaches to treatment.Study designThe study was observational in nature with elements of a clinical experiment. To increase the reliability of the results, a cohort approach was used with the division of patients into three groups:1. Main group: patients with CKD receiving hemodialysis.2. Comparison group: patients with CKD not receiving hemodialysis.3. Control group: healthy volunteers without systemic diseases.Participants of the studyThe study involved 158 people, of whom:• 108 patients made up the main group (hemodialysis);• 30 patients – comparative group (CKD without hemodialysis);• 30 people – control group.Inclusion criteria:• Age from 18 to 75 years.• Diagnosis of chronic kidney disease (confirmed by medical documents).• Consent to participate in the study.Exclusion criteria:• Oncological and autoimmune diseases.• Pregnancy and lactation period.• Surgical interventions less than 6 months before the study.• Failure to comply with oral hygiene recommendations.Survey methodsThe examination included clinical, laboratory and instrumental methods for assessing the condition of the oral cavity.1. Clinical methods:ο Examination of the oral cavity using a dental mirror and probe.ο Assessment of the condition of the gums, mucous membrane and teeth.ο Measuring oral hygiene indices:§ OHI-S (Oral Hygiene Index – Simplified): to assess the degree of dental plaque.§ PMA (Papillary-Marginal-Attached Index): For ratings inflammations gums.§ CPI (Community Periodontal Index): to detect periodontal diseases.2. Laboratory tests:ο Biochemical analysis of saliva: determination of pH, viscosity and ammonia content.ο Immunological analysis: assessment of levels of proinflammatory cytokines (IL-6, IL-8) and immunoglobulins (IgA, IgG, IgM).3. Survey:ο Patients completed questionnaires to record complaints such as dry mouth, burning sensation, bad breath, and discomfort when eating.4. Instrumental methods:ο Using a portable pH meter to measure the acidity of saliva.ο Conducting saliometry using the Pozharsky method to assess the volume of salivation.Treatment methodsPatients of the main and comparative groups were divided into two subgroups:1. Traditional therapy:ο Use of antiseptic solutions (0.05% chlorhexidine) for rinsing the mouth.ο Professional hygiene: removal of soft plaque and tartar.2. Innovative therapy:ο Use of sodium bicarbonate in the form.ο Use of xylitol spray (3 sprays three times a day).Patients underwent treatment for 4 weeks, after which they were re-examined to assess the dynamics of the indicators.Statistical analysisAll obtained data were processed using IBM SPSS Statistics version 23 software. To assess the reliability of differences between groups, the following were used:• Student's t-test for comparing quantitative data.• Chi-square test for qualitative data analysis.• Correlation analysis to identify relationships between clinical and laboratory parameters.The level of statistical significance was set at p < 0.05.
|
3. Results
- The study analyzed data from 158 participants, including 108 patients in the main group (hemodialysis), 30 patients in the comparison group (CKD without hemodialysis), and 30 people in the control group. The results confirmed the significant impact of chronic kidney disease on the dental health of patients.The most common disorder among patients with CKD was xerostomia. This symptom was observed in 78.7% of patients in the main group, which is significantly higher compared to the comparative group, where the frequency was 63.4%. In the control group, xerostomia was completely absent. Uremic stomatitis also turned out to be widespread among patients with CKD: its signs were detected in 62.3% of participants in the main group and in 47.8% of patients in the comparative group. Periodontal diseases, such as gingivitis and periodontitis, were recorded in 54.1% of patients in the main group and in 39.6% of patients not receiving hemodialysis (Diagram 1).
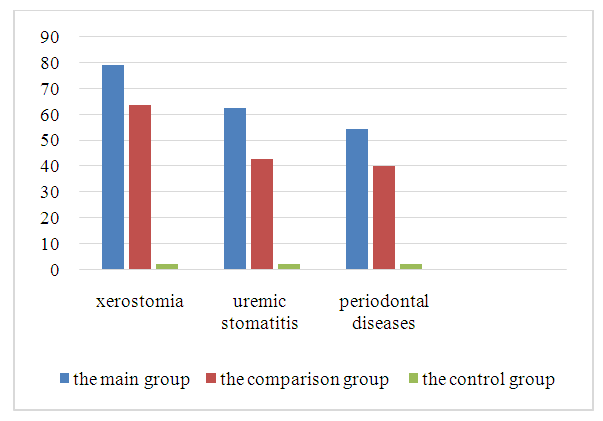 | Diagram 1. Frequency of dental disorders |
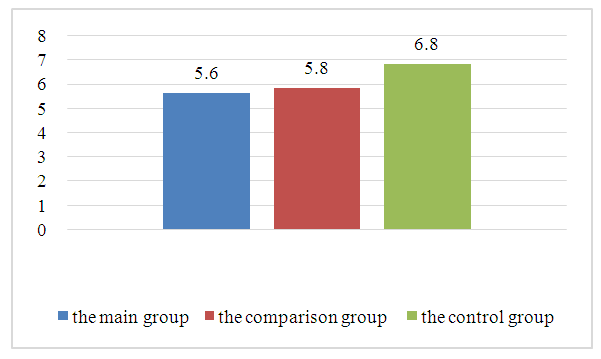 | Diagram 2. Average pH level of saliva |
4. Discussion
- The results of the study confirmed that chronic kidney disease, especially at the end stage, has a significant impact on the oral health of patients. In individuals receiving hemodialysis, oral problems such as xerostomia, uremic stomatitis and periodontal disease were significantly more common than in CKD patients without hemodialysis. These findings are consistent with the results of previous studies indicating a link between systemic disorders in CKD and oral health.The main factor worsening the oral cavity condition in patients with CKD is the change in the composition and properties of saliva. Reduced salivation, increased viscosity, and decreased pH create a favorable environment for the development of inflammatory processes and bacterial growth. In the group of patients receiving hemodialysis, these changes were most pronounced, which is probably due to the additional metabolic loads caused by the dialysis procedure.An interesting finding was the difference in the effectiveness of traditional and innovative treatment methods. Traditional approaches based on the use of antiseptic solutions showed moderate results, which emphasizes the need to find new solutions to improve the oral health of such patients. The use of sodium bicarbonate and xylitol demonstrated high clinical effectiveness. This can be explained by their ability to normalize oral pH, stimulate salivation and reduce inflammatory processes.Sodium bicarbonate, with its pronounced alkaline properties, effectively neutralizes acidity in the oral cavity, which helps reduce the risk of enamel demineralization and inflammation. Xylitol, in turn, acts as a moisturizing and antimicrobial agent, restoring the protective functions of saliva and preventing the proliferation of pathogenic microorganisms. These properties make the combination of sodium bicarbonate and xylitol a promising solution for improving the dental health of patients with CKD.It is also important to note that patients who received the innovative treatment noted a significant improvement in their general well-being after just two weeks. This indicates a rapid and pronounced effect of the therapy, which increases its clinical significance.Based on the data obtained, it can be concluded that the dental health of patients with CKD requires a comprehensive approach, including:1. Regular monitoring of the oral cavity condition and preventive measures.2. Using innovative methods such as sodium bicarbonate and xylitol to normalize pH and improve salivation.3. Teaching patients oral hygiene rules, taking into account their systemic condition.The introduction of such approaches into clinical practice will not only improve the oral health of patients with CKD, but also improve their overall quality of life.
5. Conclusions
- The results of the study confirmed that chronic kidney disease, especially at the terminal stage, has a significant impact on the oral cavity, increasing the risk of xerostomia, uremic stomatitis and periodontal diseases. These changes are most pronounced in patients receiving hemodialysis, which is associated with additional metabolic disorders and treatment features.Biochemical studies have shown that decreased pH of saliva and increased viscosity are key factors contributing to the deterioration of dental status in patients with CKD. These changes create a favorable environment for inflammatory processes and the growth of pathogenic microorganisms.A comparative analysis of traditional and innovative treatment methods demonstrated the high efficiency of therapy using sodium bicarbonate and xylitol. These agents helped normalize the acid-base balance, improve salivation and reduce inflammatory processes. Patients who received this treatment noted a significant improvement in the condition of the oral cavity within two weeks of starting therapy.Based on the conducted research, the following conclusions can be drawn:1. Patients with chronic kidney disease, especially those on hemodialysis, need regular monitoring of their dental health.2. The use of sodium bicarbonate and xylitol in complex therapy of the oral cavity demonstrates high clinical significance and can be recommended for use in dental practice.3. To improve the quality of life of patients with CKD, it is important to introduce innovative methods of prevention and treatment of dental diseases, as well as to teach patients the rules of oral hygiene.Further research in this area should be aimed at studying the long-term effects of the proposed therapy and its impact on the systemic state of patients.