-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(2): 470-472
doi:10.5923/j.ajmms.20251502.43
Received: Jan. 22, 2025; Accepted: Feb. 17, 2025; Published: Feb. 28, 2025

Hypertension as a Complication in Cerebrovascular Diseases: Morphological Changes in Intracerebral Blood Vessels
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbduolimov A. A.1, Mamajanov B. S.2
1Fergana Public Health Medical Institute, Uzbekistan
2Andijan State Medical Institute, Uzbekistan
Correspondence to: Abduolimov A. A., Fergana Public Health Medical Institute, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Hypertension-induced atherosclerosis leads to stenosis of medium and small-caliber blood vessels in the brain, ultimately resulting in ischemic necrosis in the affected area. In particular, atherosclerosis caused by hypertension manifests as vascular deformations such as aneurysms and stenosis. In many cases, hypertension-associated atherosclerosis presents with bilateral metabolic disturbances and stromal vascular dystrophy, leading to characteristic cerebrovascular damage. The development of atheromatous changes in the endothelial and subendothelial layers of blood vessels results in luminal narrowing, which contributes to ischemic processes.
Keywords: Cerebrovascular disease, Atherosclerosis, Atheromatosis, Morphology, Hypertension
Cite this paper: Abduolimov A. A., Mamajanov B. S., Hypertension as a Complication in Cerebrovascular Diseases: Morphological Changes in Intracerebral Blood Vessels, American Journal of Medicine and Medical Sciences, Vol. 15 No. 2, 2025, pp. 470-472. doi: 10.5923/j.ajmms.20251502.43.
1. Introduction
- Research based on global population studies indicates that, over the past forty years, cerebral ischemia and encephalomalacia have been most frequently observed in individuals aged 49 to 55 [1,2,4]. Considering that 70-75% of cerebrovascular pathologies are influenced by hypertension and obesity, the incidence of atherosclerosis in the arteries forming the Circle of Willis has been linked to various neurological and cognitive impairments [3,12]. Studies suggest that 40-56% of cerebrovascular diseases are associated with atherosclerosis in the Circle of Willis [5,6,7,8].The localization of atherosclerotic lesions contributes to varying degrees of vascular damage: the anterior communicating and anterior cerebral arteries are affected in 40-50% of cases, the internal carotid and posterior communicating arteries in 15-20%, the middle cerebral artery in 15-20%, the basilar and posterior cerebral arteries in 5%, and other arteries in 4-9% of cases [9,10,11,13,14].
2. Discussion and Results
- In patients with hypertension, progressive arterial narrowing, exacerbated by chronic hemodynamic disorders in the Circle of Willis, is commonly observed after the age of 50-55, particularly under stress-related conditions. The narrowing of blood vessels leads to chronic hemodynamic disturbances, resulting in lipid plaque accumulation in the endothelial layer. As this process intensifies, atheromatous changes in the subendothelial layer lead to intimal damage, which in turn facilitates the formation of atherosclerotic plaques and further vascular lumen reduction.
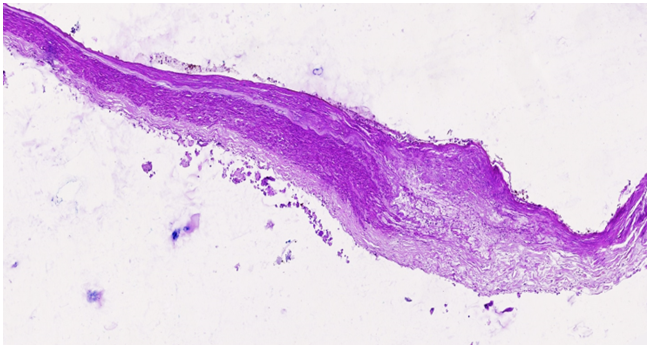 | Figure 1. The right cerebral artery wall shows an atherosclerotic plaque with an underlying atheromatous mass. The endothelial surface of the plaque varies in appearance, acting as a primary factor in thrombogenesis. Sclerotic changes are evident in the muscle layer. Staining: H.E. Magnification: 4x10 |
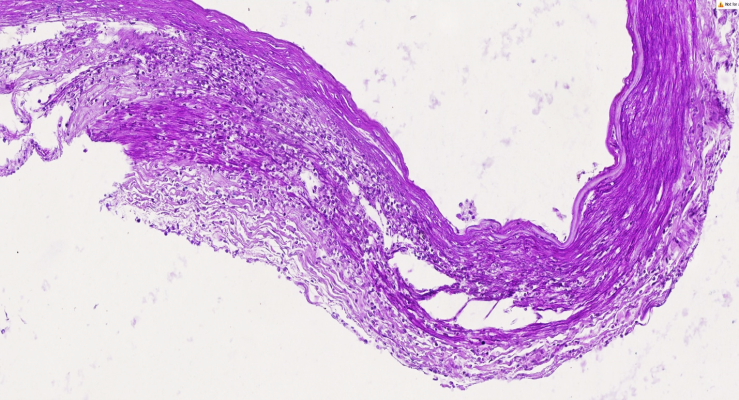 | Figure 2. The right cerebral artery exhibits an atherosclerotic plaque with myolysis and macrophage infiltration in the medial layer. The endothelial surface of the plaque presents diverse structural variations, contributing to thrombogenesis. The muscle layer has developed sclerotic changes. Staining: H.E. Magnification: 10x10 |
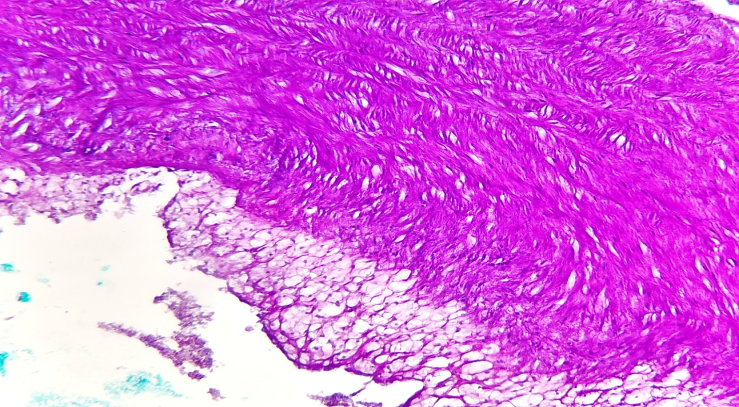 | Figure 3. The right cerebral artery displays an atherosclerotic plaque with a lipid deposit. The medial layer shows sclerotic changes with disorganized coarse fibrous structures. The endothelial surface of the plaque varies, serving as a primary factor in thrombogenesis. The muscle layer exhibits advanced sclerosis. Staining: H.E. Magnification: 40x10 |
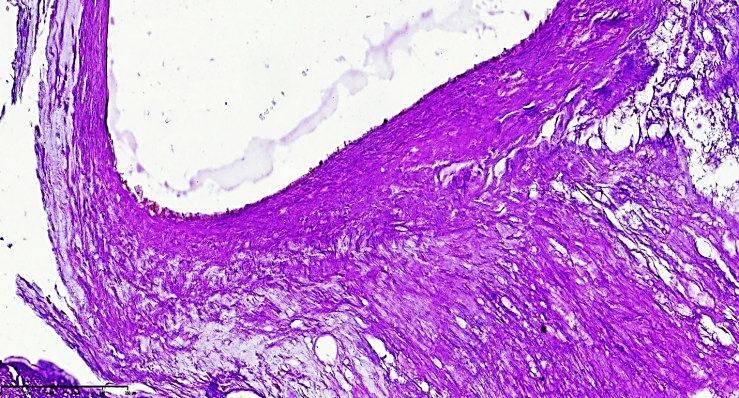 | Figure 4. Post-atherosclerotic myofibrosis and atheromatous foci are observed in the right cerebral artery. The vascular histoarchitecture is significantly altered, consisting mainly of coarse fibrous connective tissue due to sclerosis. The endothelial surface of the plaque remains irregular, contributing to thrombogenesis. Staining: H.E. Magnification: 40x10 |
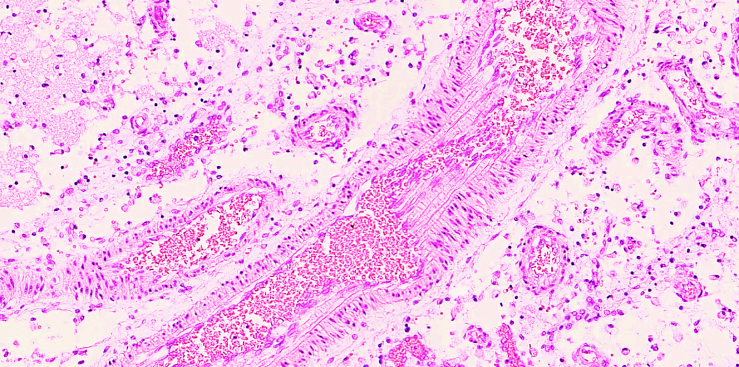 | Figure 5. Secondary branch of the right cerebral artery displaying an atherosclerotic plaque and varying wall thickness. A stenotic focus is identified. Staining: H&E, Magnification: 20×10 |
3. Conclusions
- One of the primary vascular changes in hypertension is the development of atherosclerosis, leading to narrowing of the cerebral arteries. Hypertension induces dystrophic and sclerotic changes in the vessel walls, resulting in sequential structural damage and the formation of atheromatous plaques. The destruction of collagen and elastic fibers leads to atherosclerosis, characterized by elastolysis, collagenolysis, and fibromuscular dysplasia. The Circle of Willis, particularly the anterior communicating artery, is most affected, undergoing significant structural remodeling characteristic of atherosclerotic pathology.