-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(1): 228-231
doi:10.5923/j.ajmms.20251501.44
Received: Dec. 16, 2024; Accepted: Jan. 12, 2025; Published: Jan. 27, 2025

Omega-3 Supplementation in Combination Therapy for Anorexia Syndrome in Metastatic Breast Cancer
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRakhimov N. M., Shakhanova Sh. Sh., Tulanov B. T.
Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective: To evaluate the efficacy of omega-3 fatty acids combined with megestrol acetate in managing cancer-related weight loss in breast cancer patients. Material and methods: A randomized clinical trial was conducted with 111 breast cancer patients experiencing significant weight loss. Subjects were divided into three treatment groups: Group 1 (n=34): Megestrol acetate (800 mg/day); Group 2 (n=35): Prednisolone (30 mg/day); Group 3 (n=42): Combined therapy of megestrol acetate (400 mg/day) plus omega-3 fatty acids (1.6 g/day). Parameters measured: appetite improvement, weight gain, overall quality of life metrics. Results: The combination therapy group demonstrated superior outcomes: 73% showed appetite improvement vs. 60-63% in monotherapy groups. 71% achieved significant weight gain. 50% reported enhanced quality of life compared to 20% in other groups. Conclusion: The study suggests that combined therapy with omega-3 and reduced-dose megestrol acetate provides more effective weight management with fewer adverse effects compared to standard monotherapy approaches in breast cancer patients. These findings indicate potential therapeutic advantages of incorporating omega-3 supplementation into weight management protocols for cancer patients.
Keywords: Breast cancer, Anorexia, Megestrol acetate, Omega-3, Combination therapy
Cite this paper: Rakhimov N. M., Shakhanova Sh. Sh., Tulanov B. T., Omega-3 Supplementation in Combination Therapy for Anorexia Syndrome in Metastatic Breast Cancer, American Journal of Medicine and Medical Sciences, Vol. 15 No. 1, 2025, pp. 228-231. doi: 10.5923/j.ajmms.20251501.44.
1. Introduction
- Anorexia in cancer significantly worsens the quality of life of patients and can shorten its duration, especially in the late stages of cancer. Various drugs have been actively studied to combat this condition [6,7,9].Corticosteroids were among the first drugs used to treat anorexia in cancer patients. In 1974, Moertel and colleagues conducted the first placebo-controlled study that showed that corticosteroids temporarily improve appetite in patients with advanced cancer [8]. However, subsequent studies have confirmed that these drugs do not contribute to weight gain [10].In 1990, the first study of the effectiveness of megestrol acetate was conducted. This drug has shown good results in stimulating appetite in patients with anorexia or cachexia caused by cancer or AIDS [4]. Studies with different dosages determined the optimal daily dose of 800 mg. In addition to improving appetite, megestrol acetate contributed to weight gain: in some patients, the weight gain ranged from 9 to 14 kg without signs of fluid retention [2].Comparative analysis showed that megestrol acetate is more effective than corticosteroids in stimulating appetite. In addition, it has a more favorable security profile. Unlike corticosteroids, megestrol acetate does not cause stomach ulcers, cataracts, myopathy, or glucose tolerance disorders. There was also no suppression of adrenal function, which precludes the need to gradually reduce the dosage after the end of therapy [1,3].Studies have shown that megestrol acetate has advantages over corticosteroids in the treatment of anorexia and cahex II in acute cancer patients. However, its high cost has become a significant limitation. Treatment with corticosteroids cost less than one dollar a day, while the daily intake of megestrol acetate was several times more expensive. Following a successful trial of megestrol acetate conducted by the North Central Cancer Treatment Group (NCCTG), a survey of oncologists was conducted. The results showed that doctors were divided in their opinions: some preferred megestrol acetate, while others chose more affordable corticosteroids [3,10].Objective: to determine the most effective method for correcting anorexia syndrome in disseminated breast cancer.
2. Materials and Methods
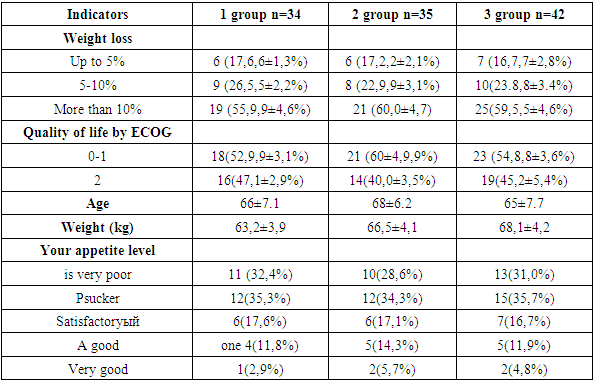
- The study involved adult patients with incurable breast cancer. The selection criteria included losing at least 2.3 kg in 6 months (not due to surgery) or consuming less than 20 calories per kg of body weight per day. Life expectancy was predicted from 6 months and ECOG status to 2.Patients with ascites, intestinal obstruction, malabsorption, persistent vomiting, on probe or intravenous nutrition were excluded. Patients with brain metastases, thrombosis in the last 6 months, poorly controlled hypertension, or heart failure were also excluded. The study did not include pregnant women, nursing mothers, patients with cataracts, insulin-dependent diabetes, stomach ulcers, or opportunistic infections.The distribution took into account the location of the tumor, the degree of weight loss, ECOG status, planned treatment, and survival prognosis. Patients were divided into three groups: the first group n=34 (n=34patients) received megestrol acetate 800 mg/day, the second (n=35) - prednisone 30 mg/day, the third (n=42) больных- мегестеролmegesterol acetate 400 mg / day and omega-3 1.6 gy/day. If poorly tolerated, the dose could be reduced by half. Indicators of basic characteristics in the compared groups are provided in table 1. In our study, we made several key measurements. When evaluating the effect of treatment on patients ' appetite, the binomial test revealed 75% power, with a difference of 20% between the groups.
|
3. Results
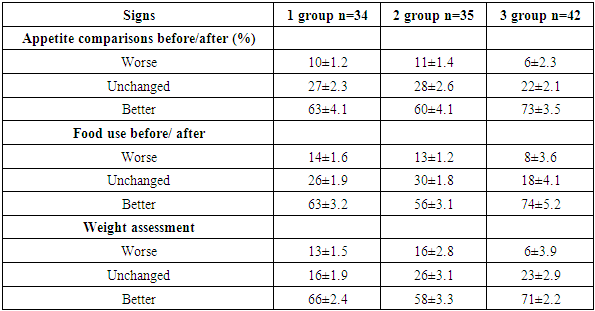
- After 3 months of taking megestrol acetate showed better results than prednisone. The effectiveness of prednisone was similar to megestrol acetate, while both groups were statistically inferior to the combination of megestrol acetate+omega-3. In patients who took these two drugs, an improvement in appetite was noted by 60-70% of participants.When analyzed by the "intent-to-treat" method, a positive effect was observed in 37-42% of all patients. The O'Brien test showed a clear superiority in the combination of megestrol acetate+omega-3 (P = 0.003), and megesterol monotherapy prevailed мегестеролаover prednisone (P = 0.0045).For the three control measures (weight loss+quality of life+appetite level), the median improvement was: megestrol acetate-4.33, prednisone-4.13 (P = 0.45), and the combination of megesterol+omega-3 – 4.9 (P = 0.0048). Significant improvement in all three parameters was observed in 52% of patients on megestrol+omega3-, 22% on монотерапии megestrol monotherapy (P = 0.003) and 17% on prednisone (P = 0.0041). These results confirm the highest efficacy of megestrol acetate+omega-3.
|
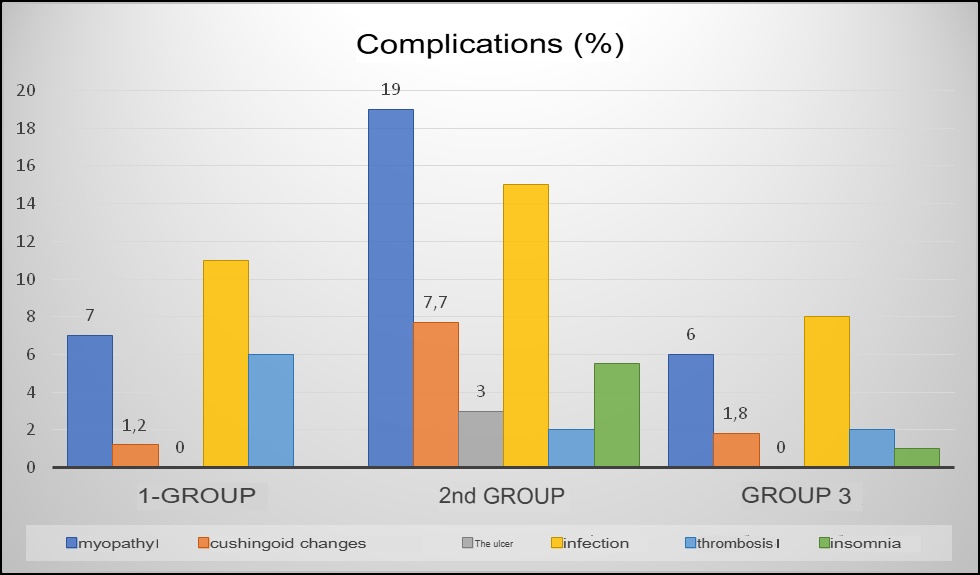 | Figure 1. Assessment of complications in the compared groups |
4. Conclusions
- The study showed that the combination of megestrol acetate and omega-3 fatty acids is the most effective treatment for anorexia in patients with disseminated breast cancer. Patients treated with megestrol acetate in combination with omega-3s showed significant improvements in appetite, weight gain, and quality of life compared to groups treated with megestrol acetate or prednisonealone. In addition, combination therapy was characterized by a more favorable safety profile, with fewer side effects, such as myopathy, kushingoid changes and peptic ulcer disease, compared with монотерапией prednisone monotherapy. The results of the study suggest that the addition of omega-3 fatty acids to megestrol acetate may be an effective approach to correcting anorexia in patients with advanced breast cancer.