-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(1): 188-192
doi:10.5923/j.ajmms.20251501.36
Received: Dec. 19, 2024; Accepted: Jan. 16, 2025; Published: Jan. 27, 2025

Pathomorphological Changes Developing in the Stenosing Variant of Esophageal Atresia in Infants
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLErkin A. Eshbaev1, Aziz A. Zufarov2, Makhzuna Kh. Mukhsinova3
1DSc, Associate Professor, Department of Pathological Anatomy, Tashkent Medical Academy, Tashkent, Uzbekistan
2DMS, Associate Professor, Department of Propaedeutics of Childhood Diseases and Hematology, Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
3PhD, Associate Professor, Head of the Department of Therapeutic No.1, Tashkent State Dental Institute, Tashkent, Uzbekistan
Correspondence to: Makhzuna Kh. Mukhsinova, PhD, Associate Professor, Head of the Department of Therapeutic No.1, Tashkent State Dental Institute, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Although the clinical and morphological frequency of atresia, which is the 4th variant of esophageal malformation and continues mainly with esophageal wall stenosis, is relatively low, in most cases patients experience a sudden decrease in quality of life. Morphologically, all anatomical walls of the esophagus of this type contain formed tissue components mainly in those areas that have not undergone stenosis, and in those areas where stenosis is detected, areas that have undergone dysplasia in the esophageal wall are identified. In particular, myodysplasia on the muscular bottoms is characterized by the fact that there are very few alveolar tubular glands on the mucosa and mucous membranes, there are 1-3-layered cuboid and prismatic epithelium on the surface of the mucous membrane, as well as cuboid epithelium cells that undergo metaplasia.
Keywords: Esophageal atresia, Stenosis, Morphology, Dysplasia, Morphological paralysis
Cite this paper: Erkin A. Eshbaev, Aziz A. Zufarov, Makhzuna Kh. Mukhsinova, Pathomorphological Changes Developing in the Stenosing Variant of Esophageal Atresia in Infants, American Journal of Medicine and Medical Sciences, Vol. 15 No. 1, 2025, pp. 188-192. doi: 10.5923/j.ajmms.20251501.36.
Article Outline
1. Introduction
- Anomalies in the development of the esophagus are a process in the embryonic period that continues the development of the esophagus and its structural formations with anatomical and histological changes. Worldwide the development of this pathology corresponds to 40 out of 100,000 infants. The detection of this pathology during early pregnancy screening in the United States and European countries, based on strict guidelines for termination of pregnancy, has an average incidence rate of 4-8 per 100,000 infants [4,6,15,16]. While the incidence of these pathologies in the CIS countries, including the Russian Federation, is 20-25 cases per 100,000, in the Republic of Uzbekistan this figure is 8-10 cases per 1,000 infants, which is manifested by a high mortality rate of an average of 60-78% of cases within a month after the birth of infants [3,5,9,17]. Currently, this issue is a problem for both pediatricians and neonatologists, since, according to foreign literature and anamnestic data, the incidence is 2.5 times higher in infants born to relatives with a higher genetic predisposition [10,11,13,18]. It is the fact that mortality in combined bronchoesophageal adhesions and oesophageal malformations exceeds 85% that causes infants to die from aspiration pneumonia in the early days of the early neonatal period [1,7,8,12,14]. This, in turn, requires focusing on the morphological aspects of finding a solution to the problem and developing methods for the expression of mutated genes and targeted therapy based on molecular genetic testing.
2. Materials and Methods of Research
- As a material for the formation of materials for the autopsy of infants who died as a result of abnormalities in the development of the esophagus, and infants who underwent surgery on the esophagus and died without it. In 18 cases, esophageal contents were taken from them. The finished samples were examined morphologically. Morphology: hematoxylin was stained with eosin dye.
3. Research Aim
- The study of specific pathomorphological changes that occur in the clinical and morphological variant of 3 anomalies of the esophagus.
4. Discussion and Conclusions
- The 4th variant of esophageal atresia. The main morphological changes are atresia of the proximal trachea and esophagus, the total atresia of the esophagus is 2%. In this variant, the wall of the esophagus has dysplasia and a section of stenosis, and the patency of the esophagus is morphofunctionally impaired. In this species, esophageal atresia is incomplete and semi-permeable and can occur in the proximal, distal, and middle triads.We remind that the development of esophageal atresia is explained by the fact that in this 4th variant, if we take into account the development of esophageal atresia along with other systemic tissues around the complex or in the alloxide, the wall of the esophageal stenosed area is not fully formed in the perinatal development of anatomical layers, mainly morphofunctional parameters of the mucous membrane.The fact that the MALT structure located on the mucous and submucosa is not fully formed, and the number of intraepithelial lymphocytes is significantly reduced, means that primary and acquired immunodeficiency occurs on average in 30% of children born with this defect.
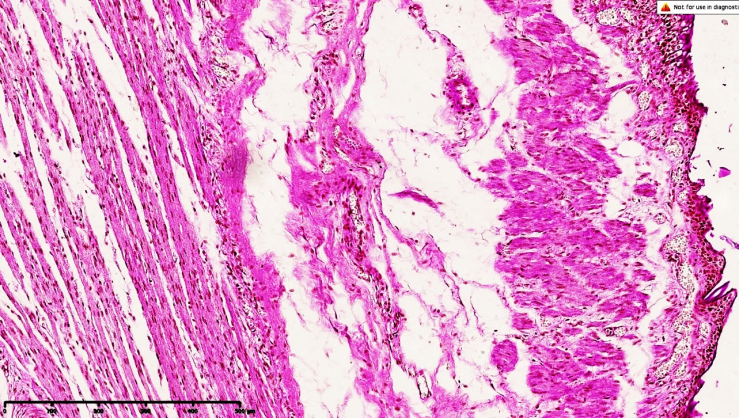
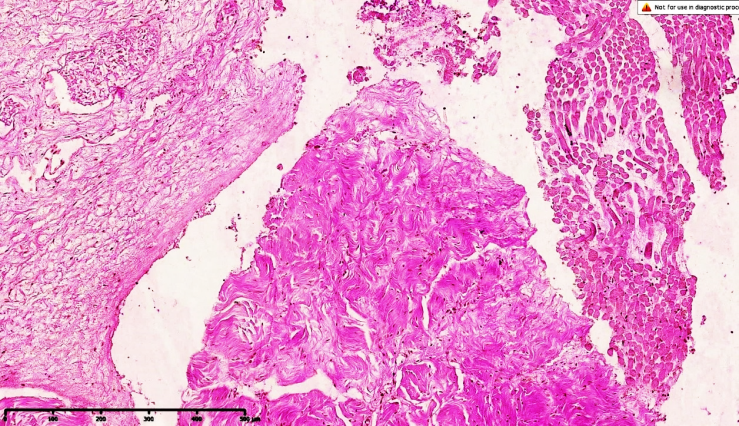 | Figure 1. Esophageal atresia in variant 4, morphological view of the upper part. Foci of trembling of transverse muscle bundles are found along the perimeter of the esophageal junction, and an increase in connective tissue components from sparse fibers is observed in the gap |
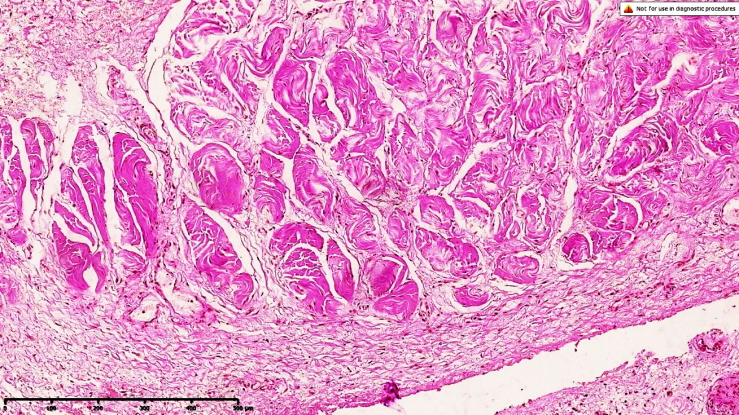 | Figure 2. Esophageal atresia in variant 4, foci of myofibrosis form between the transverse muscle bundles, the upper end of which is located on the muscular floor, elastic fibers in the adventitial floor tremble, interstitial edema in the lumbar region, there are signs of overflow of small-caliber blood vessels. Dye G.E. Is 10x10 in size |
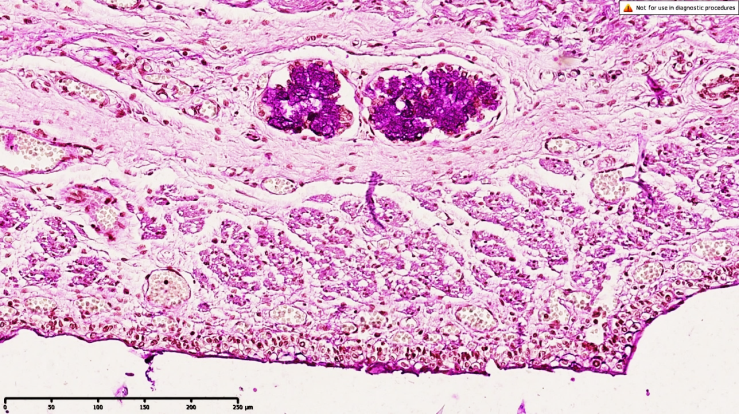 | Figure 3. Esophageal atresia in variant 4, tubular alveolar glandular tissue with a middle tip located on the mucous membrane, surrounded by sparse fibrous connective tissue forming a border around the perimeter of the gland, confirms the low morphofunctional activity of the gland, the presence of a small number of scattered intraepithelial lymphocytes on the mucous membranes and mucous membranes of the mucous membranes is determined. Intermediate tumors form at all anatomical levels, and the proliferation of connective tissue with sparse fibers is determined at all anatomical levels. On the surface of the mucous membrane, it is determined that the epithelial coating is not fully formed. Figure is 10x10 in size. The remaining areas of the mucous membranes appear to be formed in accordance with gestational age, and it is determined that these are multilayer squamous epithelial cells. At the borders of the enlarged and stenosed mucosa, a multilayer epithelial coating 200 times larger was found, consisting in appearance of 1-3 layers, with single-layered semi-prismatic and cuboid epithelial cells in the border area |
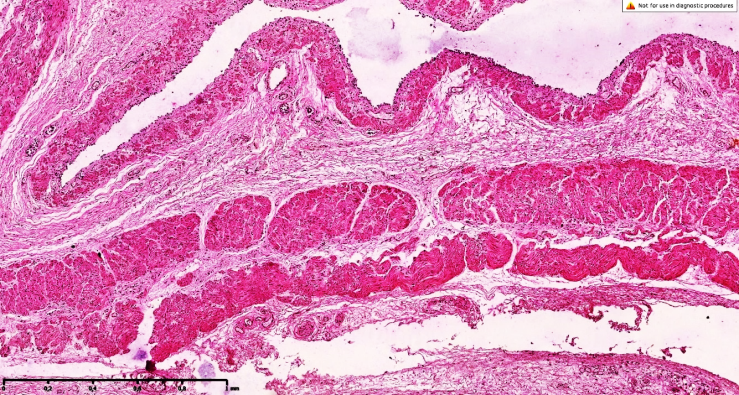
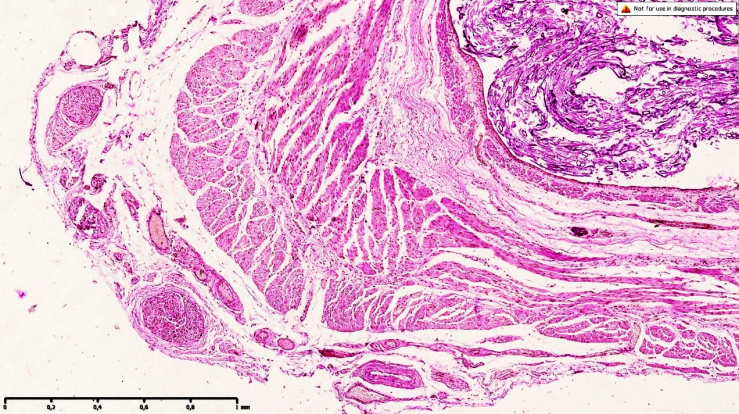 | Figure 4. Esophageal atresia in variant 4, morphological type of the middle triad. The thickness of the muscle layer of the esophagus is different, it is in the zones of myofibrosis and myosclerosis that foci of connective tissue are detected, revealing coarse fibrous tachylaxis, mucosa and mucus-like membranes of different thickness, on the adventitial floor there is a sharp fullness and preserved foci of unformed muscle rudiments. On the surface of the mucous membrane, it is determined that the epithelium is not fully formed. Dye G.E. Is 4x10 in size |
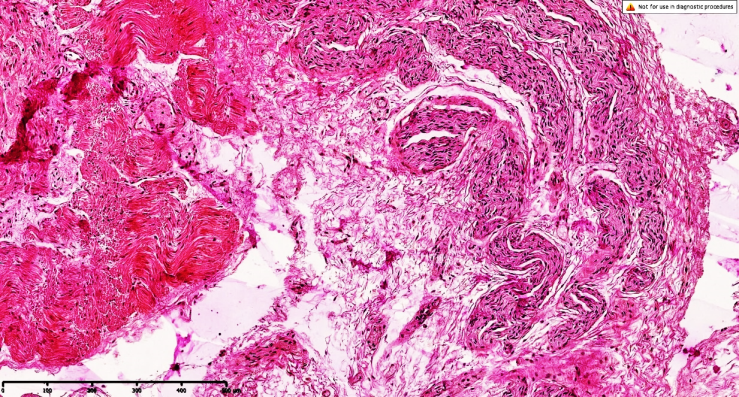
 | Figure 5. Esophageal atresia in variant 4, morphological appearance of the middle triad. Foci of inflammatory infiltrate in the mucomuscular bottoms and areas of myofibrosis in the muscles are detected in the wall of the esophagus, and the histoarchitectonics of muscle tissue can be traced along the pelvis, with a sharp development of intermediate tumors around it, components of sparse fibrous connective tissue are isolated, trembling along the perimeter of the muscle bundles. identified. The surface of the mucous membrane has uneven thickness, which exactly corresponds to the areas where it undergoes stenosis. A general dye staining is 10x10 in size |
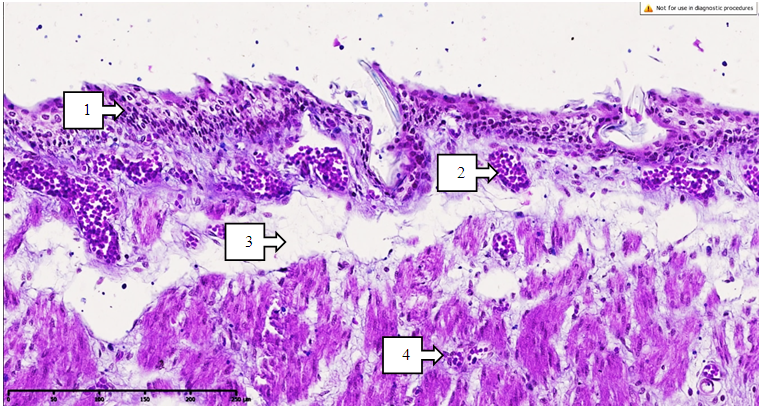 | Figure 6. Esophageal atresia in variant 4, the area of the middle triad is the surface of the mucous membrane. The mucous membrane is not fully formed, it is of different thickness (1), massive thickening has developed in the blood vessels (2), interstitial tumors have developed sharply at the borders of the mucous membrane and mucous membranes (3), sparse fibrous connective tissue between the private muscles of the layer has increased on the mucous membrane, foci of lymphocytic infiltration have formed (4). Dye G.E. Is 10x10 in size |
 | Figure 7. Esophageal atresia in variant 4, morphological appearance of the middle triad. An increase in the components of sparse fibrous connective tissue is detected along the perimeter of the esophageal junction, the mucous membrane and mucous membranes are not fully formed. On the surface of the mucous membrane, it is determined that the epithelium is not fully formed. Dye is 10x10 in size |
 | Figure 8. Esophageal atresia in variant 4, morphological view of the lower part. An increase in connective tissue components with sparse fibers is detected along the perimeter of the esophageal junction, and the mucous membrane is not fully formed. On the surface of the mucous membrane, it is determined that the epithelium is not fully formed. Dye is 10x10 in size |
5. Conclusions
- Consequently, the following changes are observed in esophageal atresia in 4th variant: an increase in the sparse and coarse fibrous connective tissue between the muscle layers where the wall of the esophagus has a round and longitudinal shape, signs of impaired contractility of the muscle layers during atresia, myofibrosis, the appearance of foci of myosclerosis and thickening of the esophageal wall. They allow to strengthen the stenosis process and predict.At the same time, the presence of full-fledged venous outflows in the blood vessels of the muscular fundus allows us to assess whether peristalsis continues in the muscle layers during non-synchronous contractions. The presence of a basal layer of different thickness between the muscular and adventitial layers also confirms the morphological changes presented above.