Iriskulov B. U.1, Khusanova D. Z.2, Khusanov R. A.3
1Professor of the Tashkent Medical Academy, Uzbekistan
2MD, Independent Researcher, Republican Specialized Scientific and Practical Medical Center of Hematology, Uzbekistan
3Doctor of Philosophy (PhD) in Medical Sciences, Alfraganus University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Among thrombocytopenia, immune thrombocytopenic purpura (ITP) averages 40%, due to the formation of IgG class autoantibodies to platelet receptor glycoprotein IIb/Sha or glycoprotein IIb/IX localized on the platelet membrane [1,2]. Antiplatelet antibodies act as opsonins recognized by the Fc receptor for IgG expressed by phagocytes, which leads to increased destruction of platelets. The incidence of ITP in children is 1.9-6.4 per 100,000 per year, the frequency of chronic ITP reaches 13-36% of children [1,7]. Cytokine genes play an important role in the implementation of immune and inflammatory processes in the human body, polymorphic changes in which lead to violations of the regulation of the inflammatory process, the immune response and the development of autoimmune diseases [2,3].
Keywords:
Immune thrombocytopenic purpura, Polymorphism, Genotype
Cite this paper: Iriskulov B. U., Khusanova D. Z., Khusanov R. A., The Role of Polymorphism rs2275913 of the IL 17A Gene in the Development of Predisposition to Immune Thrombocytopenic Purpura in Children, American Journal of Medicine and Medical Sciences, Vol. 15 No. 1, 2025, pp. 123-127. doi: 10.5923/j.ajmms.20251501.22.
1. Purpose of the Study
To study the pathogenetic relationships between the polymorphism of the IL 17A rs2275913 gene and the course of immune thrombocytopenic purpura in sick children of various age groups.
2. Research Materials and Methods
In our study, polymorphism 197G>A (rs2275913) in the IL17A gene was studied and genetically analyzed in 90 patients with ITP (main group) and 85 healthy individuals (control group), aged 1 to 17 years, undergoing outpatient and inpatient treatment at the scientific and Practical Center of Hematology and Transfusiology of the Ministry of Health RUz. Of these, 51 are girls and 39 are boys. The course of ITP was determined on the basis of ICD-10. Depending on the course, patients were divided into the following groups: acute course (OT=61), chronic course (CT=9), chronic recurrent course (HRT=8) and prolonged course (CT=12) [1]. Hematological and bone marrow parameters, hemostasis parameters, and the content of immunoglobulin’s were determined. The study of polymorphism 197G>A (rs2275913) of the IL17A gene was conducted in the laboratory of the Department of Molecular Medicine and Cellular Technologies of the National Research Center of Hematology and Blood Transfusion under the supervision of MD Professor K.T. Babaev. To do this, the "SNP-express" system was used, based on the detection of mutation (polymorphism) in the human genome. To isolate genomic DNA from peripheral blood lymphocytes, a modified phenol-chloroform extraction method and a commercial RNA/DNA sorb kit from InterLabService LLC (Russia) were used. The concentrations of purified DNA were measured using a NanoDrop 2000 spectrophotometer (NanoDropTechnologies, USA) at a wavelength of A260/280 nm. The purity of all DNA samples from patients and representatives of the control group was within the range of 1.7/1.8. The polymorphism 197G>A (rs2275913) of the IL17A gene was tested on the Rotor Gene Q device (Quagen, Germany), using allele-specific PCR in Real-Time format, using a commercial kit from the company (CJSC Syntol, Russia) and GenoTechnology (Moscow, Russia) developed on the basis of primers and alleles-specific hybridization probes Applied Biosystems 2720 (USA). Statistical processing of the obtained data was carried out using the application software package "OpenEpi 2019, Version 9.3".
3. The Results and Their Discussion
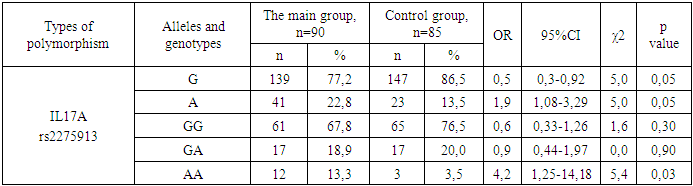
Studies of polymorphism n.197G>A (rs2275913) in the IL17A gene showed that the frequency of the wild-type allele (G) and minor allele (A) in the main group was 77.2 and 22.8%, whereas in the control group it was 86.5 and 13.5%, respectively. Similarly, the distribution of genotypes related to the 197G>A polymorphism in the IL17A gene in the main study group showed that 67.8% of children were carriers of the wild-type homozygous GG genotype, while 18.9% had the heterozygous GA genotype, and 13.3% had the homozygous GG genotype. Homozygous genotype AA. On the contrary, in the control group, these proportions were 76.5; 20.0 and 3.5%, respectively (see Table 1). The distribution of alleles and genotypes by polymorphism 197G>A (rs2275913) of the IL17A gene in a population sample and in a group of patients was checked for compliance with the Hardy-Weinberg equilibrium (RHB) using an accurate Fisher test. In the studied group of patients with ITP, there was a tendency to increase the observed frequency of the unfavorable A/A genotype compared with the expected values (0.05% vs. 0.13%, respectively). Moreover, the observed distribution of this genotype does not correspond to the expected distribution frequencies (P<0.05). The observed frequency of the normal GG genotype turned out to be statistically slightly higher than the theoretical value (0.68 versus 0.60, respectively; P>0.05). For the heterozygous G/A genotype, a very high level of theoretical heterozygosis was revealed (from 0.19 and 0.35, respectively). The observed discrepancy between the heterozygous and minor genotypes compared with the expected results suggests a potential deviation in the distribution of genotypes among children with ITP compared with the normal population distribution of the studied polymorphism. This observed deviation from the expected distribution pattern may indicate a potential association with a decrease in life expectancy, since only children were included in our study. At this age, the prevalence of heterozygous and homozygous AA genotypes may exceed expectations. We assumed that if these genotypes show a negative correlation with longevity, their proportion may decrease in older age groups and due to a decrease in the percentage of carriers of GA and AA genotypes in the population, while the wild-type genotype (GG) will increase, the observed results of polymorphism 197G>A of the IL17A gene are closer to expected the results. On the other hand, the distribution of alleles and genotypes of the 197G>A (rs2275913) polymorphism of the IL 17A gene in the control group was also checked for compliance with the Hardy-Weinberg equilibrium (HW). Polymorphism 197G/A (rs2275913) of the IL 17A gene in the control group was characterized by a very low frequency of functionally unfavorable AA genotype. In the population group, despite the distinct differences in the expected and observed frequency of the unfavorable AA genotype (0.04 vs. 0.02), statistical analysis showed that such differences are unreliable (P>0.05). The observed frequency of the GG genotype turned out to be statistically unreliably slightly higher than the theoretical value (0.76 vs. 0.75, respectively; P>0.05). The frequency of the GA genotype in the control group was unreliably higher than expected (0.20 and 0.23%, respectively, χ2 =0.42; p>0.05).Next, we analyzed the pathogenetic significance of the polymorphism 197G>A (rs2275913) of the IL 17A gene in patients (n=90) with ITP. According to the results of the odds ratio (OR — Odd Ratio) in carriers of the wild-type G allele, the probability of developing the disease statistically significantly decreased by 50% (OR=0.50, 95% CI: 0.30-0.92; χ2=5.0; p=0.05), which means that the wild-type G allele affects a statistically significant protective the role in the development of ITP. On the other hand, the minor A allele in the 197G>A polymorphism of the IL17A gene statistically significantly increases the risk of developing the disease by 90% (OR=1.90; 95% CI: 1.08-3.29; χ2=5.00; p=0.05) and proved to be a significant risk factor for the development of ITP (see Table 1).Table 1. The significance of polymorphism 197G>A of the IL 17A gene and 1142 G>A of the IL23R gene in the development of ITP in children
 |
| |
|
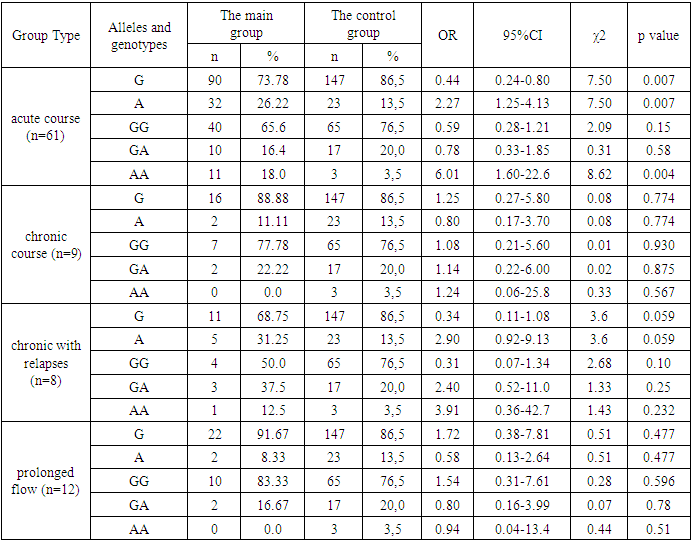
When analyzing the polymorphism 197G>A of the IL17A gene to study the pathogenetic effect of various genotypes on the development of the disease, the non-wild type AA genotype showed a 4.2-fold increase in the risk of disease (OR=4.2, 95% CI 1.25-14.18), while the homozygous GG genotype reduced this risk by 40% (OR=0.60; 95% CI 0.33-1.26). Similarly, the heterozygous GA genotype reduced the risk of developing the disease by 10% (OR=0.90; 95% CI 0.44-1.97). This means that the homozygous AA genotype plays an induced role in the pathogenesis of the disease and this result was statistically significant (χ2=5.40, p=0.03). The pathogenetic role of the heterozygous GA and homozygous GG genotypes was not statistically significant (χ2=0.00, p=0.90 and χ2=1.60, p=0.30, respectively).To clarify the significance of polymorphism of this gene on the course of ITP, we divided the sick children into subgroups: course acute (n=61), chronic (n=9), chronic with relapses (n=8) and prolonged (n=12). The analysis showed the presence of a statistically significant positive association with OTP with polymorphism of the 197 G>A minor allele (A) of the IL17A gene and the homozygous AA genotype (χ2>3.84, p<0.05). In the OT subgroup, carriers of the G allele of polymorphism 197G>A within the IL17A gene demonstrated a statistically significant protective effect against the disease, reducing susceptibility to it by 56% (OR=0.44; 95%CI: 0.242–0,800; χ2=7.50; p=0.007), whereas carriers of the A allele and homozygous genotype AA the risk of developing the disease increased statistically significantly by 2.27 times (OR=1.40; 95%CI: 0.67–2.96; χ2=7.50; p=0.007) and 6.01 times (OR=2.50; 95%CI: 0.50–12.35; χ2=8.62; p=0.004). However, statistical analysis using the chi-square criterion showed that there is no statistically significant association between the disease of OT and the genotypes GG and GA (χ2<3.84, p>0.05) (see Table 2).Table 2. The value of polymorphism 197G>A of the IL 17A gene in ITP disease with different course
 |
| |
|
In addition, we found that there is a strong statistical trend of a positive association between HRT and IL17A gene polymorphism 197 G>A (χ2=3.60, p=0.059), where carriers of the minor type A allele show an increased predisposition to the disease, with a chance ratio of 2.90 (95% CI: 0.75–32.0). Conversely, the presence of the wild-type G allele was associated with a 76% decrease in the development of the disease (OR=0.34; 95% CI: 0.110–1.082). Although the differences in the distribution of genotypes between the chronic with relapses patients and the control groups were not statistically significant (χ2<3.84, p>0.05), the chi-square test results showed a tendency to occur only the GG genotype between these groups (OR=2.40; 95%CI: 0.925-9.128; χ2=2.68, p=0.10). On the other hand, we did not find a statistically significant association between the 197 G>A polymorphism of the IL17A gene and the chronic course of ITP, as well as with the prolonged course of the disease (χ2<3.84, p>0.05).In contrast, the minor allele A of the 197G>A polymorphism of the IL-17A gene showed acceptable prognostic value for the acute course (AUC = 0.61) and excellent prognostic value for chronic with relapses (AUC= 0.82), respectively, in children. The results were statistically significant (p = 0,007). However, for primary and other subgroups, this genetic factor was not sufficient to conclude that it was a reliable predictor of disease (p>0.05).When assessing the sensitivity, specificity and prognostic effectiveness of the 197G>A polymorphism of the IL17A gene associated with the AA genotype and the GG genotype of the 1142G>A polymorphism of the IL23R gene in relation to the development of ITP in children in the main group, the following indicators were observed: for the AA genotype AUC=0.55, SE=0.86 and SP=0.23; for the GG genotype AUC=0.53, SE=0.97 and SP=0.065. In addition, the main group was divided into subgroups to assess the prognostic significance of the AA genotype of the 197G>A polymorphism in the IL17A gene and the GG genotype of the 1142G>A polymorphism in the IL23R gene. In subgroup c of the disease for the AA genotype, SE=0.18, SP=0.965 and AUC=0.64; for the GG genotype: SE=0.92, SP=0.13 and AUC=0.46. In the subgroup of children with chronic course disease for genotype AA: SE=0.00, SP=0.965 and AUC=0.87, genotype GG: SE=1.0, SP=0.13 and AUC=0.21 for. In the subgroup with chronic with relapses for the AA genotype: SE=0.125, SP=0.965 and AUC=0.89, for the GG genotype: SE=1.0, SP=0.13 and AUC=0.20. In the group of patients with chronic course disease, SE=0.00 and 0.965; SP=0.13 and 0.24, AUC=0.845 and 1.0, respectively.On the contrary, the AA genotype of the 197G>A polymorphism of the IL 17A gene demonstrated acceptable prognostic value of the acute course of ITP in children (AUC=0.64), while the result was statistically significant (p=0.004). However, for the main group and other subgroups, this genetic factor did not prove to be a reliable predictor of the disease (p>0.05).During the study, the patients included in the main group were divided into boys and girls and redistributed according to the genotypes of the 197G>A polymorphism of the IL17A gene. According to this, in the group of boys (n=40), patients with genotypes GG, GA and AA according to the polymorphism 197G>A of the IL17A gene amounted to 70.0; 20.0 and 10.0%, respectively, whereas in girls in the group (n=50) these indicators were 66.0; 18.0 and 16.0%, respectively. Although there is no statistically significant difference in the distribution of genotypes between boys and girls (χ2<3.84, p>0.05), the amount of polymorphism of the AA 197G>A genotype of the IL17A gene in girls is statistically significantly higher than the control (χ2=6.50, p=0.03).In addition, the distribution of genotypes of polymorphism 197G>A of the IL 17A gene and polymorphism 1142 G>A of the IL23R gene in patients of the main group was rearranged depending on the age index in children given by WHO. According to the results, in children under 3 years of age (early age – n=9), the percentage of GG, GA and AA genotypes of the 197G>A polymorphism of the IL17A gene was 55.56; 11.11 and 33.33%, respectively. And the percentage of GG, GA and AA genotypes in children 3-7 years old (preschool age – n=43) was 69.76; 18.60 and 11.62%, respectively. In children aged 7-14 years (primary school age – n=31), the proportion of GG, GA and AA genotypes was 70.96; 19.35 and 9.67%, respectively, whereas in children aged 14-18 years (senior school age - n=7), the percentage of genotypes was 57.14; 28.57 and 14.28%, respectively.In addition, in the main group of patients, hemostasis and platelet activity were evaluated, classified according to the genotypes of polymorphism 197G>A of the IL17A gene (GG, GA and AA). According to the analysis, individuals with the GG genotype had a significantly higher platelet count by 2.39 times (p<0.05), an increase in the PTI index by 19.0% (p<0.05), an increase in fibrinogen levels by 18.3% (p<0.05), a decrease in the GAT index by 20.7% (p<0.05) and a decrease in the percentage of megakaryocytes increased by 22.83% (p<0.05) compared with individuals with the homozygous AA genotype. On the other hand, when comparing the presented results with the indicators of KKV, TRKG, FA and RCS for different genotypes of polymorphisms of the IL17A 197G>A gene, a statistically significant difference in the above parameters was found (p>0.05). In addition, during the study, we analyzed the levels of immunoglobulins in the main group, stratifying it by polymorphism 197G>A of the IL17A gene genotypes (GG, GA and AA). The results showed that with the 197G>A polymorphism of the IL17A gene, the IgG level in individuals with the AA genotype was statistically significantly 1.39 times higher than in individuals with the GG genotype. However, there were no statistically significant differences (p>0.05) in IgA and IgM levels among the 197G>A polymorphism genotypes of the IL17A gene.As a result of the study, it was found that the rs2275913 polymorphism of the minor A allele and the AA genotype of the IL17A gene have a statistically significant positive value in the development of ITP, especially in the acute course of ITP (the tendency of significance in chronic recurrent course of the disease and statistically insignificant patients with chronic and prolonged course of ITP) in children. As mentioned earlier, SNP rs2275913, produced by the substitution of G for the nucleotide base A in the promoter of the IL-17A gene, is significantly associated with a huge number of diseases. It has been reported that allelic variants of SNP rs2275913 bind differently to the transcription factor NFAT, which leads to differences in IL-17A secretion. The IL-17A rs22759133 polymorphism is located in close proximity to two nuclear factors activating T-cell binding motifs and contributes to the production of high levels of IL-17, which, in turn, enhances IL-17-mediated immune responses [6]. This means that the A allele has a higher affinity for binding the NFAT transcription factor, which leads to a higher expression of IL17A than usual (gain of function).Thus, carriers of the IL17A rs2275913 polymorphism A allele can cause increased IL17A production and an increase in the Th17/Treg ratio, which is important for increased inflammation and the development of ETC. Indeed, several studies have shown that IL17A, an increase in the Th17/Treg ratio, and the development of ITP are positively correlated [11,13].Similarly, it was found that the polymorphism of the IL17A rs2275913 gene of the homozygous non-wild genotype (AA) contributes to the early development of the disease, and girls have an increased risk of developing the disease. In addition, the polymorphism of the IL17A rs2275913 gene in patients with the AA genotype has statistically significant more aberrant changes in hemostasis parameters, in particular, a decrease in the number of platelets, an increase in the amount of antiplatelet globulin (GAT) and a compensatory increase in the percentage of megakaryocytes. In addition, carriers of the AA rs2275913 genotype of the IL17A gene have a higher level of total IgG compared to carriers of the homozygous wild-type genotype. These data indicate that rs2275913 polymorphism may have a higher risk of serious platelet damage in owners of the AA genotype compared to carriers of the wild type genotype. Other studies have shown that interleukin IL17A, the percentage of Th17 cells and an increased Th17/Treg ratio positively correlate with the degree of ITP disease [11].In addition, a decrease in the indicators of hemostasis of PTI and fibrinogen, due to a change in the optimal Th17/Treg ratio in the proinflammatory direction, indicates an increase in the frequency and speed of the blood clotting process [5], which leads to an increase in the use of factors associated with hemostasis, exerts additional pressure on platelets from both the qualitative and quantitative sides and it can further aggravate the course of the disease.Thus, there is a statistically significant positive relationship between the minor allele A of the rs2275913 polymorphism of the IL17A gene and the AA genotype in the development of ITP (in acute course and, probably, in chronic recurrent course of ITP) and a predisposition to a relatively early onset of the disease in carriers of the AA genotype. In addition, violations of hemostasis parameters, including platelet count, PTI and fibrinogen levels, emphasize the importance of this polymorphism in the development of ITP. Noticeable changes in the levels of total IgG and antiplatelet globulin levels among individuals with the AA genotype, along with a compensatory increase in the percentage of megakaryocytes, once again emphasize the role of the rs2275913 polymorphism of the IL17A gene in the pathogenesis of ITP in children.
References
| [1] | Clinical recommendations – Immune thrombocytopenia –2021-2022-2023 (10.11.2021) – Approved by the Ministry of Health of the Russian Federation. - M. 2023. |
| [2] | Audiya S., Mahevas M., Samson M., etc. Pathogenesis of immune thrombocytopenia. // Autoimmun Rev. - 2017. - Volume 16(6). - pp. 620-632. |
| [3] | Berry S.D.G., Dossu S., Kashif A. et al. The role of IL-17 and anti-IL-17 agents in immunopathogenesis and treatment of autoimmune and inflammatory diseases. // Int. Immunopharmacol. - 2022. - Volume 102. - p. 108402. |
| [4] | Chen K., Kolls J.K. Interlukin-17A (IL17A). // Gene. - 2017. - Volume 614. - pp. 8-14. |
| [5] | Ding J.W., Zheng H.H., Zhou T. et al. (2016). Hmgb1 modulates the Treg/Th17 ratio in patients with atherosclerosis. // Journal of atherosclerosis and thrombosis. - 2016. - Volume 23(6). - pp. 737-745. |
| [6] | Espinosa J.L. et al. The genetic variant of the IL-17 promoter is functionally associated with an acute graft-versus-host reaction after unrelated bone marrow transplantation. // PLoS One. - 2011. - Volume 6. - e26229. |
| [7] | Granger J.D., Kuehne T., Gippenmeyer J., Cooper N. Romiplostim in children with newly diagnosed or persistent primary immune thrombocytopenia. // Ann Hematol. - 2021. - Volume 100(9). - pp. 2143-2154. |
| [8] | Khavrdova E., Belova A., Goloborodko A. et al. Activity of secukinumab, an antibody to IL-17A, against brain lesions in RRMS: results of a randomized trial confirming the concept. // J Neurology. - 2016. - Volume 263. - pp. 1287-1295. |
| [9] | Ji L., Zhan Yu., Hua F., et.al. The ratio of Treg/Th17 cells correlates with the activity of primary immune thrombocytopenia. // PloS One. - 2012. - Volume 7(12). - e50909. |
| [10] | Kargar M., Torabizade M., Purrahman D. et al. Regulatory factors involved in the balance of Th17/Treg cells in immune thrombocytopenia. // Current transfer from medical. - 2023.- Volume 71(2). - p. 103389. |
| [11] | Li Yu., Wei S., Xu H. and others . Immunoregulation of Th17 in the host body against intracellular bacterial infection. // Mediat. Inflamm. - 2018. - Volume 2018. - p. 6587296. |
| [12] | Liu H.K., Lin H., Gaffen S.L. The decisive role of the nuclear factor of activated T cells in the regulation of human interleukin-17 mediated by T-cell receptors. // J Biol Chem.- 2004. - Volume 279. - pp. 52762–52771. |
| [13] | Marike H. Heinecke, Aranka V. Ballering, Agnes Jamin et al., 2017. |
| [14] | Morgan D.S., Abdel-Rauf R., Afifi A. et al., 2018. |
| [15] | Rocha A.M., Souza S., Rocha G.A. and others. Levels of IL-17A and cytokines involved in the activation of Th17 cells are elevated in patients with chronic immune thrombocytopenia. // Haematologica. - 2011. - Volume 96. - pp. 1560-1564. |
| [16] | Sarkar S., Kuni L.A., Fox D.A. The role of type 17 T helper cells in inflammatory arthritis. // Clinical experience of Immunol. - 2010. - Volume 159(3). - pp. 225–237. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML