-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(1): 21-26
doi:10.5923/j.ajmms.20251501.04
Received: Dec. 11, 2024; Accepted: Jan. 3, 2025; Published: Jan. 11, 2025

Organizational Challenges in the Rehabilitation of Children with Cerebral Palsy and Their Solutions
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLErgasheva Munisa Yakubovna
Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Ergasheva Munisa Yakubovna, Samarkand State Medical University, Samarkand, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Cerebral palsy (CP) is a chronic condition requiring a multidisciplinary approach to rehabilitation aimed at improving motor, cognitive, and social functions. This article examines modern methods of rehabilitation for children with CP, including physiotherapy, speech therapy, occupational therapy, robotic systems, and virtual reality technologies. Key organizational challenges are highlighted, such as the lack of rehabilitation centers, shortage of qualified specialists, and absence of unified patient management standards. Prospective solutions are proposed, including the development of regional centers, the integration of innovative technologies, and the enhancement of medical personnel qualifications. Special attention is given to the unique aspects of rehabilitation in Uzbekistan, where accessibility and quality of healthcare services remain pressing issues. The proposed measures aim to improve treatment outcomes and enhance the quality of life for children with CP and their families.
Keywords: Cerebral palsy, Rehabilitation, Organizational challenges, Innovative technologies, Physiotherapy, Speech therapy, Robotic systems, Uzbekistan, Review
Cite this paper: Ergasheva Munisa Yakubovna, Organizational Challenges in the Rehabilitation of Children with Cerebral Palsy and Their Solutions, American Journal of Medicine and Medical Sciences, Vol. 15 No. 1, 2025, pp. 21-26. doi: 10.5923/j.ajmms.20251501.04.
Article Outline
1. Introduction
- Cerebral palsy (CP) is a group of chronic neurological conditions caused by brain damage or underdevelopment during the perinatal period. The primary clinical manifestations include impaired motor activity, postural control, and often accompanying cognitive, speech, and sensory disorders [1]. According to the World Health Organization (WHO), the prevalence of CP is 2–3 cases per 1,000 live births, making it one of the leading causes of childhood disability [2,3]. The etiology of the disease is multifactorial, encompassing intrauterine infections, hypoxic-ischemic brain injury, prematurity, birth asphyxia, genetic mutations, and exposure to adverse environmental factors [4–6].In recent years, there has been increasing attention to the rehabilitation of children with CP, as early and comprehensive interventions can significantly improve their motor function, quality of life, and level of social integration [7]. Modern approaches to rehabilitation include physiotherapy, speech therapy, occupational therapy, the use of botulinum toxin to reduce spasticity, and the application of robotic technologies and virtual reality methods [8,9]. However, the organization of rehabilitation care faces several challenges, including a shortage of specialized facilities and the lack of unified treatment protocols [10].For Uzbekistan, the issue of rehabilitating children with CP is particularly relevant, as more than 300 new cases of the condition are registered annually, while access to rehabilitation services in remote regions remains limited [11]. Most rehabilitation centers are concentrated in Tashkent, creating significant strain on healthcare institutions and limiting access for patients from rural areas [12].The aim of this article is to analyze modern approaches to the rehabilitation of children with CP, examine key organizational challenges in Uzbekistan, Russia, and other countries, and provide an overview of promising directions for improving the quality of rehabilitation care.
2. Epidemiology and Etiology of Cerebral Palsy
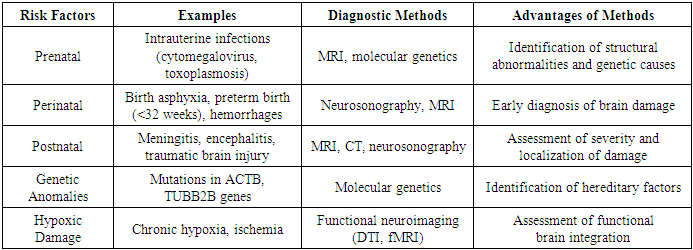
- Cerebral palsy (CP) is the most common cause of motor disability in children, occurring in 2–3 cases per 1,000 live births [1,2]. The prevalence of the condition varies depending on the development of healthcare systems, methods of perinatal diagnostics, and rehabilitation practices. In developed countries, the frequency of CP has decreased due to improved perinatal care and preventive measures. However, in resource-limited regions, the issue remains significant [3]. In Uzbekistan, over 300 new cases of CP are registered annually, with a substantial portion occurring in rural regions where access to specialized medical care is limited [4].Etiology and Risk Factors. CP is a polyetiological condition resulting from the influence of multiple factors, which can be categorized into prenatal, perinatal, and postnatal:• Prenatal factors: These include intrauterine infections (cytomegalovirus, toxoplasmosis), chronic fetal hypoxia, genetic mutations, and brain development abnormalities [5,6]. Such factors can disrupt the development of white matter and the structural integrity of the brain.• Perinatal factors: Conditions such as birth asphyxia, premature birth (especially before 32 weeks of gestation), intracranial hemorrhages, and hypoxic-ischemic encephalopathy are the leading causes of CP in preterm infants [7,8].• Postnatal factors: These encompass infectious diseases of the central nervous system (e.g., meningitis, encephalitis), traumatic brain injuries, and hypoxia occurring in the first months of life [9].Modern Approaches to Etiological Analysis. The diagnosis of CP risk factors relies on advanced technologies that can identify not only structural brain abnormalities but also genetic causes of the condition:1. Magnetic Resonance Imaging (MRI): This technique visualizes white matter damage, hemorrhages, and signs of hypoxic-ischemic encephalopathy. It is considered the gold standard for diagnosing CP in suspected cases [10].2. Neurosonography: Effective for early diagnosis in newborns, particularly preterm infants, for detecting hemorrhages, ventriculomegaly, and hypoxic changes [11].3. Molecular Genetics: Used to identify rare genetic mutations associated with brain development disorders, such as mutations in the ACTB or TUBB2B genes [12].4. Functional Neuroimaging Methods: Techniques such as diffusion tensor imaging (DTI) and functional MRI (fMRI) are applied to assess the condition of white matter and its impact on motor functions [13].Regional Features in Uzbekistan. In Uzbekistan, the rate of preterm births, a major risk factor for CP, reaches 12–15% of the total number of live births [14]. The use of modern methods such as MRI and molecular diagnostics is gradually being introduced; however, their availability remains limited in rural areas [15].
|
3. Modern Methods for the Rehabilitation of Children with Cerebral Palsy
- Rehabilitation of children with cerebral palsy (CP) requires a comprehensive approach that includes physical therapy, speech correction, occupational therapy, medication, and the use of modern technologies. The goal of rehabilitation is not only to improve motor skills but also to enhance the child’s independence and quality of life [5,7].1. Physical Therapy. Physical therapy forms the foundation of CP rehabilitation. Key methods include:• Bobath Method: Used to improve motor control and normalize muscle tone [13].• Vojta Concept: Focuses on stimulating reflexive movements and developing motor patterns [14].• Therapeutic Exercises: Applied to strengthen muscles, improve coordination, and maintain balance [15].Physical therapy helps reduce spasticity and improves motor functions, especially in children with mild to moderate CP.2. Speech Therapy. Correction of speech disorders is an essential aspect of rehabilitation. Speech therapy sessions include:• Articulation Exercises: To improve the function of the speech apparatus [16].• Bioacoustic Stimulation: To activate brain speech centers [6].Speech therapy enhances communication skills and promotes social adaptation in children.3. Occupational Therapy. Occupational therapy focuses on developing self-care skills and daily independence. Programs include:• Exercises with Adapted Equipment: Tailored to meet the child’s specific needs.• Training in Basic Skills: Dressing, feeding, and using writing tools [17].Occupational therapy plays a critical role in preparing children for integration into school and social environments.4. Medication. The use of botulinum toxin type A to reduce spasticity is recognized as the gold standard for CP treatment. This method decreases muscle tone and improves functional abilities, as confirmed by studies conducted in Russia and Uzbekistan [9].5. Innovative Technologies. Modern technologies open new opportunities for rehabilitation:• Robotic Systems: Used for gait training and improving motor functions [18].• Virtual Reality: Helps stimulate brain activity and enhance motor skills [19].
4. Organizational Challenges in the Rehabilitation of Children with Cerebral Palsy
- The rehabilitation of children with cerebral palsy (CP) faces numerous organizational challenges that limit the accessibility and effectiveness of rehabilitation programs. These issues are prevalent in both developing countries, such as Uzbekistan, and resource-limited regions in developed nations [5,7].1. Lack of Specialized Facilities. A primary issue is the shortage of rehabilitation centers. In Uzbekistan, most such facilities are concentrated in major cities, such as Tashkent, making access difficult for patients from rural areas. According to the Ministry of Health of the Republic of Uzbekistan, approximately 60% of children with CP do not receive regular rehabilitation due to geographical remoteness [4]. A similar situation exists in Russia, where rehabilitation centers are often overburdened, and waiting times can exceed several months [10].2. Shortage of Qualified Specialists. Many countries, including Uzbekistan, face an acute shortage of specialists such as physiotherapists, speech therapists, occupational therapists, and neurologists trained to work with children with CP [16]. Medical training programs often fail to cover modern rehabilitation techniques, leading to reduced quality of care [6].3. Insufficient Funding. Rehabilitation for children with CP requires significant financial resources. Government programs often cover only part of the expenses, placing a substantial financial burden on the families of patients. In Uzbekistan, rehabilitation costs account for about 30% of a family’s budget, making services inaccessible for low-income families [11]. In Europe and North America, state insurance systems have been implemented to partially address this issue [12].4. Absence of Unified Standards. In most cases, standardized protocols for managing CP patients are lacking, leading to variability in approaches and reduced treatment effectiveness. Neither Russia nor Uzbekistan has established unified recommendations to ensure continuity and systematic rehabilitation [8].5. Role of the Family. Another critical issue is the insufficient involvement of families in the rehabilitation process. Parents often lack the necessary knowledge to support their children at home, and educational programs for families cover only a small percentage of patients [17]. Studies indicate that active family participation in the rehabilitation process improves treatment outcomes and promotes the social adaptation of children [9].Solutions. To address the identified challenges, the following measures are necessary:• Establishment of Regional Rehabilitation Centers: This will improve access to services for rural residents.• Training Specialists: Organizing advanced training courses on modern rehabilitation methods.• Financial Support: Developing government programs aimed at reducing costs for families.• Implementation of Standards: Creating unified protocols for managing children with CP.• Family Involvement: Conducting educational activities and providing psychological support to parents.
5. The Role of the Family in the Rehabilitation of Children with Cerebral Palsy
- Family involvement is a key component of the successful rehabilitation of children with cerebral palsy (CP). The family plays a central role in ensuring continuity of care, providing psychological support for the child, and implementing rehabilitation activities at home [5,7]. Studies show that active family participation in the treatment process improves functional and social outcomes in children with CP [6].1. Family Involvement in the Rehabilitation Process. One of the most critical tasks is teaching parents and relatives how to provide care and perform simple rehabilitation exercises at home. In countries with advanced rehabilitation systems, special educational programs for parents are available. For instance, in Sweden and Norway, such programs include regular training sessions, consultations, and psychological support [12,20]. In Uzbekistan, similar programs are under development but remain limited in scope [4].2. Psychological Support for Parents. Parents of children with CP often face high levels of stress, depression, and emotional burnout [21]. Organizing support groups, consultations with psychologists, and psychotherapy sessions help reduce stress and improve the overall quality of family life [22]. In Russia, specialized centers for psychological support of families have been established, but in Uzbekistan, such services are currently available only in major cities [10].3. Financial Aspects. Families of children with CP often encounter financial difficulties due to the high cost of rehabilitation. Government programs in countries like Germany and Canada provide subsidies for rehabilitation services [23]. In Uzbekistan and other Central Asian countries, additional measures are needed to reduce the financial burden on families, including free provision of essential rehabilitation tools [24].4. The Role of the Family in the Child’s Social Adaptation. The social adaptation of children with CP largely depends on their environment. Active parental involvement promotes successful integration into school and society. Research shows that children whose parents actively participate in their education and socialization demonstrate better cognitive and emotional development outcomes [25,26].Solutions. To enhance family involvement in the rehabilitation process, the following measures are recommended:• Development of Accessible Educational Programs for Parents: Including online courses and video materials.• Organization of Systematic Psychological Support for Families: Providing regular counseling and mental health support.• Government Support: Offering benefits and subsidies for rehabilitation services.• Promotion of Social Initiatives: Aimed at integrating children with CP into educational and cultural institutions.
6. Innovative Approaches and Prospects in the Rehabilitation of Children with Cerebral Palsy
- Recent advances in medical technologies have opened new opportunities for the rehabilitation of children with cerebral palsy (CP). Innovative approaches include the use of robotic systems, virtual and augmented reality technologies, bioengineering solutions, and other methods designed to improve the functional capabilities and quality of life of patients [5,7].Robotic Systems. Robotic technologies are actively used for rehabilitating children with motor impairments. The most common systems include:• Exoskeletons: Provide support during walking, stimulating correct movement patterns [18].• Robotic Trainers (Lokomat and Gait Trainer): Help restore walking, improve movement coordination, and strengthen muscles [27]. Studies show that using robotic devices in combination with traditional physical therapy yields more pronounced results in children with moderate and severe CP [25].Virtual and Augmented Reality. Virtual reality (VR) technologies create an interactive environment for performing rehabilitation exercises. Benefits of VR include:• Motivating Children Through Gamified Elements.• Improving Cognitive and Motor Functions [28]. Augmented reality (AR) is used to train real-time movements, making rehabilitation more effective [29].Biofeedback. The biofeedback method allows patients to visualize their physiological processes (e.g., muscle tension) and improve control over them. This method has proven effective in reducing spasticity and enhancing motor control in children with CP [30].Bioengineering and Genetic Technologies. Innovative bioengineering developments, such as 3D printing of orthopedic devices, enable the creation of individualized tools for correcting motor impairments [23]. Genetic research offers prospects for diagnosing and correcting hereditary factors influencing CP development [19].Electrical Stimulation. Functional electrical stimulation is used to activate muscles and improve their strength. This method is applied to rehabilitate both upper and lower limbs, as well as to correct posture [16].Personalized Approach. Modern rehabilitation programs are designed to meet the individual needs of each patient. The use of big data and artificial intelligence (AI) algorithms enables the prediction of therapy effectiveness and the adaptation of treatment methods to each child [6].Prospects for Implementing Innovative Technologies in Uzbekistan. In Uzbekistan, the implementation of innovative methods is constrained by insufficient material and technical resources as well as a shortage of qualified personnel. To address this issue, the following measures are necessary:• Enhancing Specialist Training: Improving qualifications in robotic and technological rehabilitation.• Investing in Specialized Centers: Establishing facilities equipped with innovative technologies.• International Collaboration: Partnering with leading rehabilitation centers to exchange experiences and adopt best practices.
7. Conclusions
- Cerebral palsy (CP) remains one of the leading causes of motor disability in children, requiring a comprehensive and multidisciplinary approach to rehabilitation. The analysis shows that despite significant advances in diagnostics and treatment, serious organizational challenges persist, limiting the accessibility and effectiveness of rehabilitation services.Innovative approaches, such as robotic systems, virtual and augmented reality technologies, biofeedback, and personalized rehabilitation strategies, open new opportunities to improve rehabilitation outcomes. However, their implementation requires substantial investments in infrastructure, specialist training, and the creation of technological support systems.For Uzbekistan, the key priorities include:1. Developing a network of regional rehabilitation centers accessible to rural residents.2. Introducing national rehabilitation standards that incorporate international best practices.3. Training specialists in modern rehabilitation methods and technologies.4. Developing educational programs for parents to increase their involvement in the treatment process.5. Increasing funding for rehabilitation programs, including support for low-income families.Implementing these measures will significantly improve the quality of rehabilitation services, enhance treatment outcomes, and improve the quality of life for children with CP and their families. Collaboration among specialists, the government, and society is essential to address this critical social and medical issue effectively.