-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(12): 3437-3441
doi:10.5923/j.ajmms.20241412.77
Received: Dec. 10, 2024; Accepted: Dec. 28, 2024; Published: Dec. 31, 2024

Alternative Phytotherapy for Dyspeptic Symptoms After Eradication Therapy Using the Ventrap® Biologically Active Food Supplement
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMakhmudova N. M.
Republican Scientific and Practical Center for Traditional Medicine, 2 Farobi St., Almazar District, Tashkent, Uzbekistan
Correspondence to: Makhmudova N. M., Republican Scientific and Practical Center for Traditional Medicine, 2 Farobi St., Almazar District, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article discusses the results of using the biologically active supplement VENTRAP®, consisting of dried mulberry, black root, and large plantain, in addition to eradication therapy (ET) in 40 hospitalized patients suffering from Helicobacter pylori-associated chronic gastritis. Despite the implementation of highly effective eradication therapy (ET), 15-25% of patients continue to experience persistent dyspeptic symptoms (DS) such as a burning sensation and pain in the epigastric region, heaviness after meals, and early satiety, significantly worsening the patients' quality of life. VENTRAP has demonstrated high effectiveness and safety in eliminating (DS) and has been recommended as an alternative phytotherapy for the treatment and prevention of (DS) in patients with Helicobacter pylori-associated chronic gastritis.
Keywords: Phytotherapy, Alternative medicine, Helicobacter pylori, Chronic gastritis, Gastroenterology, Dietary supplements, Dandelion, Elecampane, Great plantain
Cite this paper: Makhmudova N. M., Alternative Phytotherapy for Dyspeptic Symptoms After Eradication Therapy Using the Ventrap® Biologically Active Food Supplement, American Journal of Medicine and Medical Sciences, Vol. 14 No. 12, 2024, pp. 3437-3441. doi: 10.5923/j.ajmms.20241412.77.
1. Introduction
- Among stomach diseases, gastritis, functional dyspepsia, peptic ulcer disease, and stomach cancer are most frequently discussed. The history of studying stomach diseases dates back centuries in the development of medicine and healthcare; however, to this day, problems related to the pathologies of the upper gastrointestinal tract remain relevant. The complexity of solving this problem for medicine and healthcare is determined by the widespread prevalence of these diseases, the multifactorial nature of their causes, the polymorphism of symptoms, and the difficulty of diagnosis and statistical accounting [1,2,3].Helicobacter pylori (H. pylori) is one of the most common bacterial infections worldwide, affecting nearly half of the global population. In fact, it is often stated that every second person on Earth is a carrier of H. pylori. This high prevalence makes it a significant public health concern, particularly due to its association with gastrointestinal diseases such as gastritis, peptic ulcers, and even gastric cancer. In African countries, approximately 80% of the population is infected, in South America about 70%, in Asia about 55%, and in Europe 47%. [3,4] In Central Asian countries, the prevalence of H. pylori exceeds 70%. In Uzbekistan, according to M.M. Karimov et al. (2018), the prevalence of H. pylori reaches 80-84%, with a mixed type of IceA1/IceA2 infection with the CagA genotype. In patients with chronic atrophic gastritis (B-type), the most frequently detected strain is Cag+ VacA s1 VacA m2 and IceA [5]. Cag+ VacA and VacA m2 and IceA [5] strains were most frequently detected in patients with chronic hepatitis C (B-type).It should be noted that H. pylori infection is mainly acquired in childhood and persists throughout life without special treatment, which ensures its transmission route - domestic, fecal-oral - through water and food products, kissing, etc. [6,7,8]. One of the risk factors for the development of chronic gastritis is advanced age, especially over 60 years old [9]. Both older and contemporary authors studying the development and prevalence of gastritis, functional dyspepsia (FD), and gastric cancer pay considerable attention to the dietary risk factor. According to the Chinese author Yuan Li (2020), a survey of patients with gastritis showed that the majority of them (58.2%) attribute their illness to dietary and behavioral factors. According to the author, the factors of dyspeptic disorders in all men were irregular meal portion sizes, barbecue, snacks, and alcohol, while sweets were the only dietary factor associated with all symptoms in women [10,11].20-30% of the population constantly or periodically experiences dyspeptic symptoms. However, research has shown that a smaller portion (35-40%) belongs to the group of diseases classified as organic dyspepsia, while a larger portion (60-65%) is attributed to functional dyspepsia (FD). The etiology and pathogenesis of FD syndrome remain insufficiently studied. The role of H. pylori infection in causing functional dyspepsia (FD) is still debated among experts. Some believe it plays a part, while others argue that it's not a significant factor. Current data does not provide grounds for considering H. pylori as a significant etiological factor in the development of dyspeptic disorders in most patients with functional dyspepsia. Eradication may only be beneficial for 5% of such patients. Treatment of H. pylori-associated gastritis is a complex and lengthy process, requiring significant economic, labor, and time costs not only from medical staff but also from the patient and their family. Ideally, etiotropic therapy (ET) should lead to 90% eradication of H. pylori, which is achieved by the simultaneous use of 2-3 antibiotics. However, doctors in many countries are observing a decrease in the effectiveness of ET to an unacceptable level of ≤ 80%. The main reasons for unsuccessful eradication are the emergence of antibiotic-resistant H. pylori strains [12,13].Research Objective: To study the clinical efficacy and tolerability of the dietary supplement VENTRAP® manufactured by "OMAR CARE" (Uzbekistan).
2. Materials and Methods
- The study included 40 patients aged 19 to 60, with an average age of 35+16.5 years, with a verified diagnosis of HP associated with CG. The diagnosis was established based on EFGDS and targeted biopsy followed by a rapid urease test on the NR. Chronic gastritis, verified in the patient, and the clinical symptom complex characteristic of FD, were combined when making a general diagnosis and encrypted in the ICB-10 using both the "chronic gastritis" (K 29) and "fever functional disorders" (K 31). All patients completed a special questionnaire designed to assess the likelihood of acid-related diseases, including functional dyspepsia (FD). According to the questionnaire, epigastric pain syndrome was noted in cases where the patient reported moderate or severe pain or a burning sensation in the upper abdominal area at least once a week. At the same time, the pains were not permanent, they were related to eating or arose at night, did not localize in other parts of the abdomen, did not decrease after defecation and did not accompany signs of dysfunction of the gallbladder or Oddy's sphincter. Epigastric pain syndrome is often accompanied by postprandial distress syndrome. Postprandial distress syndrome was noted when patients experienced a sense of heaviness in the upper abdomen or felt full too quickly after eating, at least several times a week. Additionally, postprandial distress syndrome was sometimes associated with nausea and epigastric pain. Symptoms were assessed using a three-point system, where: 0 - absence of symptoms; 1 - poorly expressed, periodic symptoms - rarely; 2 - moderately expressed symptoms - quite often; 3 - pronounced, permanent symptoms - constant.Patients were divided into 2 groups, comparable in terms of gender, age, and clinical course of CG and FD. The first control group of patients received standard eradication therapy consisting of a proton pump inhibitor (PPI), amoxicillin at a dose of 1.0 g 2 times a day, clarithromycin at a dose of 500 mg 2 times a day, and tricalcium bismuth citrate at a dose of 120 mg 4 times a day for 10 days. Another group of patients (the main group) on the background of similar eradication therapy for 4 weeks also received the dietary supplement VENTRAP® 370 mg 1 tablet 3 times a day. Control tests for NR infection were conducted 4 weeks after the completion of eradication therapy using the C14 respiratory urea test. The anti-secretory efficacy of the drugs was assessed by topographic pH-metry using glass-surface probes and their registration on the "AGM-03" microprocessor acidogastrometer.
3. Results and Discussion
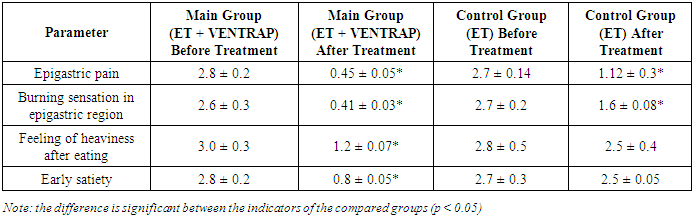
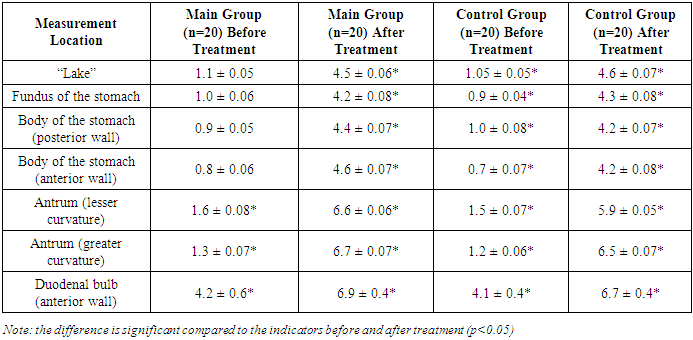
- The study included patients with chronic hepatitis who were hospitalized, both sexes, aged 18 and older, who agreed to participate in the study. Exclusion criteria for the study were pregnancy, lactation, calculous cholecystitis and/or mechanical obstruction of the biliary tract, increased sensitivity to the components of the drug, the patient's participation in other clinical trials in the last 30 days, and intestinal obstruction.The studied plant pest VENTRAP® consists of the following medicinal herbs: Plantago major (40%), Taraxacum officinale (30%), Inula helenium (30%). Plantago major (Large and ordinary traveller). Folium plantaginis majoris (Latin) and herba plantaginis majoris (Herba Plantaginis majoris recens) are used as medicinal raw materials. Taraxacum officinale (medicinal common bile duct) exhibits biliary, fever-reducing, laxative, relieving, calming, spasmolytic, and mild sleep-inducing effects. Inula helenium is used as an exfoliating agent and in the treatment of gastrointestinal diseases. The clinical presentation of chronic gastritis (CG) and peptic disorders (PD) in patients was characterized by ulcerative syndrome in 24.3% of cases and postprandial distress syndrome in 20.6%. A mixed form of the disease occurred in 45.3% of patients. Pain in the upper abdomen was reported in only 36.5% of cases, with 62% of those patients experiencing pain after eating. Nighttime pain affected 82% of patients, and in 89% of these cases, the pain was severe enough to disrupt sleep.Additional symptoms included early satiation, noted by 85.7% of patients, burning sensations mainly in the epigastric region (85.4%), and nausea, which was reported in 92.5% of cases.The most significant causes of functional dyspepsia (FD) in these patients were:- Acid-related factors- Genetic predisposition- A history of non-responders (NR)- Smoking and alcohol use- Frequent toxic infections- Dietary factors such as excessive spicy or salty food, late-night meals, and overeating- Psychosocial factorsNutritional recommendations for all FD patients included frequent (5-6 times a day), small, and fractional meals, with restrictions on fatty and spicy foods, as well as coffee. It was recommended to refrain from smoking, alcohol consumption, and NSAIDs.Studies to evaluate the effectiveness of the eradication treatment regimen were conducted 8 weeks after the start of treatment. According to the protocols of the VI Maastricht Consensus, 85% of the eradication rate is "satisfactory." Thus, according to our research, the eradication rate indicators of the main group of patients who received vonprazole meet the criteria of "satisfactory."Table 1 presents the dynamics of clinical manifestations of the disease before and after the course of treatment.
|
|
|
4. Conclusions
- After these experiments, we have come to certain conclusions regarding the use of the dietary supplement VENTRAP® in conjunction with eradication therapy for patients with H. pylori-associated chronic gastritis (CG) and functional dyspepsia (FD). The findings are as follows:1. The use of the dietary supplement VENTRAP®, which contains Plantago major, Taraxacum officinale, and Inula helenium, in combination with eradication therapy in patients with H. pylori-associated CG and FD, significantly contributes to the alleviation of clinical symptoms of these conditions.2. The clinical benefits of VENTRAP® are demonstrated by the reduction in both abdominal pain and postprandial distress syndrome symptoms in patients with FD.3. VENTRAP® was well tolerated by all patients when used alongside standard treatments for CG and FD, with no reported side effects observed during the study.