Yodgarova U. G., Raimova M. M.
Tashkent State Dental Institute, Tashkent, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The study included 21 patients with symptomatic restless legs syndrome (RLS) combined with chronic kidney failure. The severity of the disease symptoms in all patients was assessed using the Augmentation Severity Rating Scale (ASRS) and Johns Hopkins Restless Legs Severity Scale (JHRLSS). To evaluate the effectiveness of the scales for assessing symptom severity in RLS, the highly effective International Restless Legs Syndrome Rating Scale (IRLS) was used. In cases of symptomatic RLS associated with chronic kidney failure, the IRLS scale demonstrated high effectiveness: mild symptoms were recorded in 10 (90.9%) cases using both the IRLS and ASRS, whereas the JHRLS scale identified mild symptoms in 6 (54.5%) cases, which is 1.67 times lower. Severe symptoms were identified in 1 (10.0%) case using both the IRLS and JHRLS scales, but no severe symptoms were detected using the ASRS, indicating its low effectiveness in assessing severe symptoms. To assess the reliability of the scales used, Receiver Operating Characteristic (ROC) analysis was applied, combining the sensitivity and specificity of the scales using the Area Under the Curve (AUC).
Keywords:
Symptomatic restless legs syndrome, Augmentation Severity Rating Scale (ASRS), International Restless Legs Syndrome Rating Scale, Johns Hopkins Restless Legs Severity Scale, Receiver Operating Characteristic, Area Under the Curve
Cite this paper: Yodgarova U. G., Raimova M. M., Determination of the Effectiveness of Assessing the Severity of Symptoms in Patients with Restless Legs Syndrome Combined with Chronic Kidney Failure Using Scales, American Journal of Medicine and Medical Sciences, Vol. 14 No. 12, 2024, pp. 3420-3424. doi: 10.5923/j.ajmms.20241412.73.
1. Relevance
The prevalence of chronic kidney failure (CKD) is estimated at 10–15% of the general population, meaning that over 800 million people worldwide are living with CKD [1,7]. Among patients undergoing hemodialysis, CKD is highly prevalent, with approximately 70–90% of these patients experiencing various neurological symptoms, including restless legs syndrome (RLS) [2,4]. RLS affects 5–10% of the general population, with its prevalence reaching up to 15% in older adults [2,3,5]. RLS is more common in women (60%) and presents a higher risk in older age groups. Approximately 20–50% of CKD patients exhibit symptoms of RLS [1,8,9]. The prevalence of RLS among patients undergoing hemodialysis is 20–30%, with severe symptoms observed in approximately 10–15% of these patients [4,10].Purpose of the study. The study aimed to assess the severity of symptoms in patients with symptomatic restless legs syndrome (RLS) combined with chronic kidney failure using the International Restless Legs Syndrome Rating Scale (IRLS), Augmentation Severity Rating Scale (ASRS), and Johns Hopkins Restless Legs Severity Scale (JHRLSS).
2. Materials and Methods
The study included 21 patients diagnosed with symptomatic restless legs syndrome (RLS), of whom 13 were women and 8 were men, with an average age of 49.5±3.9 years. Patients belonged to different age groups, and the study considered the duration of their illness, the severity of their symptoms, and their response to treatment.All patients underwent either standard treatment (n=10) or comprehensive treatment (n=11). Their condition was evaluated both before and after treatment using several validated scales, including the Augmentation Severity Rating Scale (ASRS), International Restless Legs Syndrome Rating Scale (IRLS), and Johns Hopkins Restless Legs Severity Scale (JHRLSS). Each scale provided an in-depth analysis of various aspects of the disease and its impact on patients' lives.The patients’ conditions were assessed using primary symptoms affecting both physical and psychological states and quality-of-life indicators measured through the scales. Based on the scale results, data on changes during treatment and symptom progression or regression were collected. This analysis facilitated the development of effective treatment strategies tailored to the severity of symptoms.
3. Results Аnalysis
The effectiveness of the IRLS scale in detecting symptom severity in RLS was found to be nearly 100%, making it the gold standard for evaluating the efficacy of other scales and questionnaires used in the study. The IRLS scale is internationally recognized for diagnosing RLS and assesses the severity of symptoms, their impact on daily activities, and the general condition of patients. The JHRLSS, developed by Johns Hopkins University, is used to evaluate the severity of RLS symptoms. The Augmentation Severity Rating Scale (ASRS) is a specialized scale used to assess symptom exacerbation or progression associated with RLS.These scales collectively enabled a comprehensive evaluation of symptom severity in patients with RLS and CKD, aiding in the identification of effective treatment strategies.The results of assessment of disease severity using scales in patients with chronic renal failure (SBE) in the study group are presented in Figure 1. 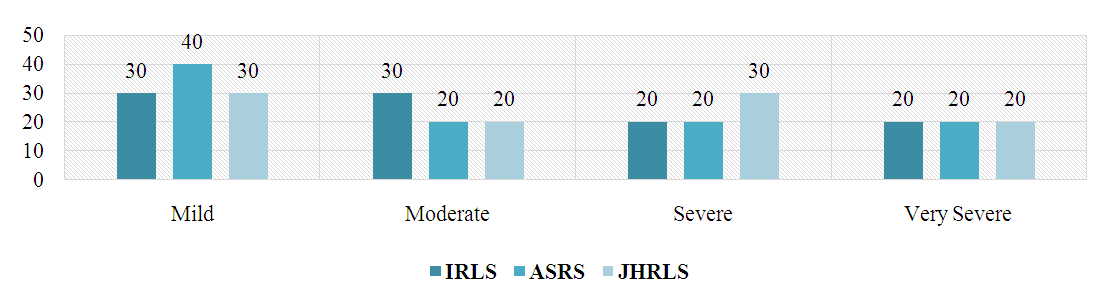 | Figure 1. In patients with chronic kidney failure (n=10) scores of symptom severity scores before standard treatment, % |
Mild pretreatment symptoms were observed in 3 (30.0%) patients on the IRLS scale, 4 (40.0%) patients on the ASRS scale, and 3 (30.0%) patients on the JHRLS scale. Here, the number of mild symptoms according to ASRS was 1.33 times higher compared to IRLS and JHRLS.Moderate symptoms were reported in 3 (30.0%) patients on the IRLS, 2 (20.0%) patients on the ASRS, and 2 (20.0%) patients on the JHRLS, showing a difference between ASRS and JHRLS scores. shows the same level and it was found that the number of moderately severe symptoms is 1.5 times less compared to IRLS.Severe symptoms were reported in 2 (20.0%) patients in IRLS and ASRS, and in 3 (30.0%) patients in JHRLS. This indicates a 1.5 times greater number of severe symptoms on the JHRLS scale. Symptoms of extreme severity were the same for IRLS, ASRS and JHRLS, i.e. 2 (20.0%) patients, where no difference was noted.The results of symptom severity scales after standard treatment are presented in Figure 2. Mild symptoms were observed in 5 (50.0%) patients on IRLS, 7 (70.0%) on ASRS and 6 (60.0%) on JHRLS. Mild symptoms on the ASRS scale were reported more often and were 1.4 times higher compared to IRLS and 1.17 times higher compared to JHRLS.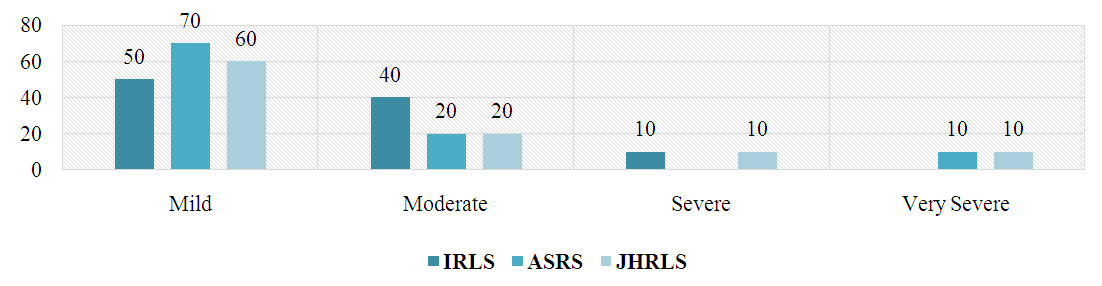 | Figure 2. In patients with chronic kidney failure (n=10) scores of symptom severity after treatment, % |
Symptoms of moderate severity were noted in 4 (40.0%) patients on IRLS and 2 (20.0%) patients on ASRS and JHRLS. This showed 2 times more moderate-severe symptoms on the IRLS scale, indicating that this scale better identifies moderate-severe symptoms associated with BOS.Severe symptoms were reported in 1 (10.0%) patients on the IRLS and JHRLS, while no severe symptoms were reported on the ASRS. This suggests that the ASRS scale is not effective in assessing severe symptoms.Severe symptoms were reported in 1 patient (10.0%) in ASRS and JHRLS, but not in IRLS. This suggests that the ASRS and JHRLS scales are limited in their ability to detect severe symptoms.Based on the analysis, it was found that the ASRS was effective in recording mild symptoms and the JHRLS was effective in recording severe and very severe symptoms.The results of the evaluation of the severity of symptoms by IRLS, ASRS and JHRLS scales (n=10) 3 months after treatment are presented in Figure 3.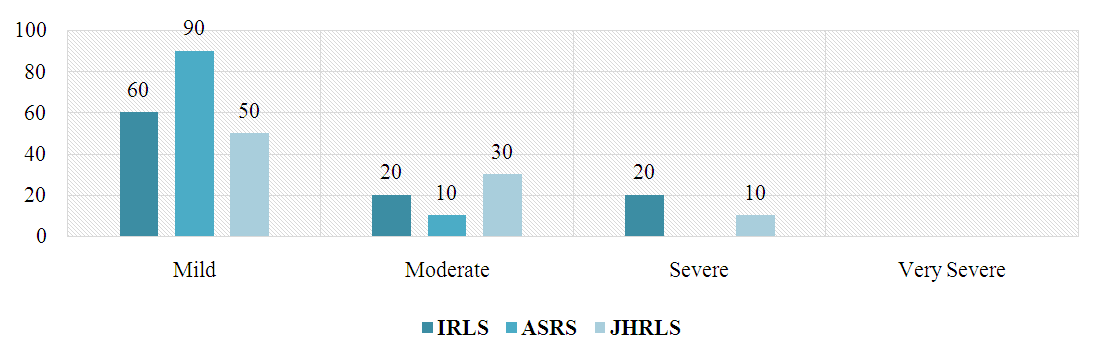 | Figure 3. Results of assessment of severity of symptoms with chronic renal failure (n=10) after 3 months of treatment, % |
Mild symptoms were observed in 5 (50.0%) patients on IRLS, 7 (70.0%) on ASRS and 6 (60.0%) on JHRLS. It was found that mild symptoms on the ASRS scale were reported more often and were 1.4 times higher compared to IRLS and 1.17 times higher compared to JHRLS.Symptoms of moderate severity were noted in 4 (40.0%) patients on IRLS and 2 (20.0%) patients on ASRS and JHRLS. This shows that 2 times more moderate-severe symptoms were reported on the IRLS scale, indicating that this scale better identifies moderate symptoms.Severe symptoms were reported in 1 (10.0%) patients on the IRLS and JHRLS, while no severe symptoms were reported on the ASRS. This suggests that the ASRS scale is not reliable in assessing severe symptoms.The results of the assessment of severity levels of disease symptoms before complex treatment are presented in Figure 4. In patients with restless legs syndrome accompanied by SBE, mild and severe symptoms were recorded on the ASRS scale and the IRLS scale (27.2% and 18.1%, respectively) before complex treatment.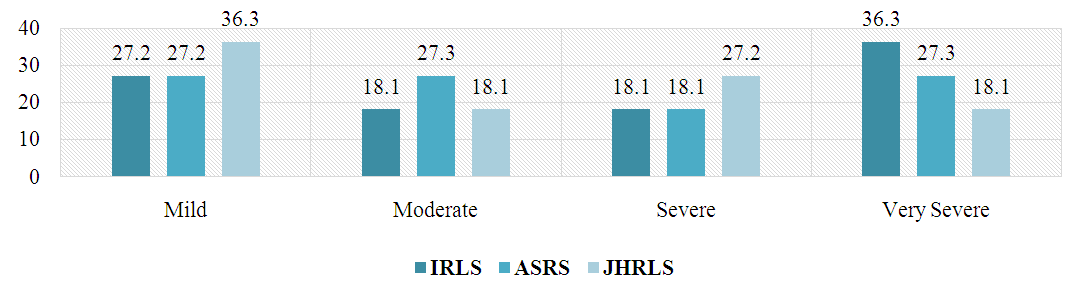 | Figure 4. Results of assessment of disease severity after complex treatment in patients with chronic kidney failure (n=11), % |
High efficiency (100.0%) was found in the JHRLS scale for identifying moderate symptoms. ASRS (27.3%) was more accurate than JHRLS (18.1%) in determining the severity of BOS.In patients with chronic kidney failure of the second group (n=11) the results of disease severity assessment after complex treatment are presented in Figure 5.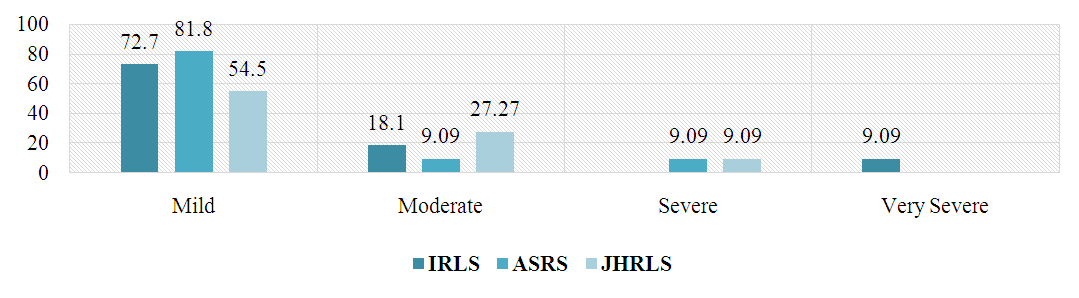 | Figure 5. Results of assessment of disease severity after complex treatment in patients with chronic kidney failure (n=11), % |
In identifying mild symptoms, ASRS had 9.1% error, JHRLS 18.2%, and ASRS had a relatively better result (81.8%). Both the ASRS and JHRLS scales had an error of 9.1% in determining the moderate level of BOS. This shows that they are an effective method for determining the average severity of the disease. Based on the IRLS scale, erroneous results were obtained on the ASRS and JHRLS scales when determining severe and severe symptoms.Рatients with chronic kidney failure (n=11), 3 months after complex treatment, the results of evaluating the severity of symptoms using IRLS, ASRS and JHRLS scales were analyzed (Fig. 6).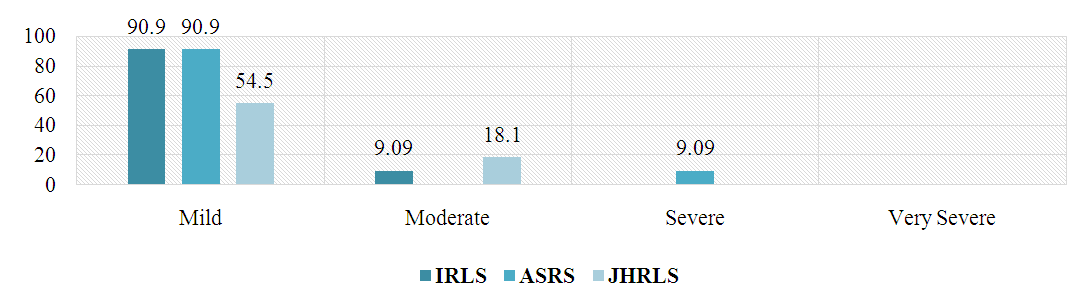 | Figure 6. Results of assessment of severity of disease in patients with chronic kidney failure (n=11) after 3 month complex treatments, % |
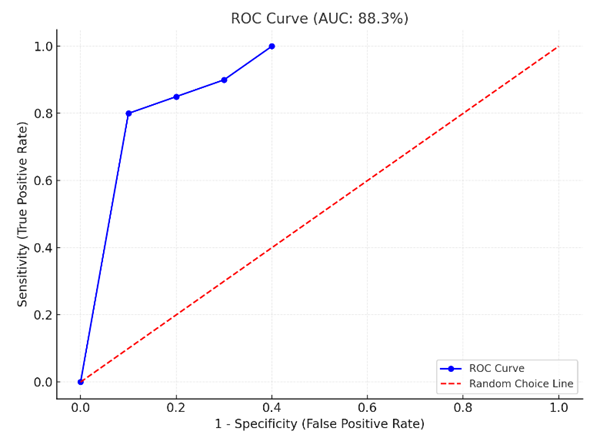
Mild symptoms were noted in 10 (90.9%) patients according to the IRLS and ASRS scales, while this indicator was 6 (54.5%) patients according to the JHRLS. It was found that the scores on the IRLS and ASRS scales were the same and 1.67 times higher compared to the JHRLS. This suggests that the IRLS and ASRS are equally effective in identifying mild symptoms, but the JHRLS was found to under-detect symptoms at this level.Moderate-severe symptoms were reported in 1 (9.09%) patient on IRLS, no symptoms at this level on ASRS, and 2 (18.1%) patients on JHRLS. Compared with IRLS, JHRLS was recorded in 2 times more patients. This analysis suggests that the ASRS scale is effective in identifying mild symptoms.Severe symptoms were noted in 1 patient (9.09%) according to the ASRS, and symptoms of this level were not detected in the IRLS and JHRLS scales.The reliability assessment results of the IRLS scale using the ROC curve in patients with symptomatic restless legs syndrome (RLS) combined with diabetes mellitus are presented in Figures 7–8.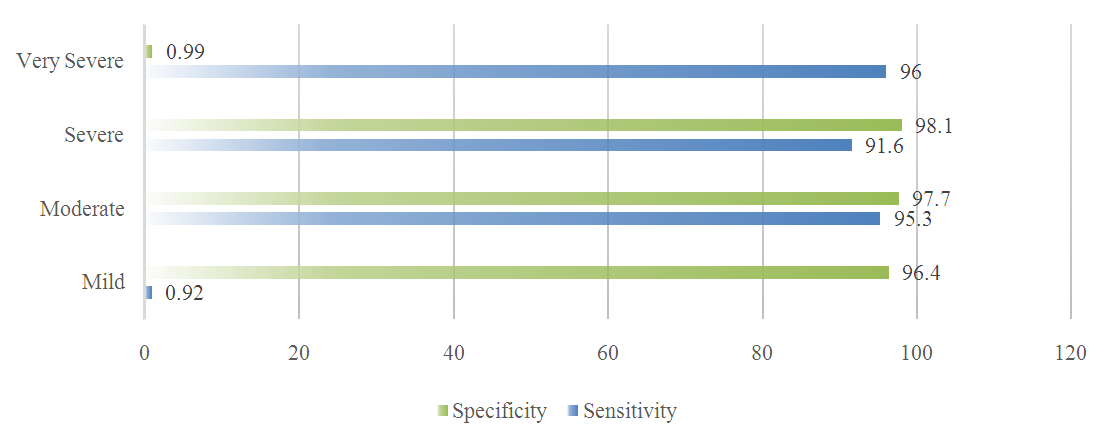 | Figure 7. Reliability assessment results of the IRLS scale using the ROC curve, % |
 | Figure 8. Graphical representation of the effectiveness of the JHRLSS scale in the study group |
For mild symptoms, the sensitivity was recorded at 92%, and specificity at 96.4%, indicating the IRLS scale's very high reliability in detecting mild symptoms. These high sensitivity and specificity values confirm the scale's strong performance in symptom identification.For moderate symptoms, the sensitivity was determined to be 95.3%, and specificity 97.7%. These values emphasize the IRLS scale's ability to provide reliable and precise results when assessing this level of symptom severity.For severe symptoms, the sensitivity was 91.6% and the specificity was 98.1%, demonstrating the high reliability of the IRLS scale in detecting severe symptoms. These values highlight the scale's effectiveness in clinical applications, yielding accurate results.For very severe symptoms, the sensitivity was 96.0% and the AUC was 0.99. These indicators confirm the scale's exceptional reliability in identifying symptoms of this severity. Based on the AUC value, the IRLS scale can be effectively and reliably used to assess very severe symptoms. The AUC value was recorded at 94.6%, further validating its clinical utility.
4. Conclusions
1. In cases of symptomatic restless legs syndrome combined with chronic kidney failure, the IRLS scale demonstrated high effectiveness, with mild symptoms being identified in 10 (90.9%) patients using both the IRLS and ASRS scales. For the JHRLS scale, this indicator was observed in 6 (54.5%) patients, which is 1.67 times lower compared to the IRLS and ASRS scales. Therefore, the IRLS and ASRS scales are effective for detecting mild symptoms, whereas the JHRLS scale showed lower effectiveness in identifying symptoms of this severity.2. Moderate symptoms were recorded in 1 (9.09%) patient using the IRLS scale, while the JHRLS scale identified moderate symptoms in 2 (18.1%) patients, indicating a 2-fold increase compared to the IRLS scale. No moderate symptoms were identified using the ASRS scale, suggesting its ineffectiveness in detecting moderate symptoms. Severe symptoms were observed in 1 (9.09%) patient using the ASRS scale, while neither the IRLS nor the JHRLS scales detected severe symptoms, demonstrating the ASRS scale's advantage in identifying severe symptoms.
References
| [1] | Allen, R. P., & Earley, C. J. (2003). Restless legs syndrome: A review of clinical and pathophysiologic features. Journal of Clinical Neurophysiology, 20(1), 39–52. DOI:10.1097/00004691-200303000-00007. |
| [2] | Molnar, M. Z., & Kalantar-Zadeh, K. (2017). Association of restless legs syndrome with chronic kidney disease and mortality: A meta-analysis. Journal of the American Society of Nephrology, 28(5), 1459–1472. DOI:10.1681/ASN.2016070803. |
| [3] | Winkelman, J. W., & Claman, D. (2006). Restless legs syndrome in end-stage renal disease. American Journal of Kidney Diseases, 45(3), 565–572. DOI:10.1053/j.ajkd.2005.10.031. |
| [4] | Silber, M. H., & Ehrenberg, B. L. (2013). The relationship of restless legs syndrome with iron status and kidney function: A systematic review. Sleep Medicine Reviews, 17(6), 377–387. DOI:10.1016/j.smrv.2012.12.001. |
| [5] | Garcia-Borreguero, D., & Kohnen, R. (2017). Augmentation in restless legs syndrome: Diagnostic criteria and management. Sleep Medicine Reviews, 36, 50–58. DOI:10.1016/j.smrv.2016.11.001. |
| [6] | Kushida, C. A., & Nichols, D. A. (2006). Clinical evaluation and treatment of restless legs syndrome in chronic kidney disease. Seminars in Nephrology, 26(4), 287–294. DOI:10.1016/j.semnephrol.2006.02.006. |
| [7] | Zuo, L., & He, H. (2020). The prevalence of restless legs syndrome in dialysis patients: A systematic review and meta-analysis. BMC Nephrology, 21(1), 185. DOI:10.1186/s12882-020-01809-w. |
| [8] | Salih, A. M., & Gray, L. M. (2018). Sleep disturbances and quality of life in patients with chronic kidney disease and restless legs syndrome. Nephrology Dialysis Transplantation, 33(2), 302–310. DOI:10.1093/ndt/gfx278. |
| [9] | Ekbom, K. A. (1945). Restless legs: A clinical study. Acta Medica Scandinavica, 158, 1–123. |
| [10] | Hornyak, M., & Trenkwalder, C. (2004). Restless legs syndrome and periodic limb movement disorder in dialysis patients: An update. American Journal of Nephrology, 24(4), 431–438. DOI:10.1159/000081046. |
| [11] | Yodgarova, U., Raimova, M., & Boboyev, K. (2019). Etiopathogenetic factors and clinical picture of restless legs syndrome in persons of Uzbek nationality. Journal of the Neurological Sciences, 405, 236. |
| [12] | Raimova, M. M., & Yodgarova, U. G. (2021). PATHOGENETIC ASPECTS OF RESTLESS FEET SYNDROME. British Medical Journal, 1(1.2). |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML