-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(12): 3227-3232
doi:10.5923/j.ajmms.20241412.29
Received: Nov. 22, 2024; Accepted: Dec. 11, 2024; Published: Dec. 16, 2024

Results of Immunohistochemical Study of Colorectal Cancer in Patients Living in the Unfavorable Zone of the Aral Sea Region
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhudaykulova Feruza Xojikulovna1, Yuldashev Bakhrom Sobirjonevich2
1Senior Lecturer, Urgench branch of the Tashkent Medical Academy Uzbekistan
2DSc, Associate Professor, Vice-Rector for International Relations, Mamun University, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article provides data on patients with colon cancer living in environmentally unfavorable conditions of Khorezm region and who were treated in 2021-2023 at Khorezm branch of the Republican Scientific and Practical Oncology Center. The history of the disease, outpatient records, age categories аnd gender, pathomorphological changes and histological studies of various types of colon cancer were studied, cases of metastasis immunohistochemical study with the study of p53 and cytokeratin 20 (CK20) antigens.
Keywords: Colon cancer, Macroscopic, Microscopic changes, Pathomorphological changes, Metastasis, Histological characteristics, Immunohistochemical study, p53, Cytokeratin 20 (CK20) antigens
Cite this paper: Khudaykulova Feruza Xojikulovna, Yuldashev Bakhrom Sobirjonevich, Results of Immunohistochemical Study of Colorectal Cancer in Patients Living in the Unfavorable Zone of the Aral Sea Region, American Journal of Medicine and Medical Sciences, Vol. 14 No. 12, 2024, pp. 3227-3232. doi: 10.5923/j.ajmms.20241412.29.
1. Introduction
- The study of the state of colon cancer in the Republic of Uzbekistan by such Uzbek scientists as Navruzov S.N., Aliyeva D.A., Kulmiev E.E. (2020) showed that the incidence of colon cancer tends to increase, and the number of deaths from this pathology is also increasing, which indicates the need to study the risk factors for colon cancer, as well as continue research to identify and study territorial differences [1,4].High mortality from colon cancer and associated medical and social problems emphasize the importance of studying various aspects of the disease, including its regional characteristics. Today, colon cancer is one of the most common neoplastic diseases worldwide, and its incidence increases significantly with age, especially after 50 years [5].At the same time, a decrease in the number of deaths from this disease in relatively developed countries reflects an improvement in survival due to the introduction of advanced methods of diagnosis and treatment of cancer [2]. In the structure of all oncological neoplasms of the colon, rectal cancer ranks first, accounting for up to 95% of cancers of this localization. The term colorectal cancer includes tumors of the colon, rectal adenocarcinoma, and other types of malignant neoplasms of these organs. The reasons for the development of intestinal adenocarcinoma are not fully understood, but there is some data that allows us to determine the risk factors that increase the probability of developing this pathology: immunodeficiency states, a history of cancer of the female genital organs, the presence of polyps of the colon or rectum. In most cases, adenocarcinoma of the colon develops from existing polyps, and the longer they exist and the larger their size, the higher the risk of malignancy. Genetic predisposition: in most cases, adenocarcinoma of the colon is a sporadic disease, i.e. it is not associated with hereditary factors, but there are two cases where genetics plays a key role. This is familial adenomatous polyposis and hereditary non-polyposis colon cancer (Lynch syndrome).The presence of non-specific ulcerative colitis and Crohn's disease continuous tissue regeneration under the influence of chronic inflammation in these diseases increases the probability of mutations and cell changes, which in turn leads to the development of colon cancer [2,3].In particular, the risk increases with the nature of nutrition: with excessive consumption of animal fats, high-protein foods and a lack of fiber in the diet, as well as with overeating and alcohol abuse.If you look at it from this point of view, it is interesting to study the factors of colon cancer development among the population of Khorezm region of the ecologically unfavorable zone of the Aral Sea region, it can be revealed the dependence of the local diet on customs, age and gender of residents.
2. Materials and Methods
- The study was conducted on the basis of a retrospective analysis of the medical records of 110 patients who underwent treatment in 2021-2023, at the departments of Khorezm branch of the Oncology Scientific and Practical Center of the Republic of Uzbekistan. Their medical records, outpatient cards, age groups, gender, the most common type of colon cancer, and emerging pathomorphological changes were studied. Histological forms, the most common complications were studied, and the features of metastasis were analyzed. All patients included in the study had a confirmed histological diagnosis of colon cancer, tumor localization according to colonoscopy data, all patients underwent standard instrumental, pathomorphological and immunohistochemical research methods. Patients were examined according to the level of differentiation. Currently, the immunohistochemistry method is recognized as the gold standard for cancer diagnostics worldwide. Immunohistochemical studies are carried out to analyze various processes. This study is used to determine the molecular structure in cells, study the location of cells, study the spread or histogenesis of tumor diseases, monitor these processes during the development of precancerous processes, determine prognostic complications of diseases, determine the stages of the tumor and treatment tactics, monitor the dynamics and control the treatment processes, it is important to conduct this examination of the tumor in order to identify risk groups that can cause diseases.In order to study pathomorphologically dangerous tumors by the immunohistochemical method, patients with colon cancer were divided into 3 groups, 20 were selected from each group, a total of 60 patients and subjected to immunohistochemical examination for the level of differentiation. For immunohistochemical research, cell expression was studied using antibodies of the Bond Leica Australia immunohistoprocessor (Australia) and p53 and cytokeratin 20 (CK20) antigens were studied by immunohistochemical research.The p53 protein controls the course of cell cycle processes, as well as the presence of damage in the genome that could lead to further development of pathology. The p53-dependent apoptosis is a powerful selector that allows you to avoid the accumulation of mutations, and in the case when they have already arisen, p53-dependent apoptosis allows you to eliminate such potentially dangerous cells for the body.Tumor suppressor gene, mutations in which are found in 50% cases of cancer of all types, this gene encodes a transcription factor that controls the entry of a cell into the cell cycle. Many intracellular systems that monitor the "health" of a cell transmit signals about "malfunctions" to the p53 protein. With its help, the cell decides whether to divide or not. If the cell has irreparable damage, the p53 protein triggers a chain of events leading to "suicide" of the cell, otherwise called apoptosis [6]. Cells that do not have p53 or in which it functions incorrectly are not capable of such self-control and continue to divide, even when it becomes dangerous for the body. Like all tumor suppressors, p53 controls the normal progression of the cell cycle.Cytokeratin 20 (CK20) is a protein produced by epithelial cells in the colon and urinary tract. It is also produced by Merkle cells in the skin. This type of protein is also produced by most benign (non-cancerous) and malignant (cancerous) tumors that occur in the colon and urinary tract, as well as a type of skin cancer called Merkle cell carcinoma. Once CK20 is made, it is stored in the cytoplasm (body) of the cell. CK20 is a structural protein that helps epithelial cells maintain their shape. Immunohistochemistry (IHC) can show CK20-producing cells in a tissue sample. The results of this test, in combination with others, are needed to make a diagnosis. Cells that produce CK20 are usually described as “positive,” while cells that do not produce the protein are described as “negative.” This test is especially useful when examining a tumor under a microscope, since tumors originating from the colon and urinary tract are more likely to produce CK20, while tumors from other localizations are not. Tumors expressing cytokeratin 20: colon cancer, including adenocarcinoma; urinary tract cancer, including urothelial carcinoma;bile duct and pancreatic cancer, including cholangiocarcinoma and ductal adenocarcinoma; merkel cell carcinoma of the skin; some types of ovarian cancer, including mucinous carcinoma. Detection of the cytokeratin-20 reagent was carried out using polyclonal antibodies from Dako (Denmark) at a dilution of 1:500 according to the manufacturer's instructions. To visualize the immunohistochemical reaction, the reaction was carried out in the dark for 5-10 minutes. Evaluation of the obtained results was carried out using a light microscope. Accordingly, the localization of staining in the cell for all markers was assessed. The number of positive cells was assessed in the areas containing the maximum number of them. The tumor was considered negative if there was no nuclear reactivity with antibodies in the tumor tissue or the number of stained cells was less than 25; and if more than 25% of the tumor cell nuclei were stained, it was considered positive [7,8].
3. Results
- The results of the study showed that the incidence of tumors by age groups was 4.6% of cases in 18-34 years, 12% in 35-44 years, 20.7% in 45-54 years, the largest number of cases - 33.6% in 55-64 years, 25% in 65-74 years, 4.2% in 75-90 years; It was studied that the gender of the patients was male in 56.7% of cases, female in 43.3% of cases. Tumor localization - the most frequent localization is in the rectum - 55.3% of cases, in the sigmoid colon - in 7.8% of cases, in the rectosigmoid sinus - in 11.5% of cases, in the cecum in 4.3% of cases, the colon-hepatic angle - in 3.2% of cases, the colon-splenic angle - in 2.3% of cases, 5.5% were recorded in the ascending colon, in 3.2% of cases - in the descending colon. The study of the histological structure of the tumors showed that 30 selected patients were diagnosed with highly differentiated adenocarcinomas - G1, 45 patients - moderately differentiated adenocarcinomas - G2 and 35 patients - poorly differentiated adenocarcinomas - G3.Highly differentiated adenocarcinomas G1: The pathohistological materials of patients with colon cancer in Khorezm region were studied by the level of differentiation.Thirty of the selected patients (27%) had highly differentiated adenocarcinoma. The microscopic picture reveals hyperplasia of colon epithelial cells and malignant cancer cells with polymorphism. Angiomatous cells and fibrous connective tissue are formed in the epithelial space. Polymorphized tumor cells retained their structure and grew into all layers of the intestine.
 | Figure 1. Selected patients with well-differentiated adenocarcinoma |
 | Figure 2. Moderately differentiated adenocarcinoma G2: Moderately differentiated adenocarcinoma in patients with colon cancer in the Khorezm region |
 | Figure 3. Poorly differentiated adenocarcinoma G3: The patient had poorly differentiated adenocarcinoma |
|

|

4. Conclusions
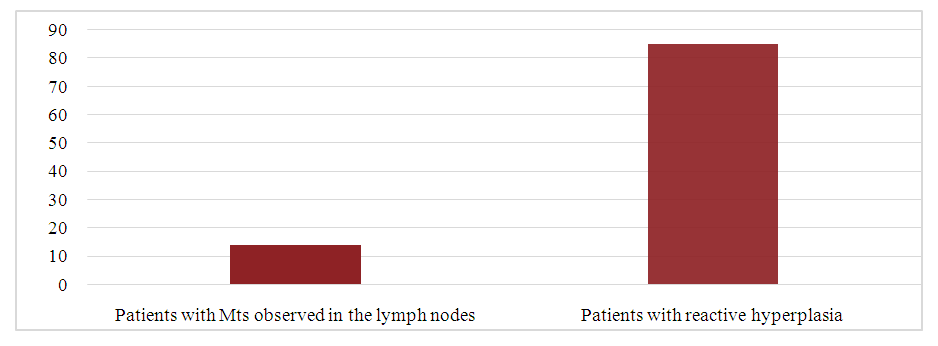
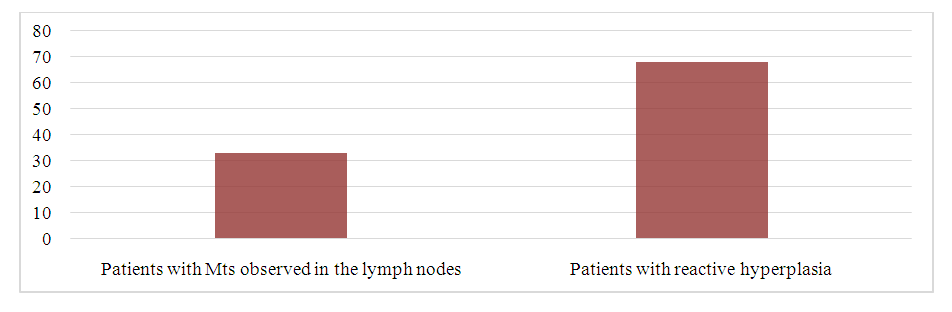
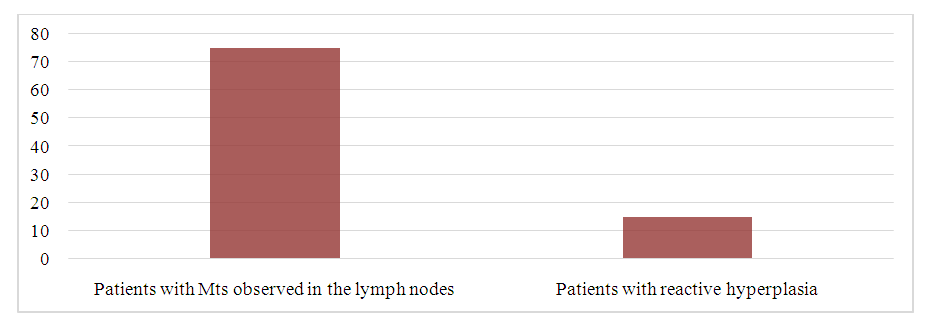
- 1. Based on the use of modern pathomorphological research methods, important criteria for the possibility of prognosis in patients with colon cancer were determined. Pathomorphological criteria for relapse and development of tumor growth in patients with colon cancer are: endophytic tumor growth, deep invasion, low level of differentiation.2. The occurrence of metastatic processes in patients was observed in 75% of cases with low differentiation of cancer, with moderate differentiation of tumors, metastasis occurred in 33% of cases, with high differentiation this figure is 15%, it is clear that the earlier the disease is diagnosed, the longer the duration and better the quality of life.3. Based on the studied molecular characteristics of patients with colon cancer, criteria for determining cases with a high risk of developing metastases were developed and a group of patients was studied.4. For the first time, the relationship between the expression of proliferation suppressors and apoptosis in patients with colon cancer was studied. The study of the expression of protein markers allowed us to determine their significance in predicting the outcome of patients with colon cancer with possible surgical intervention. The study showed the statistical reliability and significance of the studied immunohistochemical markers. Thus, in the group of patients with colon cancer, patients with a high proliferation index are significantly more common, and the proliferative activity of patients with colon cancer is more than 50%, which is a negative prognostic factor.5. As a result of the assessment of the cytokeratin-20 reagent status, the following data were obtained: hyperexpression of this protein (3+) was detected in patients with the tumor stage, which indicates amplification of the corresponding gene in tumor cells, with the onset of adipose tissue invasion, metastasis to the lymph nodes. Thus, as the stage of the disease increased, an increase in the expression of the Cytokeratin-20 reagent was noted, including hyperexpression, which was more pronounced in the presence of metastases in the regional lymph nodes. In the study, a positive reaction to the Cytokeratin-20 tumor marker was observed mainly with high differentiation, 3 out of 20 patients (15%) had a mild positive reaction, 15 patients (75%) had a moderate positive reaction, 2 (10%) had a high positive reaction. In moderately differentiated adenocarcinomas, a mild positive reaction was observed in 6 patients (30%), a moderate positive reaction in 7 patients (35%), and a high positive reaction in 7 patients (35%). In poorly differentiated adenocarcinomas, 2 patients (10%) had a low positive reaction, 7 patients (35%) had an intermediate positive reaction, and 11 patients (55%) had a high positive reaction. The results show that high positivity of Cytokeratin-20 at the level of cancer differentiation reduces the probability of its treatment, and a low level of differentiation increases the possibility of its aggressiveness. Thus, in this study, the cytokeratin-20 reagent was studied, and the parameters of marker expression in the pathomorphological assessment of colon tissue with a tumor showed the existence of their prognostic role, which is of great importance for considering it among the criteria when assessing the possibility of treating patients. 6. The results of immunohistochemical study obtained with p53 reagent showed that in the group with strong staining of tumor cells there is a risk of progression and relapse, therefore, overexpression of p53 can be a prognostic factor. Increased positivity with p53 reagent of proliferative activity in colon adenocarcinoma can be associated with a more specific mutation or blockade of the wild-type p53 tumor suppressor gene, which plays a central role in the development of apoptosis. The results obtained with p53 reagent showed that a correlation was found between the inhibition of apoptosis. During the study, a positive reaction to the p53 tumor marker was observed in 5 of 20 patients (25%), mainly in highly differentiated adenocarcinomas, with a moderate positive reaction. Moderate positive reaction was observed in 12 patients (60%), high positive reaction - in 3 patients (15%). In moderately differentiated adenocarcinomas, mild positive reaction was observed in 8 patients (40%), moderate positive reaction - in 6 patients (30%), and high positive reaction - in 4 patients (20%). In poorly differentiated adenocarcinomas, mild positive reaction was observed in 4 patients (20%), moderate positive reaction - in 8 patients (40%), and high positive reaction - in 8 patients (40%). The obtained results show that the higher the level of cancer differentiation, the higher the mutant gene, the higher the process of its aggressive escape. The most important factor in the development of tumor growth is the increase in general genetic instability, which leads to the appearance of additional markers necessary for metastasis. Firstly, this is aberration of genes leading to the formation of metastatic components of the p53 phenotype. Signs of tumor development are genetic features (chromosomal polymorphism, structural abnormalities of chromosomes and gene loci, mutation, increase or loss of protein production), for example, histological types of differentiation, tumor invasiveness, metastatic lesions. At the same time, identifying a group of genetic markers characterizing different levels of genomic instability associated with clinical and pathological parameters of rapid tumor development brings us closer to predicting the outcome of the disease in each patient, which is especially important for common and unfavorable forms. It should be noted that information about the variability of tumor markers that determine the impact on the prognosis of the disease contradicts the fact that it affects the formation of a certain gene and the rate of tumor growth. In this regard, it is necessary to strictly compare the observed changes in tumor development with their localization, the nature of mutations, clinical and morphological indicators and analysis of factors.