Akbarov M. M.1, Djumaniyazov D. A.2, Polvonniyozov Kh. G.1, Otamirzaev K. A.1
1The Department of Faculty and Hospital Surgery No.2 Tashkent Medical Academy, Uzbekistan
2The Department of Endoscopy of the State Institution "Republican Specialized Scientific and Practical Medical Center for Surgery named after Academician V.Vakhidov", Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The problem of gallstone disease, despite the current level of health care development, remains mainly a surgical problem, although a number of clinical situations require an integrated solution involving therapists, endoscopists, radiologists and doctors of other specialties. The study included 611 patients with gallstone disease complicated by mechanical jaundice for the period from 2021 to 2023, who, according to indications, underwent endoscopic retrograde cholangiopancreatography and endoscopic interventions. At the time of admission to the clinic, 174 (28.5%) patients had no mechanical jaundice, while 144 patients had a history of intermittent mechanical jaundice, and 30 patients had choledocholithiasis or choledoch ectasia on ultrasound. Being a minimally invasive intervention, endoscopic manipulations belong to the primary priority methods of diagnosis and treatment of patients with obstructive jaundice, however, despite their high diagnostic (93.5%) and therapeutic effectiveness (78%), a rational approach is needed, taking into account the likely risk factors for the development of complications specific to this type of intervention.
Keywords:
Cholelithiasis, Mechanical jaundice, Endobiliary interventions, Endoscopic papillosphincterotomy
Cite this paper: Akbarov M. M., Djumaniyazov D. A., Polvonniyozov Kh. G., Otamirzaev K. A., Endobiliary Interventions at the Stages of Treatment of Cholelithiasis Complicated by Mechanical Jaundice, American Journal of Medicine and Medical Sciences, Vol. 14 No. 12, 2024, pp. 3092-3097. doi: 10.5923/j.ajmms.20241412.02.
1. Introduction
The relevance of the problem. The problem of gallstone disease, despite the current level of health care development, remains mainly a surgical problem, although a number of clinical situations require an integrated solution involving therapists, endoscopists, radiologists and doctors of other specialties.In patients with gallstone disease (GD), choledocholithiasis occupies a leading place and is observed in 8.1-26.8% of cases [1,4], and in the group of patients older than 60 years, its frequency reaches 28.1% [3].The introduction into clinical practice of endoscopic retrograde cholangiopancreatography (ERCP), endoscopic papillosphincterotomy (EPST), endoscopic balloon papillodilation, endobilioprosthetics, as well as methods of laparoscopic sanitation of the common bile duct and the technology of minidos-tupa to the gallbladder, has opened up great opportunities for clinicians in the diagnosis and treatment of complicated forms of gallstone disease [1,2,5,6,7].Dissatisfaction with the results of treatment of GD, especially with a combination of mechanical jaundice and purulent cholangitis, has determined the need for comprehensive treatment of this category of patients using endovideosurgical techniques, endoscopic and endobiliary interventions.
2. Materials and Methods
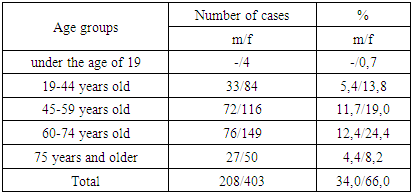
The study included 611 patients with gallstone disease complicated by mechanical jaundice who were in the clinic of the State Institution "Republican Specialized Scientific and Practical Medical Center for Surgery named after academician V.Vakhidov" for the period from 2021 to 2023, who, according to indications, underwent ERCP (or isolated ERCG, ERPG) and endoscopic interventions: Endoscopic papillosphincterotomy (EPST) or suprapapillary choledohodenostomy, after preliminary a suprapapillary fistula superimposed with a needle electrode. There were 249 (40.7%) patients with acute calculous cholecystitis, 362 (59.3%) patients with chronic calculous cholecystitis.The distribution of patients by gender and age is shown in Table 1. At the same time, women prevailed (ratio 1:1.9). The average age of the patients was 57.5±16.0 years.Table 1. Distribution of patients with gallstone disease by gender and age
 |
| |
|
The clinic of mechanical jaundice was observed in 436 patients (71.4%). The duration of anamnesis in 295 patients (48.3%) was 10 days or more, in other cases, patients were admitted to the clinic within 10 days from the onset of mechanical jaundice. Indications for emergency ERCP were ultrasound data and hyperbilirubinemia.Endoscopic examinations were performed with an OLYMPUS CV-170 video duodenoscope (Japan). X-ray monitoring was carried out using SIEMENS Siremobil Compact and Symbol devices.Diagnostic ERCP revealed that the main cause of mechanical jaundice in the study group of patients were: choledocholithiasis in 484 patients (79.2%); choledocholithiasis in combination with stenosing papillitis of the large duodenal papilla in 99 patients (16.2%); stenosis of the terminal choledochus in combination with stenosing papillitis of the large duodenal papilla in 20 patients (3.3%) and Mirizzi syndrome in 9 patients (1.4%).
3. Results and Discussion
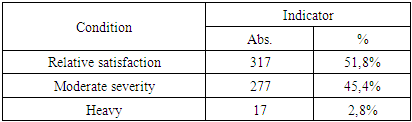
At the time of admission to the clinic, 174 (28.5%) patients had no mechanical jaundice, while 144 patients had a history of intermittent mechanical jaundice, and 30 patients had choledocholithiasis or choledoch ectasia on ultrasound. The assessment of the general condition of patients at admission according to the examination and anamnesis is shown in Table 2.Table 2. Assessment of the general condition of patients at admission according to the examination and anamnesis
 |
| |
|
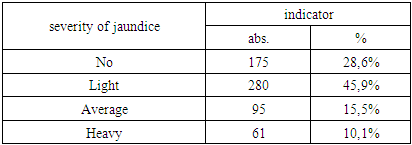
In the comprehensive assessment of mechanical jaundice according to the classification of Fedorov V.D. et al. (2000), which included the determination of not only bilirubin parameters, but also an assessment of the functional status of the liver – a severe degree was detected in 62 (10.1%) patients (Table 3).Table 3. A comprehensive assessment of the severity of mechanical jaundice according to Fedorov V.D. et al. (2000)
 |
| |
|
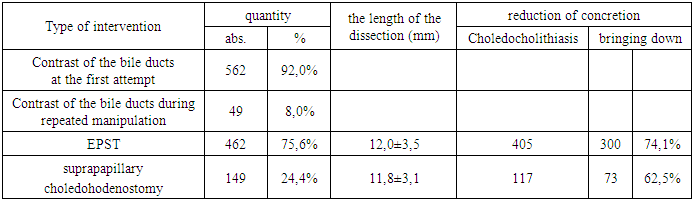
In our opinion, this is of fundamental importance in determining the prognosis of the disease, since in severe cases the mortality rate reaches 40%.When performing ERCG, bile duct contrast was obtained on the first attempt in 562 (92%) patients. In the remaining 49 (8%) cases, cannulation was performed with repeated manipulation, which was facilitated by portioned endoscopic papillotomy or suprapapillary fistula. According to the indications, endoscopic interventions were performed: EPST was performed in 462 (75.6%) patients, and suprapapillary choledohodenostomy was performed in 149 (24.4%) patients. At the same time, out of 300 observations of choledocholithiasis during EPST in 222 (74.1%) patients, it was possible to extract a concretion into the lumen of the duodenum 12. In the group of patients with choledocholithiasis, where suprapapillary choledohodenostomy was performed (117 patients), concretion from the choledochus was reduced in 73 (62.5%) cases. The length of the choledochodenostomy averaged 12 mm (Table 4).Table 4. Endoscopic therapeutic and diagnostic manipulations
 |
| |
|
With inadequate EPST and suprapapillary choledohodenostomy, additional dissection was performed to extract relatively larger concretions, usually within 4-6 mm. Thus, an additional expansion of the papillotomy opening was performed in 46 patients (7.5%), and an additional expansion of the suprapapillary choledohodenostomy was performed in 49 patients (8.0%).The type of endoscopic interventions depending on the etiology of mechanical jaundice against the background of GD is shown in Fig. 1.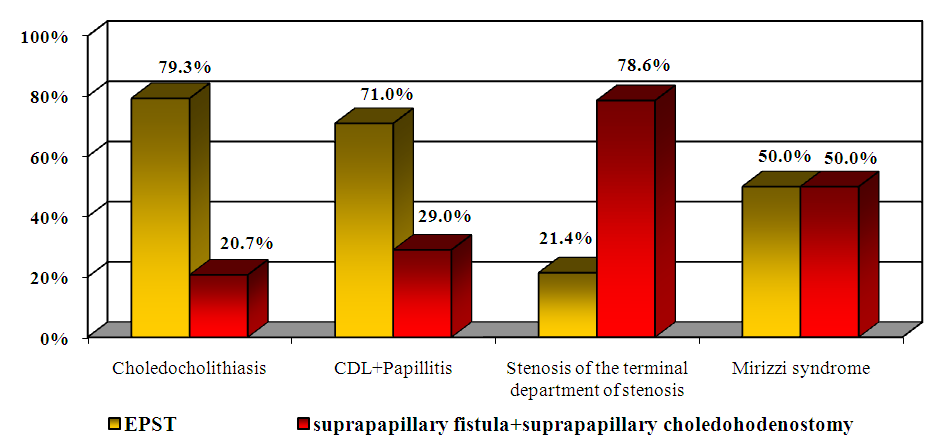 | Figure 1. Type of endoscopic interventions depending on the etiology of mechanical jaundice |
As can be seen from the above diagram, EPST was most often used in choledocholithiasis (79.3%) and its combination with papillitis (71%), and the frequency of suprapapillary choledochodenostomy in this pathology, on the contrary, was low, 20.7% and 29%, respectively. However, in the group of patients with terminal department of choledochus stenosis that makes EPST difficult, the frequency of suprapapillary choledohodenostomy was 78.6%, and EPST was only 21.4%. In Mirizzi syndrome, the frequency of both types of endoscopic interventions was the same.Among the etiological causes of mechanical jaundice, according to ERCG, choledocholithiasis was detected in 96.6% of cases and in 92% its combination with papillitis of the large duodenal papilla (Fig. 2). Stenosis of the terminal choledochus was determined in 19 (61.1%) patients, Mirizzi syndrome in 11 (33.3%) patients. The comparative diagnostic effectiveness according to ultrasound data was only 38.8%, whereas according to ERCG data it was 93.5%.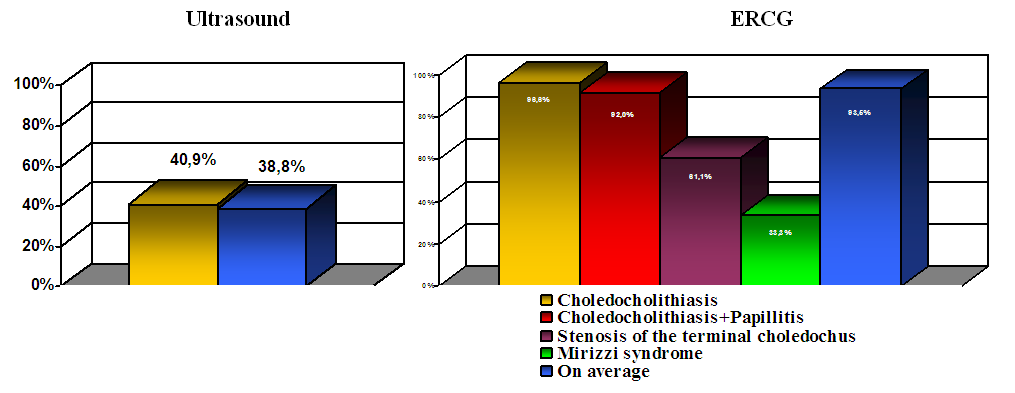 | Figure 2. Diagnostic effectiveness in verifying the etiology of obstructive jaundice |
An analysis of the frequency of complications depending on the type of endoscopic intervention performed showed that after suprapapillary interventions, bleeding of varying intensity was observed in 19 (12.5%) cases, after EPST in 31 cases (6.8%), and pancreatitis was observed in 8 (7.7%) and 16 (5%) cases, respectively. In 1 case, during suprapapillary choledohodenostomy, a perforation of the wall of the duodenum occurred, which required surgical intervention.Thus, the incidence of complications with suprapapillary fistula and suprapapillary choledohodenostomy in patients with GI was higher and amounted to 21.2%, with EPST this indicator was 11.8% (Fig. 3). | Figure 3. The frequency of complications depending on the type of endoscopic intervention |
In 91% of cases after EPST, bleeding from papillotomic edges was stopped by additional coagulation, 2 (9.1%) patients underwent emergency surgery due to ineffective hemostasis. 1 patient died. In suprapapillary choledohodenostomy, ineffective endoscopic hemostasis was found in 2 patients, which amounted to 15.4%. 1 patient died after the operation. 4 patients were operated on for acute pancreatitis provoked by retrograde intervention after EPST and suprapapillary choledohodenostomy. Mortality in the development of acute pancreatitis was 6.3% in the EPST group and 12.5% in the suprapapillary choledohodenostomy group.In general, the ineffectiveness of conservative measures for complications after endoscopic interventions required emergency surgery in 6 (15.8%) after EPST and in 7 (31.8%) after suprapapillary choledohodenostomy (Fig. 4).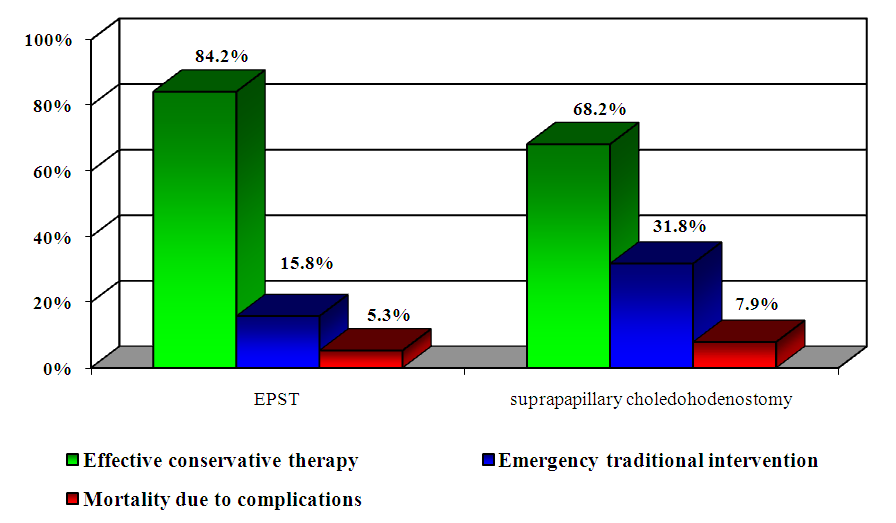 | Figure 4. Effectiveness of conservative measures for the treatment of complications after endoscopic interventions |
Among the total number of endoscopic interventions in 477 (78.0%) patients, the latter were effective in resolving the cause of mechanical jaundice. Thus, their effectiveness turned out to be virtually the same for the two methods, amounting to 78.9% (in 364 out of 462 patients) for EPST and 75% (in 112 out of 149 patients) for suprapapillary choledohodenostomy (Table 5).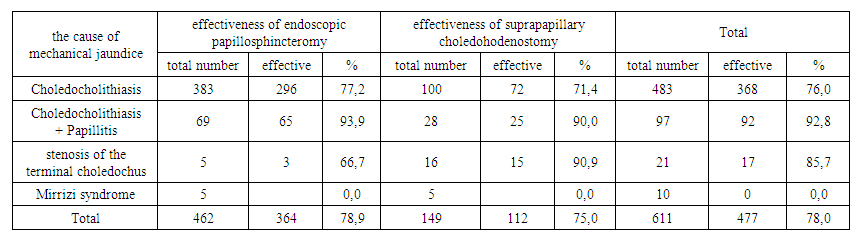 | Table 5. The effectiveness of endoscopic interventions in the resolution of mechanical jaundice |
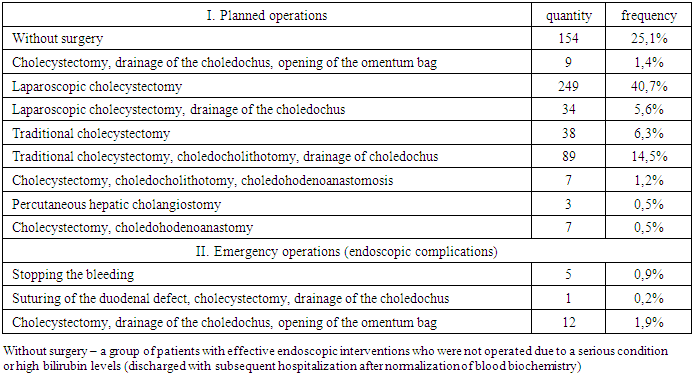
Among the entire group of patients with gallstone disease, 457 patients were operated on. At the same time, traditional interventions were performed in 172 cases and laparoscopic cholecystectomy was performed in 283 patients (Table 6).Table 6. Types of emergencies and planned surgical interventions performed in patients with gallstone disease after preventive endoscopic interventions
 |
| |
|
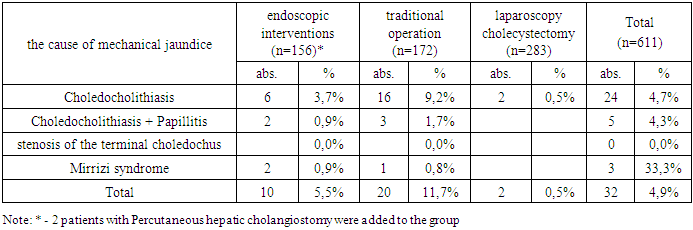
The total mortality rate was 4.9% (32 cases). Of this number, the mortality rate after traditional interventions was 11.7% (20 patients), endoscopic interventions – 5.5% (10 observations) and 0.5% (2 patients) after laparoscopic cholecystectomy (Table 7).Table 7. Mortality rate after performed interventions
 |
| |
|
The main cause of mortality in severe mechanical jaundice was hepatic or multiple organ failure. In milder degrees of mechanical jaundice, mortality was due to myocardial infarction and pulmonary embolism.
4. Conclusions
Being a minimally invasive intervention, endoscopic manipulations belong to the primary priority methods of diagnosis and treatment of patients with obstructive jaundice, however, despite their high diagnostic (93.5%) and therapeutic effectiveness (78%), a rational approach is needed, taking into account the likely risk factors for the development of complications specific to this type of intervention.Performing atypical endoscopic transpillary interventions causes an increased risk of developing specific complications, as the bleeding rate was 12.5% versus 6.8% for EPST, and ERCP-provoked acute pancreatitis was 7.7% versus 5%, respectively. At the same time, the ineffectiveness of conservative measures for complications after endoscopic interventions required emergency surgery in 6 (15.8%) after EPST and in 7 (31.8%) after suprapapillary choledohodenostomy.
References
| [1] | Briskin B.S., Gudkov A.N., Bryunin A.V., Kotovchikhina Y.A., Gaitukiev T.L., Mishina E.V. Modern tactics for cholelithiasis in patients with a high degree of operational risk // Annaly hirurgicheskoj gepatologii, 2002. - No1. – pp. 91-92. (In Russ.). |
| [2] | Karimov S.I. Endobiliary surgery in the treatment of mechanical jaundice // Annaly hirurgicheskoj gepatologii, 1996. - No1. – pp. 91-97. (In Russ.). |
| [3] | Nazirov F.G., Saatov R.R., Strussky L.P., Turakulov U.N., Saidazimov E.M. Endoscopic technologies in patients with external biliary fistulas // Materialy XI Moskovskogo Mezhdunarodnogo kongressa po jendoskopicheskoj hirurgii. – Moscow, 2007. – pp. 248-249. (In Russ.). |
| [4] | Kachmazova A.V., Teterin Yu.S., Tigiev L.R., Yartsev P.A., Rogal M.L., Bayramov R.S. Endoscopic treatment of patients with mechanical jaundice in Klatskin tumor // Hirurgija. Zhurnal imeni N.I. Pirogova, 2023. - No4. – pp. 55-60. (In Russ.). |
| [5] | Shuleshova A.G., Fomicheva N.V., Balalykin A.S., Danilov D.V. Confocal laser endomicroscopy in the diagnosis of extrahepatic bile duct strictures // Dokazatel'naja gastrojenterologija, 2018; 7(4): 1219. (In Russ.). |
| [6] | Sapaev D.Sh., R.Yu. Ruzibaev, B.N. Kuryazov, F.R. Yakubov. Problems of diagnostics, treatment and prevention of multiple hydatid echinococcosis of the liver // Vestnik of Saint Petersburg university. Medicine. –Sankt -Peterburg, 2019. –No 1 (14). –pp. 42 –48. |
| [7] | Vazquez-lglesias J.L., Gonzalez-Conde B., Lopez-Roses L. et al. Endoscopic sphincterotomy for prevention of the recurrence of acute biliary pancreatitis in patients with gallbladder in situ: long-term follow-up of 88 patients. Surg Endoscopy 2004; 18: 10: 1442-1446. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML