-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(11): 3084-3087
doi:10.5923/j.ajmms.20241411.89
Received: Oct. 22, 2024; Accepted: Nov. 28, 2024; Published: Nov. 30, 2024

Structure and Dynamics of Anxiety and Depressive Disorders in Patients with Epilepsy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTuraev Tolib Makhmudjonovich, Kuchimova Charos Azamatovna
Samarkand State Medical University, Uzbekistan
Correspondence to: Kuchimova Charos Azamatovna, Samarkand State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Epilepsy is one of the most common neuropsychiatric diseases. It should be noted, however, that modern scientific and practical studies aimed at students and doctors reflect only part of the problem of epilepsy (neurological, neurosurgical, psychiatric, neurophysiological), but do not give a holistic view of epilepsy as a complex, polymorphic disease. Despite the frequency of mental disorders in epilepsy, their place in the clinic and the dynamics of the disease have not yet been clarified. Recently, a new approach to studying the effect of the epileptic process on the functional state of the brain has begun to take shape, using 3 certain psychopathological disorders (anxiety, depressive, behavioral, ideational, communicative, etc.) that are caused by epileptic activity in the absence of epileptic seizures (V.A. Karlov, 2019; L.R. Zenkov et al., 2009, 2016, 2018; S.I. Shevelchinsky et al., 2019, 2020.) in connection with with the concept of epileptic encephalopathy. However, psychiatrists practically do not take any part in discussing these problems.
Keywords: Epileptic process, Anxiety disorders, Depression, Seizures, Panic disorders
Cite this paper: Turaev Tolib Makhmudjonovich, Kuchimova Charos Azamatovna, Structure and Dynamics of Anxiety and Depressive Disorders in Patients with Epilepsy, American Journal of Medicine and Medical Sciences, Vol. 14 No. 11, 2024, pp. 3084-3087. doi: 10.5923/j.ajmms.20241411.89.
Article Outline
1. The Purpose of the Study
- The study of all anxiety and depressive mental disorders of non-psychotic level in patients with epilepsy and the identification of the main pathogenetic factors causing their occurrence with the establishment of prognostic significance for the course of the disease.
2. Research Tasks
- 1. To identify the prevalence of ictal and interictal non-psychotic "mental" disorders in patients with epilepsy;2. To differentiate and systematize a variety of anxiety and depressive psychopathological manifestations in patients with epilepsy; 3. To identify the main pathogenic factors involved in the formation of anxiety and depressive disorders in patients with epilepsy; 4. To develop algorithms for providing assistance to epilepsy patients with non-psychotic affective disorders.
3. Research Materials
- The research was conducted in the dispensary department and day-patient hospital of the psychiatric hospital of Samarkand region during 2022-2023. A total of 144 patients with epilepsy, in whom depressive and anxiety disorders were determined by clinical and clinical-psychopathological methods. The study was carried out in the dispensary and full-time Departments of the Samarkand regional mental health hospital on the method of cellular selection. The study included 144 patients receiving treatment with epilepsy from 2022 to 2023. Respondents were identified by random selection and observed using retrospective and prospective methods. The nature of epilepsy has been clarified by clinical-psychopathological and psychometric examinations.
4. Research Methods
- Clinical-psychopathological, clinical-typological, clinical-catamnestic, psychometric, experimental-psychological, clinical-genealogical, statistical methods were used in scientific research. To solve the tasks set, the clinical and epidemiological research method was used as the main one. Special attention was paid to the psychopathological analysis and to the data of the catamnestic examination. These methods were used to study the features of the course of the disease, to clarify the nature, structure, dynamics of epileptic mental disorders, correlations between different variants of mental paroxysms and to establish differentiated prognostic criteria for epilepsy occurring with mental disorders. In addition, all patients underwent electrophysiological examination aimed at clarifying the localization of epileptic foci in epilepsy with mental paroxysmal and permanent disorders. The work also used data from pathopsychological, neuropsychological, neuro-ophthalmological, otoneurological, neurorentgenological, and neuroradiological studies in order to identify etiopathogenetic factors that are important for the occurrence of mental disorders in epilepsy. In assessing the nosological affiliation of the studied affective disorders, we used the ICD-10 criteria, namely, compliance with the signs of a depressive episode of mild (F32.0) and moderate severity (F32.1), mania without psychotic symptoms, cyclothymia (F34.0), dysthymia (F34.1), mixed anxiety and depressive disorder (F41.2).
5. Research Results
- Using the continuous sampling method, 144 patients with mental disorders were identified from all patients with epilepsy who were under observation in the Urban Neuropsychiatric Dispensary (812 people), which is 43%. Figure 1 shows all the varieties of interictal mental disorders identified by the method of continuous selection from all patients with epilepsy. Approximately the same proportion is occupied by patients with affective (18.9%), anxiety disorders (17.2%) and epileptic dementia (16%), and in very small numbers (taking into account the outpatient profile of the Urban Neuropsychiatric Dispensary) patients with epileptic psychoses (1%) and interstitial twilight obscurations (2%) were identified.
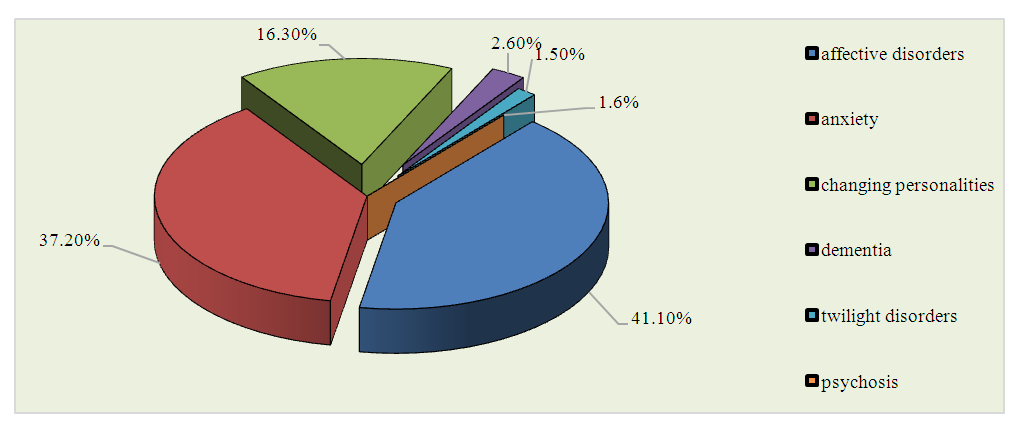 | Figure 1. The structure of interictal mental disorders |
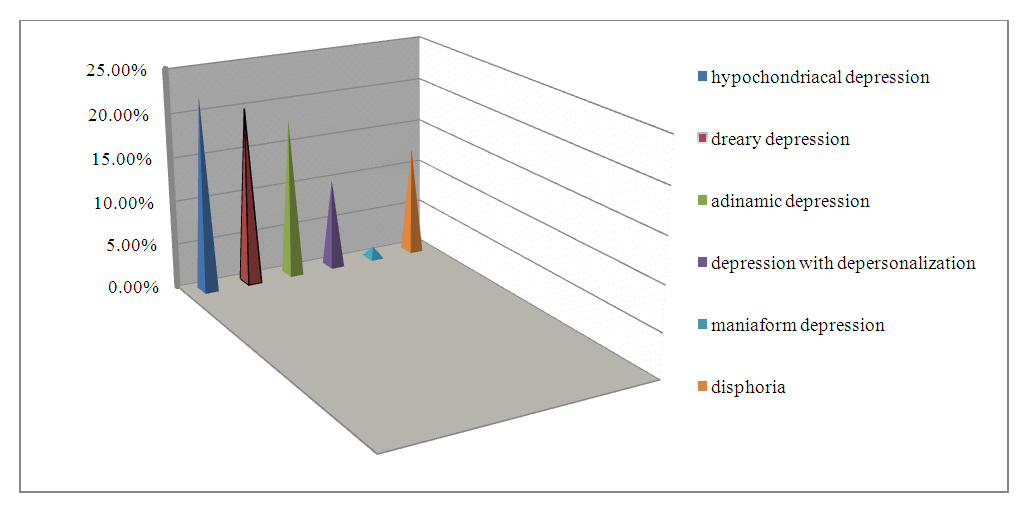 | Figure 2. The structure of interictal affective disorders in patients with epilepsy |
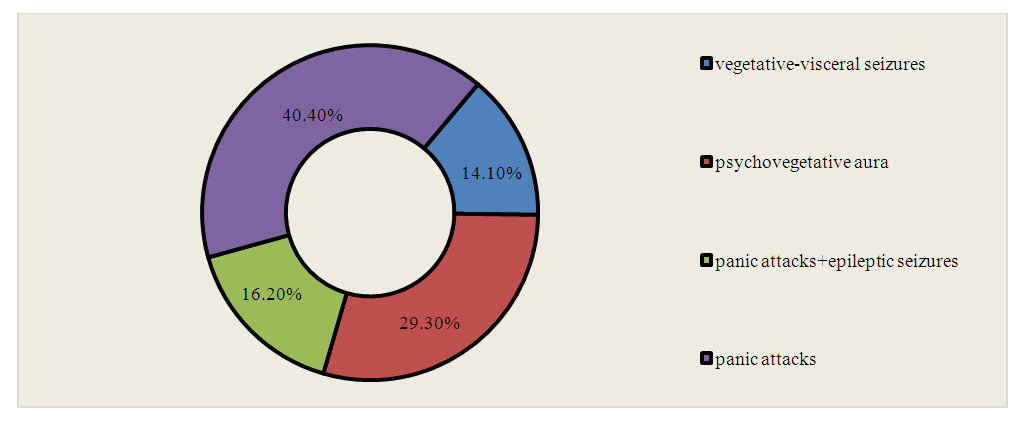 | Figure 3. The structure of anxiety disorders in patients with epilepsy |
|
|

6. Conclusions
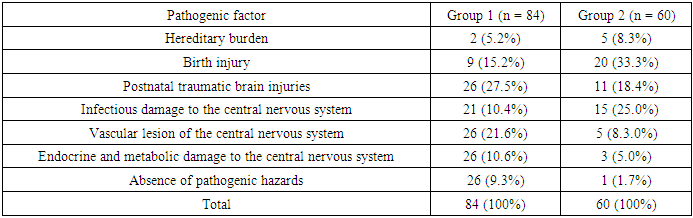
- Interictal affective disorders of non-psychotic level in patients with epilepsy are represented by: emotional lability (15.2%), dysphoric depression (12.6%), dreary depression (20.2%), hypochondriac depression (22.3%), anxiety depression (8.5%), asthenic depression (7.3%), adynamic depression (18.1%). 10.3% of epilepsy patients have depression with depersonalization. Mixed conditions are observed in 5.3% of patients. Patients with hysterical depression account for 4.1%. Maniform disorders without psychotic symptoms occur in 3.8% of patients, depression with obsessions - in 2.9% of patients. Among the pathogenic factors in patients with epilepsy with interictal affective disorders of a non-psychotic level, postnatal traumatic brain injuries, vascular and infectious lesions of the central nervous system are more often observed. In most patients with epilepsy, simple partial affective mental seizures respond well to treatment with antiepileptic drugs. In total, seizure cessation is detected in 69.3% of patients, a significant decrease in seizures occurs in 21.6% of patients, and a slight decrease in seizures occurs in 9.1% of cases. The results of the study showed that most often remission of affective mental seizures is achieved in monotherapy with valproates, topiramate, oxcarbazepine and levetiracetam, as well as in combination with topiramate oxcarbazepine or valproates and when carbamazepine is combined with valproates.