-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(11): 3078-3083
doi:10.5923/j.ajmms.20241411.88
Received: Oct. 20, 2024; Accepted: Nov. 26, 2024; Published: Nov. 30, 2024

Adrenalectomy Eliminates Hypergravity-Induced Suppression of Gastric Acid Secretion
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLUsanova Saodat Turayevna
Senior Lecturer at the Medical Faculty of the Alfraganus University, Uzbekistan
Correspondence to: Usanova Saodat Turayevna, Senior Lecturer at the Medical Faculty of the Alfraganus University, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Jet fighter pilots experience high gravitational acceleration forces in the head-to-foot direction (+Gz), which induce significant physiological stress, particularly affecting the gastrointestinal system. Although hypergravity's impact on cardiovascular and cerebral functions has been widely studied, its effects on gastric secretory activity remain insufficiently explored. Recent studies indicate that acute hypergravity exposure reduces gastric acid secretion, yet the underlying mechanisms are unclear. Objectives: This study aimed to investigate the role of adrenal glands in hypergravity-induced gastric acid hyposecretion and assess whether adrenalectomy could restore gastric secretory function under hypergravity conditions. Methods: Male Sprague-Dawley rats were divided into adrenalectomized and sham-operated groups. Gastric acid secretion was enhanced using the pylorus ligation technique. Both groups were subjected to +10Gz three times for 3 minutes each using a centrifuge, while a control group underwent no hypergravity exposure (+1Gz). Gastric juice parameters, including volume, total acidity, and pH, were measured, and plasma gastrin levels were analyzed using an enzyme-linked immunosorbent assay (ELISA). Results: In sham-operated rats, acute hypergravity significantly reduced gastric juice volume (P < 0.001) and total acidity (P < 0.001) while increasing pH (P < 0.001). However, adrenalectomized rats showed no significant differences in these parameters between hypergravity-exposed and nonexposed groups (P > 0.05). Plasma gastrin levels remained unaffected by hypergravity exposure in both adrenalectomized and sham-operated rats. Conclusion: Adrenalectomy prevented hypergravity-induced gastric acid hyposecretion, suggesting that the adrenal glands play a key role in this physiological response. These findings indicate that hypergravity-induced reductions in gastric acid secretion are mediated through the adrenal glands, likely via catecholamine release and subsequent splanchnic vasoconstriction. This study enhances understanding of the physiological mechanisms underlying stress-induced gastric dysfunction, with potential implications for managing gastrointestinal health in high-stress environments such as aviation.
Keywords: Adrenalectomy, Hypergravity, Gastric acid, Gastrin, Stress physiology, Gastrointestinal function
Cite this paper: Usanova Saodat Turayevna, Adrenalectomy Eliminates Hypergravity-Induced Suppression of Gastric Acid Secretion, American Journal of Medicine and Medical Sciences, Vol. 14 No. 11, 2024, pp. 3078-3083. doi: 10.5923/j.ajmms.20241411.88.
Article Outline
1. Introduction
- Gastric acid secretion is controlled by both the autonomic nervous system and hormones. The parasympathetic nervous system, along with gastrin, stimulates parietal cells to secrete gastric acid. This occurs through direct action on the parietal cells and indirectly via stimulation of histamine release from enterochromaffin-like cells [1]. The stomach’s highly acidic environment causes food proteins to unfold, exposing their peptide bonds. Chief cells in the stomach secrete the inactive enzyme pepsinogen [2], which is activated by gastric acid into pepsin. Pepsin aids digestion by breaking the peptide bonds between amino acids in a process called proteolysis. Additionally, the acidic environment inhibits the growth of many microorganisms, which helps prevent infections [1-3].Fighter jet pilots are exposed to extremely high gravitational acceleration forces, specifically in the cephalocaudal direction (+Gz). With the development of modern lightweight, high-thrust aircraft, G-force limits are primarily determined by the pilot’s physiology rather than by the aircraft’s performance or structural constraints. Military fighter pilots often experience sustained and repeated hypergravity, with forces reaching up to +9Gz. These forces, combined with the anti-G straining maneuver required to counteract them, cause significant changes in the autonomic nervous system, leading to severe physical and emotional stress [4,5].For this reason, it is essential for physicians and aviation medicine researchers to understand any pathophysiological changes induced by hypergravity. Numerous studies have documented various effects of human exposure to +Gz, including alterations in cerebral and coronary blood flow, cardiovascular reflexes, and endocrine responses [6-11].In addition to reducing cerebral and coronary blood flow, hypergravity leads to structural and functional changes in the visceral organs, particularly impairing visceral circulation [12,13]. A decrease in visceral blood flow is thought to result from a combination of hypergravity-induced cardiovascular reflex responses, stress-induced sympathetic vasoconstriction, and increased peripheral vascular resistance in visceral beds. Previous studies have shown that exposure to hypergravity significantly reduces blood flow to organs like the spleen, pancreas, liver, and kidneys, likely to ensure adequate blood flow to the brain and heart [12-14].The gastrointestinal system is particularly sensitive to stress, as shown by stress-induced changes in gastric acid secretion and intramucosal blood flow [15]. Although the effects of hypergravity exposure on cardiovascular and cerebral functions have been widely studied [7-9,13,14], its potential pathophysiological effects on the gastrointestinal tract remain unclear. Recently, we reported a significant reduction in gastric secretory activity in rats exposed to hypergravity [5]. To better understand this finding, it was essential to identify the mechanism behind hypergravity-induced gastric acid hyposecretion. Given previous research showing that hypergravity increases catecholamine levels from the adrenal glands and that sympathetic nervous system activation decreases gastric secretory activity [16,17], we hypothesized that hypergravity-induced gastric acid hyposecretion may be linked to adrenal gland function.To test this hypothesis, we examined the effects of bilateral adrenalectomy on gastric juice parameters and plasma gastrin levels in hypergravity-exposed rats. Continuing from our previous study, we used the pylorus ligation technique to induce gastric acid hypersecretion [5,18]. We measured several gastric juice parameters, including volume, acidity, pH, and plasma gastrin levels.
2. Results
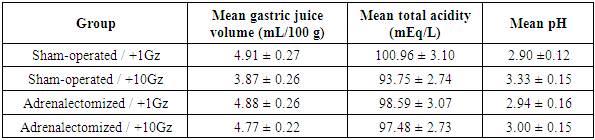
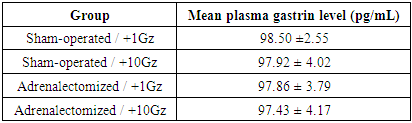
- Effects of hypergravity exposure and adrenalectomy on gastric juice parameters were first examined by comparing the differences between groups, as shown in Figure 1. Acute exposure to hypergravity significantly affected gastric juice parameters. In sham-operated rats, the gastric juice volume of hypergravity-exposed rats (3.87±0.26 mL/100 g) was significantly lower than that of nonexposed rats (4.91±0.27 mL/100 g; P < 0.001; Figure 1A). Similarly, the total gastric juice acidity in hypergravity-exposed rats (93.75±2.74 mEq/L) was significantly lower compared to nonexposed rats (100.96±3.10 mEq/L; P < 0.001; Figure 1B). Additionally, the gastric juice pH in hypergravity-exposed rats (3.33±0.15) was significantly higher than that in nonexposed rats (2.90±0.12; P < 0.001; Figure 1C). These findings are consistent with our previous data, which demonstrated that hypergravity exposure significantly decreases gastric juice volume and acidity while increasing its pH [5].
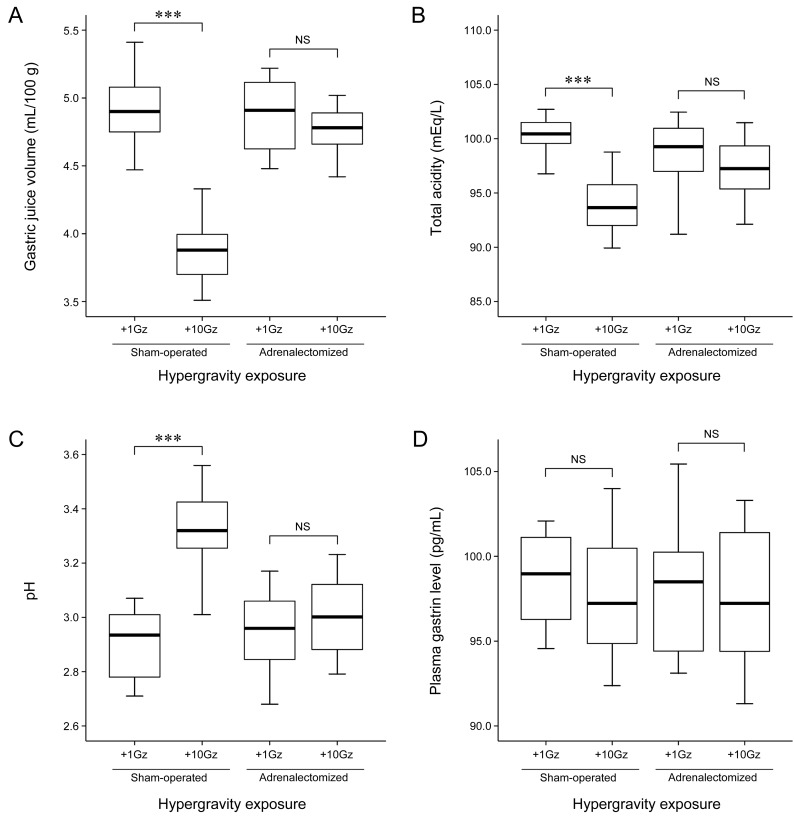 | Figure 1. Effects of adrenalectomy on gastric juice parameters and plasma gastrin level in hypergravity-exposed rats |
|
|
3. Discussion
- Gastric acid plays a crucial role in digestion by activating pepsin, which aids in breaking down proteins, and in killing bacteria. Stress-induced activation of the sympathetic nervous system inhibits gastric secretory activity by triggering catecholamine release from the adrenal glands. This reduction in gastric acidity significantly lowers pepsin activity, impairing protein digestion. Improperly digested proteins can become potentially harmful antigens in the body. In severe cases, insufficient protein breakdown may lead to gastroesophageal reflux and flatulence by causing proteins to remain in the stomach longer and increasing gastric acidity. Fighter pilots with gastrointestinal issues, such as dyspepsia, abdominal discomfort, or pain due to abnormal gastric secretory activity, may face significant challenges performing their tasks during flight [5].In our previous study, we found that hypergravity exposure significantly reduced the volume and acidity of gastric juice, while no significant differences were observed in plasma gastrin levels between hypergravity-exposed and nonexposed rats [5]. These results were reaffirmed in the present study. Acute hypergravity exposure inhibits gastric acid secretion, but the reductions in gastric juice volume and acidity observed during hypergravity exposure are unlikely to be related to gastrin. To our knowledge, no prior study has examined the specific mechanisms behind hypergravity's effects on gastric secretory activity.We hypothesized that acute hypergravity exposure stimulates the sympathetic nervous system, leading to increased catecholamine release from the adrenal glands and inhibiting gastric acid secretion. To test this hypothesis, we investigated the effects of adrenalectomy on gastric acid parameters. The hypergravity-induced decreases in gastric acid volume and acidity observed in sham-operated rats were absent in adrenalectomized, hypergravity-exposed rats. In other words, the changes in gastric acid parameters due to hypergravity were not statistically significant in the adrenalectomized rats. This suggests that adrenalectomy eliminates hypergravity-induced gastric acid hyposecretion, implicating the adrenal glands in this process.The hypergravity-induced reduction in visceral blood flow and the corresponding increases in plasma epinephrine, norepinephrine, and corticosterone levels support the theory that elevated catecholamine levels, driven by sympathetic nervous system stimulation, may cause splanchnic vasoconstriction, which slows blood flow to visceral organs, including the stomach [7,11-14,17]. In this study, we speculated that the hypergravity-induced reduction in gastric acid secretion may result from decreased blood flow to the stomach. Additionally, we cannot rule out the possibility that reduced acid secretion may also result from physical compression of gastric tissues as visceral organs shift downward under hypergravity forces.The relationship between gastric acid secretion and the adrenal glands in humans can vary depending on different pathophysiological conditions. Reduced gastric acidity and a lower incidence of chronic peptic ulcers in patients with adrenal insufficiency suggest the adrenal glands play a role in regulating gastric secretory activity [19]. Similarly, administering adrenal steroids or adrenocorticotropic hormone has been shown to increase gastric acidity and pepsin secretion, highlighting the adrenal glands' involvement in the development of peptic ulcer disease. Conversely, multiple gastrointestinal ulcers in the pyloric region of the stomach observed in patients with acute adrenal insufficiency indicate that adrenal function and gastric secretory activity are not always directly correlated [19].In humans, acute gastric ulcerative lesions resulting from absolute or relative adrenal insufficiency can be experimentally reproduced in animals exposed to severe stress following adrenalectomy [19]. This finding aligns with our results, which show increased gastric acid volume and acidity after adrenalectomy. Previous studies have suggested that changes in gastric secretory activity due to acute adrenal insufficiency may be linked to vascular stasis and cellular damage caused by dehydration and electrolyte imbalance [19]. Histologically, ulcerative lesions associated with acute adrenal insufficiency tend to be multiple and superficial, while lesions resulting from adrenal replacement therapy are more likely to be discrete, deep, and chronic peptic ulcers, particularly when the hormone is administered over a prolonged period.Clinical assessments of changes in gastric pathophysiology due to adrenal hypo- or hyperfunction, or excessive adrenal hormone administration, should consider alterations in the mucosal barrier, interference with tissue repair, and decreased tissue resistance caused by vascular and metabolic disturbances, alongside changes in secretory activity.In conclusion, our study demonstrated that adrenalectomy prevents hypergravity-induced gastric acid hyposecretion but does not affect gastrin release. These findings suggest that the adrenal glands play a key role in hypergravity-induced gastric acid hyposecretion.
4. Materials and Methods
- Experimental AnimalMale Sprague-Dawley rats, aged 10-11 weeks and weighing 280-300 g, were used for the study. They were fed standard laboratory rat chow, had free access to water, and were housed under controlled conditions, including a 12-hour light-dark cycle, with temperature maintained at 20-25°C and humidity levels at 40-45%. To minimize the impact of stress and fear, the rats were allowed to acclimate to their environment for 7 days prior to the experiment. All experimental procedures involving the animals were approved by the Institutional Animal Care and Use Committee of the Republic of Uzbekistan. The procedures were carried out in accordance with the Guide for the Care and Use of Laboratory Animals published by the National Institutes of Health and followed the ethical guidelines set by the International Association for the Study of Pain.Bilateral AdrenalectomyThe rats were divided into two groups: adrenalectomized (n = 24) and sham-operated (n = 21). Bilateral adrenalectomy was carried out using a dorsal approach. A one-inch midline incision was made along the back, and after shifting the incision towards each side of the kidneys, a small cut was made in the muscle just behind the last rib. The adrenal glands were located near the kidneys and removed. In the sham-operated group, the same procedure was followed, except the adrenal glands were grasped but not excised. After surgery, the adrenalectomized rats were given physiological saline (0.9% sodium chloride) in place of drinking water. The rats were kept in a warm environment (25°C) in the laboratory for 6 hours post-surgery for observation, after which they were returned to the housing unit.Pylorus Ligation and Hypergravity ExposureIn our previous study, we confirmed that pylorus ligation enhances gastric secretory activity and that acute hypergravity exposure negatively impacts gastric acid secretion [5]. The objective of this study was to investigate the restorative effect of adrenalectomy on gastric secretory function under the same conditions as in the previous study. Under light anesthesia, a laparotomy was performed through a midline incision of approximately 3 cm. The pyloric region of the stomach was gently isolated and tied off with a 4-0 silk suture around the pyloric sphincter [5, 20]. The incision was then closed with 3-0 silk sutures. Thirteen adrenalectomized rats and 11 sham-operated rats were exposed to +10Gz three times for 3 minutes each (onset rate, +1Gz/s) using a small-animal centrifuge. Each rat was placed in a cylindrical plastic restraint device, which, when mounted in the centrifuge, aligned the +Gz force along the rostrocaudal axis. After securing the rats, the restraint device was clamped to the centrifuge arm, which allowed one degree of freedom, ensuring that the net G force was perpendicular to the floor of the restraint device [5,21-23]. Rats in the hypergravity-nonexposed group (+1Gz) were placed in the centrifuge arm and underwent the same process, but without hypergravity exposure. Throughout the centrifugation experiments, the behavior of the rats was monitored using a charge-coupled device camera. None of the rats died as a result of the surgical procedure or hypergravity exposure.Measurement of Gastric Juice ParametersThree hours after pylorus ligation, the rats were euthanized. The abdomen was opened, the stomach was removed, and the gastric contents were collected and centrifuged at 8,000×g for 10 minutes at 25°C. The volume (mL/100 g), total acidity (mEq/L), and pH of the gastric juice were measured. Total acidity was determined by titrating to pH 7.0 using 0.01 N sodium hydroxide with phenolphthalein as an indicator. The pH was measured using a digital pH meter.Measurement of Plasma Gastrin LevelJust before removing the stomach, blood samples were collected from the abdominal aorta. The heparinized blood was centrifuged at 3,000×g for 10 minutes, and the plasma was stored at –20°C until further analysis. Plasma gastrin levels were measured using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (Abcam, Cambridge, UK).Statistical AnalysisAll data are expressed as mean ± standard error. Differences between groups were analyzed using one-way analysis of variance (ANOVA), followed by Tukey's multiple range test. Statistical analyses were performed using PASW Statistics for Windows (version 18.0; Armonk, NY, USA). A P value of less than 0.05 was considered statistically significant.
ACKNOWLEDGMENTS
- The authors acknowledge that the views and opinions presented in this article are solely their own and do not represent the official policies or positions of the Republic of Uzbekistan Air Force.
Conflicts of Interest
- The author declares that she has no conflicts of interest.
Fund Support
- This research was supported and funded by the Ministry of Education of the republic of Uzbekistan.