-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(11): 3071-3073
doi:10.5923/j.ajmms.20241411.86
Received: Nov. 10, 2024; Accepted: Nov. 26, 2024; Published: Nov. 29, 2024

Monitoring of Differential Diagnostic Features of Rosacea Keratitis and Rosacea Corneal Ulcers
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdullaev Sherzod Rakhmatovich, Kamilov Khalidjan Makhamadzhanovich, Babakhanova Dilaram Mukhutdinovna, Maksudova Laylo Maskhutovna
Center for Development of Professional Qualifications of Medical Workers, Ministry of Health of the Republic of Uzbekistan, Tashkent, Republic of Uzbekistan
Correspondence to: Abdullaev Sherzod Rakhmatovich, Center for Development of Professional Qualifications of Medical Workers, Ministry of Health of the Republic of Uzbekistan, Tashkent, Republic of Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Rosacea is a very common chronic facial skin disease with involvement of small vessels and sebaceous-hair follicles. Until recently, rosacea was considered to be exclusively a dermatological disease, although in a significant proportion of patients who present, the clinical manifestations of this pathology may be localized in the eye area. About one third of patients with rosacea and ophthalmorosacea have corneal lesions that lead to visual acuity impairment. Rosacea has a chronic recurrent course, with progressive symptoms. Exogenous and endogenous factors are known to worsen the course of the dermatosis and contribute to the development of another exacerbation: exposure to ultraviolet rays, spicy or salty food, alcohol consumption, exposure to extreme temperatures, physical exercise, menopause, excessive emotionality, hormonal, immune and endocrine dysfunctions, avitaminosis, gastrointestinal disorders, etc. The ocular form of rosacea or ophtalmorosacea is characterized by a variety of clinical manifestations.
Keywords: Rosacea, Ophthalmorosacea, Keratitis, Corneal ulcer, Treatment
Cite this paper: Abdullaev Sherzod Rakhmatovich, Kamilov Khalidjan Makhamadzhanovich, Babakhanova Dilaram Mukhutdinovna, Maksudova Laylo Maskhutovna, Monitoring of Differential Diagnostic Features of Rosacea Keratitis and Rosacea Corneal Ulcers, American Journal of Medicine and Medical Sciences, Vol. 14 No. 11, 2024, pp. 3071-3073. doi: 10.5923/j.ajmms.20241411.86.
1. Relevance
- Rosacea has a chronic recurrent course, with progressive symptoms. Exogenous and endogenous factors that worsen the course of the dermatosis and contribute to the development of another exacerbation are known: exposure to ultraviolet rays, spicy or salty food, alcohol consumption, exposure to extreme temperatures, exercise, menopause, excessive emotionality, hormonal, immune and endocrine dysfunctions, avitaminosis, gastrointestinal disorders, etc. [1,3].The ocular form of rosacea or ophthalmorosacea is characterized by a variety of clinical manifestations. One of the most fequent forms of ophthalmorosacea is corneal involvement in the form of rosacea keratitis and corneal ulceration (up to 30% of all cases). Corneal lesions are usually bilateral, accompanied by a significant decrease in visual functions, and the severity of eye damage often does not correlate with the severity of cutaneous manifestations of rosacea [2].In this case, almost half of patients, rosacea keratitis occurs after skin manifestations of rosacea in the form of pink acne, and in 20% of patients - before skin rashes. In the remaining cases, the skin and eye lesions occur simultaneously. The disease has a progressive recurrent course, which often leads to blindness.The causes that give rise to the development of rosacea keratitis, as in the case of the skin disease acne rosacea, are unknown. In our observations, as well as according to the literature, a certain role was played by chronic diseases of the gastrointestinal tract (cholecystitis, gastritis, helicobacter infection), endocrinopathies (diabetes mellitus, hypothyroidism, dysmenorrhea), neurovegetative disorders (hypertension, vegetative dystonia), heredity, vitamin deficiency - hypovitaminosis A, E, B6, B12. The etiological role of the demodex mite has been proved not only in the development of the cutaneous form of rosacea, but also in rosacea keratitis [5]. According to the working classification, corneal lesions in ophthalmorosacea may clinically manifest as superficial marginal infiltrate, subepithelial infiltrate and progressive corneal ulceration [6]. The superficial form is characterized by the formation of grayish-white infiltrates near the limbus, slightly elevated above the cornea with single superficial vessels. The infiltrates eventually disintegrate with the formation of ulcers, which, after epithelialization, leave minor corneal opacities [4].Subepithelial infiltrates are characterized by small gray convex nodules located under the corneal epithelium. The disintegration of such nodules is accompanied by ulceration, vascularization, and the deposition of calcium salts, which causes the formation of chalky corneal opacity [8].In progressive rosacea keratitis, an extensive ulcer forms, similar to a creeping ulcer, has a valley-like raised edge and an opposite flat edge, to which rough newly formed vessels extend [7].Purpose of the work. To study differential diagnostic signs of rosacea -keratitis and rosacea -corneal ulcers.
2. Materials and Methods
- Twelve patients (24 eyes) with ophthalmorosacea were under our observation. One them 1 male and 11 females. The mean age of the patients was 38.6+3.2 and ranged from 28 years to 65 years. Ophthalmologic examination included visometry, perimetry, biomicroscopy, anterior optical coherence tomography to determine the depth and area of the corneal ulcer, ocular ultrasound (B-scan), and pachymetry. Corneal epithelial defects were detected by instillation of fluorescein solution and lissamen green. To detect demodectic mite, epilated specimens of eyelashes and scrapings from the patient's facial skin were examined. The degree of tear production disorder was determined by Schirmer’s and Norn’s tests. The function of meibomian glands was determined on the LacriDiag apparatus. Laboratory studies in addition to general blood and urine tests included blood biochemistry, HALC complex – Helicobacter + Ascaris + Lamblia + Candida, microscopy of eyelashes and facial skin scrapings for demodicosis, immunogram of blood and tears, stool analysis, if indicated - seeding the conjunctival cavity with determination of sensitivity to antibiotics.
3. Results and Discussion
- Out of the 12 patients with ophthalmorosacea, 8 patients were found to have rosacea keratitis and 4 patients had rosacea corneal ulceration.When patients came to us, they complained of burning and pain in the eyes, redness, lacrimation and photophobia, a feeling of a foreign bodies and sand in the eyes, and vision loss of varying degrees. When examining the patients we paid attention to the facial skin: all 12 patients had skin manifestations of varying degrees of severity: from insignificant erythema of the cheeks, nose, forehead or telangiectasia and desquamation to bright red papulo-pustular rashes and hypertrophic phimosis changes of the skin of certain parts of the face. On the eye side, the following was observed: pericorneal or mixed injection of the conjunctiva of the eyeball, in 3 patients - mucopurulent discharge, in 10 patients - telangiectasias on the eyelid skin. Chronic blepharitis was diagnosed in 8 patients and chalazion in 4 patients. For correct diagnosis of rosacea keratitis (Fig.1) and rosacea-ulcers (Fig.2) of the cornea, some diagnostic studies were performed together with dermatovenerologists, endocrinologists and gastroenterologists.
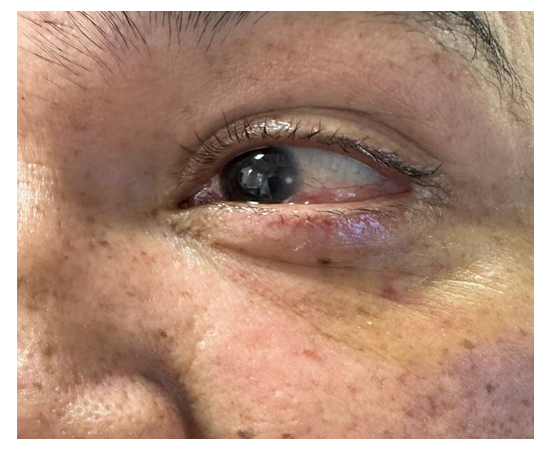 | Figure 1. Patient Sh.K., 32 years old. Rosacea with ophthalmorosacea (marginal keratitis with descemetocele) |
 | Figure 2. Patient A.G., 43 years old. Rosacea, marginal rosacea keratitis with vascularization |
4. Conclusions
- Thus, in our studies, ophthalmorosacea with involvement of the cornea in the inflammatory process involvement process was 11 times more frequent in women than in men. Among patients with ophthalmorosacea and corneal lesions, rosacea keratitis was 2 times more frequent than rosacea-corneal of the cornea. Treatment of corneal manifestations of rosacea is performed in conjunction with dermatovenerologists and other specialists as needed. Systemic and local application of antibiotics, Metronidazole, lubricants, vitamins, immunomodulators in the treatment of ophthalmorosacea allows to obtain a rapid clinical effect.