Islamov Khurshid Jamshidovich
Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, Tashkent, Uzbekistan
Correspondence to: Islamov Khurshid Jamshidovich, Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, Tashkent, Uzbekistan.
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
This study was performed on the basis of the coloproctology department of the Republican Medical Specialized Scientific and Practical Center of Oncology and Radiology in Tashkent. The retrospective group included data on 360 patients with colorectal cancer of stage II-IV of the disease who received surgical treatment in the department of Coloproctology of the Republican Medical Specialized Scientific and Practical Center of Oncology and Radiology. The minimum mandatory set of diagnostic measures to determine the primary distant metastases of CRC is the analysis of the results of UAC, elevated levels of REA and CA19-9, the presence of metatstases according to the results of MRI.
Keywords:
Colorectal cancer, Metastasis, Diagnosis, Predictors
Cite this paper: Islamov Khurshid Jamshidovich, A New Stage in the Diagnosis of Metastatic Colorectal Cancer, American Journal of Medicine and Medical Sciences, Vol. 14 No. 11, 2024, pp. 3051-3055. doi: 10.5923/j.ajmms.20241411.82.
1. Introduction
In 2020, about 1.9 million people fell ill with colorectal cancer (CRC), and about 900,000 died, making it the second most fatal cancer after lung cancer [4]. The highest incidence in the world is observed in North America, Europe and Oceania, but the incidence is also increasing in countries with economies in transition, such as Russia, China and Brazil [1], which makes the disease an indicator of socio-economic development. CRC affects men more than women. With a global incidence of 23.4 per 100,000 male and 16.2 per 100,000 female population. CRC is a rare disease at a young age (under 40 years old), most cases occur in the age group of 70 years and older [3]. However, there are reports of an increase in morbidity in younger age groups and that young people are diagnosed with later tumors, which indicates a real increase in morbidity, and not only a consequence of an earlier diagnosis [2,6].Inflammatory bowel diseases (IBD), i.e. Crohn's disease and ulcerative colitis, increase the risk of developing CRC. Patients with IBD are under colonoscopic supervision, and the mortality rate from CRC in patients with IBD is decreasing.The International Agency for Research on Cancer and the American Institute of Cancer Research published the report "Diet, Nutrition, Physical Activity and Colorectal Cancer in 2018", in which they reviewed published studies on lifestyle factors and CRC. They claim that the consumption of red and processed meat increases the risk of colorectal cancer, the same can be said about taking two or more servings of alcohol per day. In addition, obesity, as well as higher height, increase the risk of CRC [7]. Also, cigarette smoking increases the risk of colorectal cancer, moreover, it has been proven that the risk of CRC associated with smoking is for the rectum than for the colon [5].The purpose of the study. To improve a multidisciplinary approach for the timely diagnosis of metastatic colorectal cancer.
2. Material and Methods
This study was performed on the basis of the coloproctology department of the Republican Medical Specialized Scientific and Practical Center of Oncology and Radiology in Tashkent.The retrospective group included data on 360 patients with colorectal cancer of stage II-IV of the disease who received surgical treatment in the department of Coloproctology of the Republican Medical Specialized Scientific and Practical Center of Oncology and Radiology. The study did not include patients with primary multiple synchronous/metachronous malignant neoplasms, patients who received surgical treatment for malignant neoplasm of the colorectal zone in other medical institutions of the Republic of Uzbekistan.The diagnosis was established on the basis of complaints, anamnesis, physical examination, morphological examination of tumor material, data from instrumental and laboratory examination methods. Patients received adjuvant/neoadjuvant treatment in accordance with the current algorithms for the diagnosis and treatment of colorectal cancer patients approved by the Ministry of Health of the Republic of Uzbekistan. The research material was: peripheral blood of patients, paraffin blocks of tumor tissue, freshly frozen tumor and normal colon tissues, isolated circulating tumor cells.The prospective group included data on 105 patients with metastatic colorectal cancer II-IV.IBM SPSS Statistics 23 (Stat Soft, USA) and MedCalc 19.3.0 (MedCalc Software bv, USA) programs were used to process the primary research materials.The estimation of the distribution of values and the difference from the normal distribution were analyzed according to the Shapiro-Wilk criterion. In the presence of a normal distribution of indicators, the Student-Fisher criterion was used to assess the statistical significance of differences; in the absence of a normal distribution, the Mann–Whitney criterion was used.
3. Results
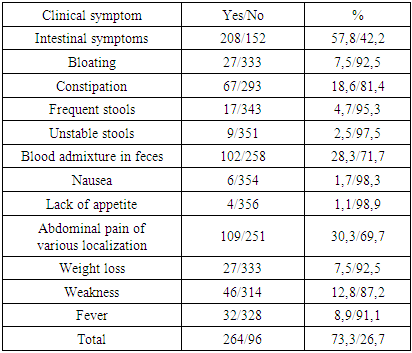
Based on the data of the outpatient disease chart, medical history and patient survey, the frequency of occurrence of clinical symptoms of CRC in a group of patients was assessed. In the study of the clinical status, the presence of symptoms of the disease in patients with CRC was studied. Clinical manifestations of the disease were noted in 264 (73.3%) patients. Intestinal symptoms were noted in 208 patients (57.9%) (Table 1).Table 1. Clinical signs of patients with CRC
 |
| |
|
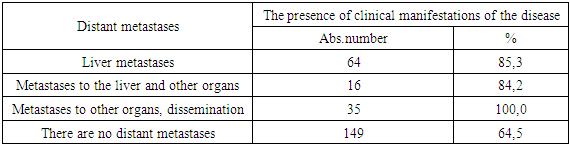
As can be seen from the data presented in Table 1, the most common symptoms in patients with CRC were intestinal manifestations: abdominal pain of various localization (30.3%), blood admixture in feces (28.3%) and constipation (18.6%). Symptoms such as general weakness and fever were noted in 12.8% and 8.9% of cases.The overall survival rate of patients included in the study group was assessed, depending on the presence or absence of the studied symptoms.The 5-year overall survival rate in the group of patients without clinical symptoms (63.9±6.0%) is slightly higher (p=0.053) than in the group of patients with clinical manifestation of the disease (52.6±3.7%). The median overall survival was 81.0 months (95% CI 53.6-108.4) in the group of patients without clinical manifestations and 70.0 months (95% CI 52.8-87.2%) in the group of patients with clinical manifestations.Correlation analysis revealed a statistically significant correlation between the presence of clinical manifestations of the disease and the stage of the disease (p<0.001) and the presence of distant metastases (p<0.001). Table 2 shows the distribution of the frequency of clinical manifestations depending on the presence of distant metastases.Table 2. Frequency of clinical manifestations depending on the presence of distant metastases
 |
| |
|
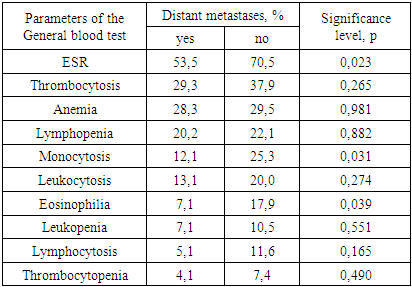
In the presence of distant metastases, patients noted clinical symptoms of the disease significantly more often than in their absence (p<0.001). Also, with an increase in the stage of the disease, the frequency of detection of clinical symptoms increases.Among patients with distant metastases, 30 people (85.7%) complained about intestinal symptoms, the most common manifestations were constipation in 13 (37.1%), blood admixture in feces in 14 (40.0%) and abdominal pain in 23 (65.7%). Complaints of weakness were made by 7 patients (20.0%), fever – 3 (8.6%).The frequency of changes in the total blood count was noted in 235 patients (65.3%). Among laboratory parameters, an increase in ESR was the most frequent and was observed in 120 (33.3%) patients, among patients with changes in the UAC. Thrombocytosis was observed in 65 patients (18.1%), anemia, of varying severity – in 56 (15.6%) patients.UAC changes were noted significantly (p<0.001) more often in the group of patients with distant metastases (76.7%) than among patients without them (40.3%). At the same time, in the group of patients without distant metastases, changes in ESR, monocytosis and eosinophilia were significantly more often noted than among patients with distant metastases (Table 3).Table 3. The frequency of changes in the general blood test (GBT) depending on the presence of distant metastases
 |
| |
|
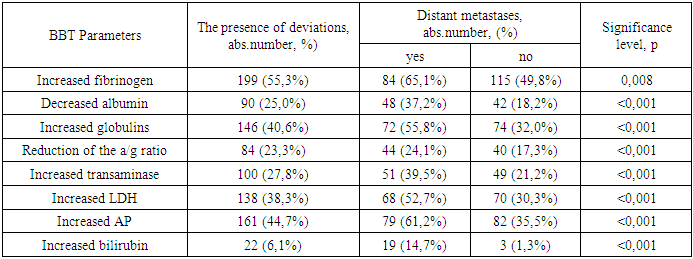
Changes in the biochemical blood test (BBT) were detected in 304 (84.4%) patients. Individual biochemical parameters were assessed by the frequency of deviations from the norm. Among them are fibrinogen, globulin, alkaline phosphatase (AP), bilirubin, albumin, a/g coefficient, transaminases (ALT and AST), LDH. Table 4 shows the results of the analysis of BAC indicators in patients with CRC for individual biochemical parameters. An increase in fibrinogen levels was detected in 199 patients (55.3%), globulins – in 146 (40.6%), transaminases – in 100 (27.8%), LDH – in 138 (38.3%), alkaline phosphatase – 161 (44.7%), bilirubin – 22 (6.1%). A decrease in such indicators as albumin concentration and a/g coefficient was detected in 90 (25.0%) and 84 (23.3%) patients, respectively. In the presence of distant metastases, changes in the tank, both in general and in the analysis of individual biochemical parameters, were significantly more common than in the group of patients without primary distant metastases.Table 4. The frequency of changes in the biochemical analysis of blood depending on the presence of distant metastases
 |
| |
|
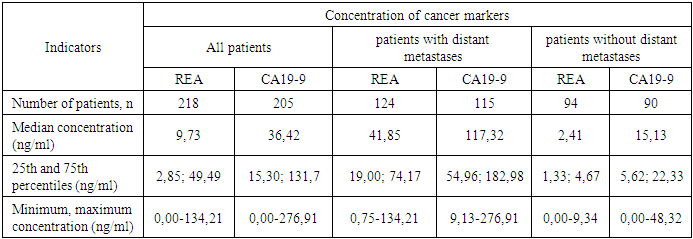
In addition to the indicators of GBT and BBT, the level of REA and CA19-9 was assessed in patients with CRC. Thus, the assessment of the concentration of REA was carried out in 218 (60.6%) patients, CA19-9 – in 205 (56.9%).Table 5. The frequency of changes in the concentration of tumor markers in patients with colorectal cancer
 |
| |
|
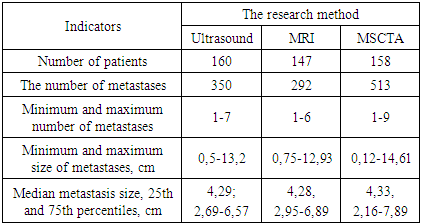
An increase in the concentration of CA19-9 was detected in 105 patients (51.2%), REA – in 135 (61.9%). Among patients with primary distant metastases, an increase in the concentration of CA19-9 and REA was significantly more frequent than in the group of patients without distant metastases (p<0.001). All patients included in the study group were examined according to protocols for the diagnosis and treatment of colorectal cancer approved by the Ministry of Health of the Republic of Uzbekistan. To determine the metastatic lesion, the following diagnostic methods were used: ultrasound examination (ultrasound) conducted at the place of residence, ultrasound at the RNPC, MSCTA, MRI, X-ray examination of BP and OGK, MSCT GCT, positron emission tomography (PET-CT has been performed in patients since 2020).The most frequent diagnostic study (Table 6), to identify metastases, was ultrasound – 344 (95.6%) patients. Ultrasound in the RNPC was performed in 333 patients (92.5%), ultrasound at the place of residence – 255 (70.8%), MRI – 327 (90.8%), MSCT OGK – 326 (90.6%), MSCTA – 325 (90.3%), 321 X-ray examination – 321 (89.2%), PET-CT – 33 (9.2%). The small number of patients who underwent PET_CT is primarily due to the fact that this study was not a mandatory component of diagnostic measures approved by the Ministry of Health, and secondly, it was not widely available to the public during the study period. Table 6 shows the number of distant metastases and their sizes detected using various instrumental methods (ultrasound, MRI, MSCTA).Table 6. The number and size of metastases detected during radiation diagnostics
 |
| |
|
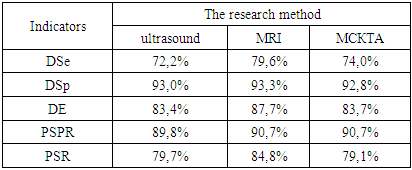
So, based on the data obtained, the largest number of metastases was described in the results of MSCTA – 513 units in 158 patients, 350 units were described using ultrasound. metastases in 160 patients, with MRI – 292 metastases in 147 patients.Histologically confirmed metastases were found in 129 patients. To determine the most effective method of diagnosing distant metastases, an assessment of diagnostic sensitivity (DS), diagnostic specificity (DS), diagnostic efficacy (DE), the prognostic significance of a positive result (PSPR) and the prognostic significance of a negative result (PSR) was carried out. Table 7 shows the results of the assessment.Table 7. Evaluation of the effectiveness of instrumental methods for the diagnosis of distant metastases
 |
| |
|
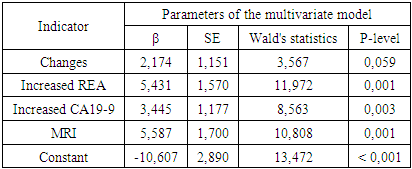
The highest results were obtained during the MRI examination. PET-CT was not evaluated due to the small number of studies conducted. At the same time, during PET-CT studies, distant metastases were identified and confirmed histologically in 100% of cases.Separately, the effectiveness of instrumental diagnostic methods in determining liver metastases was evaluated. Primary metastatic liver damage, histologically confirmed, was in 75 patients, liver and other organs – in 19 patients. The frequency of detection of distant liver metastases, both independently and in combination with metastases to other organs, as using ultrasound (89.1%), MSCTA (92.0%) and MRI (89.3%) does not significantly differ (p=0.801).The results of the study described above are the basis for the development of an algorithm for the diagnosis of distant metastatases of CRC. A multifactorial logistic analysis with a step-by-step exclusion procedure was performed to assess the effectiveness of the studied indicators in determining distant CRC metastases. The resulting model included 3 indicators: changes in the GBT, an increase in the concentration of REA, an increase in the concentration of CA19-9, and the determination of metastases during MRI examination. The results of the analysis are presented in table 8.Table 8. The results of a multifactorial logistic analysis to assess the determination of primary distant metastases of CRC
 |
| |
|
Thus, the minimum mandatory set of diagnostic measures to determine the primary distant metastases of CRC is the analysis of the results of GBT, elevated levels of REA and CA19-9, the presence of metatstases according to the results of MRI.
4. Conclusions
1. The combination of clinical manifestations of the disease correlates with the stage of the disease (p<0.001) and the presence of distant metastases (p<0.001). The 5-year overall survival rate in the group of patients without clinical symptoms (63.9±6.0%) is slightly higher (p=0.053) than in the group of patients with clinical manifestation of the disease (52.6±3.7%). The median overall survival was 81.0 months (95% CI 53.6-108.4) in the group of patients without clinical manifestations and 70.0 months (95% CI 52.8-87.2%) in the group of patients with clinical manifestations.2. Changes in GBT and BBT were noted significantly (p<0.001) more often in the group of patients with distant metastases (76.7%) than among patients without them (40.3%). At the same time, in the group of patients without distant metastases, changes in ESR, such as monocytosis and eosinophelia, were significantly more frequent than among patients with distant metastases. Among patients with primary distant metastases, an increase in the concentration of CA19-9 and REA was significantly more frequent than in the group of patients without distant metastases (p<0.001). 3. To identify primary distant metastases of CRC, MRI examination has the highest indices of DSe (79.6%), DSp (93.3%), DE (87.7%), PSPR (90.7%) and PSR (84.8%) compared with ultrasound diagnostics and MSCT.4. An algorithm for the diagnosis of primary distant CRC metastases has been developed, which includes a mandatory assessment of GBT, CA19-9 and REA levels, and an MRI examination. The obtained predictive model is characterized by a high level of statistical significance (p<0.001).
References
| [1] | Arnold M, Sierra MS, Laversanne M, et al. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017; 66(4): 683. doi: 10.1136/gutjnl-2015- 310912. |
| [2] | Brenner DR, Heer E, Sutherland RL, et al. National Trends in Colorectal Cancer Incidence Among Older and Younger Adults in Canada. JAMA Network Open 2019; 2(7): e198090-e90. |
| [3] | Cancer i sifrror 2018: Socialstyrelsen and Cancerfonden, 2018; Siegel RL, Miller KD, Goding Sauer A, et al. Colorectal cancer statistics, 2020. CA: a cancer journal for clinicians 2020; 70(3): 145-64. |
| [4] | GLOBOCAN 2020 [Available from: https://gco.iarc.fr/ accessed 2021-06-07 2021. |
| [5] | Liang PS, Chen T-Y, Giovannucci E. Cigarette smoking and colorectal cancer incidence and mortality: Systematic review and meta-analysis. International Journal of Cancer 2009; 124(10): 2406-15. |
| [6] | Meester RGS, Mannalithara A, Lansdorp-Vogelaar I, et al. Trends in Incidence and Stage at Diagnosis of Colorectal Cancer in Adults Aged 40 Through 49 Years, 1975- 2015. Jama 2019; 321(19): 1933-34. |
| [7] | Research WCRFAIoC. Diet, Nutrition, Pshycial Activity and Cancer: a Global Perspecitve. Continous Update, 2018. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML