Ziyaeva E. R.1, Ruzieva N. H.2
1Andijan State Medical Institute, Andijan, Uzbekistan
2Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Chronic salpingo-oophoritis (CSO) is a prevalent gynecological condition affecting 60–65% of cases, often leading to chronic pelvic pain syndrome (CPPS), infertility, and ectopic pregnancies. Despite advances in diagnostic and therapeutic measures, CSO persists as a major medical and social issue due to its frequent relapses, treatment challenges, and severe complications such as adhesions, tubo-ovarian abscesses, and immune system dysfunction. The disease significantly impacts reproductive health, mental well-being, and quality of life, highlighting the need for comprehensive strategies to address its medical and societal implications.
Keywords:
Chronic Salpingo- Oophoritis (CSO), Chronic Pelvic Pain Syndrome (CPPS), Fertility Issues, Infertility, Ectopic Pregnancy, Gynecological Pathologies, Reproductive Health, Immunopathological Response
Cite this paper: Ziyaeva E. R., Ruzieva N. H., Complex Therapy for Women with Chronic Pelvic Pain Syndrome, American Journal of Medicine and Medical Sciences, Vol. 14 No. 11, 2024, pp. 3017-3027. doi: 10.5923/j.ajmms.20241411.76.
1. Introduction
Today, diagnostic and therapeutic approaches to pelvic inflammatory disease (PID) are well-regulated. The state of women’s health has promoted the development of measures at both the national and global levels aimed at preserving reproductive health, a key priority of the “National Strategy” for women’s well-being. The relevance of PID in the new millennium remains high and continues to be actively discussed in both domestic and international literature [16]. Chronic salpingo-oophoritis (CSO) or adnexitis is one of the most common diagnoses in gynecological practice, accounting for approximately 60-65% of all gynecological pathologies. [12]. In some cases, the duration of treatment and monitoring for CSO symptoms persist throughout a women’s fertile years [15]. Around 70% of patients with CSO undergo treatment multiple times a year, and approximately 40% report dissatisfaction with the effectiveness of their treatment on an annual basis [5]. CSO has significantly negative impact on fertility, with some patients experiencing no improvement after treatment. CSO is the cause of chronic pelvic pain syndrome (CPPS) in one out of every three or four patients, and in about 5% of cases, it leads to ectopic pregnancy. Approximately 40% of women with CSO may become infertile [8,16]. CPPS in these patients contributes to mental and physical health issues, sexual dysfunction, a higher rate of divorce, and frequent temporary or permanent disability [10,17,19].Chronic salpingo-oophoritis (CSO) often presents a prolonged course characterized frequent relapses and exacerbation, which can ultimately lead to infertility. Over time, the chronic nature of CSO contributes to the development of chronic pelvic pain syndrome (CPPS) as adhesions from around the uterine adnexa and progressively spread throughout the pelvic. This progression frequently results in purulent complications, including pyosalpinx, pyovar, and tubo-ovarian abscesses, among other [10].Chronic salpingo-oophoritis (CSO) is marked by pronounced sclerotic, adhesive, fibrotic, and degenerative changes in many structures and adnexa of the uterus, leading to both morphological and functional abnormalities. These pathological changes often result in discrepancies between clinical symptoms and findings from gynecological or instrumental examinations, as well as with morphological indicators observed in the fallopian tubes, ovaries, and surrounding tissues [6]. This inconsistency is frequently attributed to the diversity and changing virulence of the lower genital tract microflora, which influences both the immune competency of the body and the overall efficacy of treatment [14].The chronic nature of salpingo-oophoritis (CSO) is driven by an immunopathological response influenced by the baseline functionality of the immune system, including factors such as immunoglobulin secretion, cytokine release, formation of pathogenic immune complex, and expression of adhesive molecules [1,2].Infertility is the most common complication associated with chronic salpingo-oophoritis, affecting over 35% of patients, miscarriages, endometriosis, as well as benign and malignant tumors of the female reproductive system [9,17].In summary, an analysis of current scientific and clinical literature suggest that CSO represents not only a medical issues but also a significant social concern, underscoring its status as one of the most urgent medical and social challenges in modern gynecology. The study aimed - to investigate the characteristic changes in levels of the pain-associated peptide substance P (SP) and various cytokines in the blood of women with chronic salpingo-oophoritis complicated by pain syndrome, and to develop an integrated therapeutic approach.Determine the frequency and typological characteristics of chronic- oophoritis (CSO) based on disease duration and exacerbation patterns; Examine alterations in the levels of pain-associated peptide substance P(SP) and blood cytokines in women with CSO;Develop and assess the effectiveness of a comprehensive therapeutic approach for managing CSO exacerbations. The study analyzed diagnostic and treatment outcomes for 136 patients with chronic salpingo-oophoritis (CSO), with and without chronic pelvic pain syndrome (CPPS), who received care at the clinical base of the Department of Obstetrics and Gynecology No. 1 (Head: Professor Asrankulova D.B., Doctor of Medical Sciences) at the Andijan branch of the Republican Specialized Scientific and Practical Medical Center for Mother and Child Health (Director: Nasretdinova D.B., Candidate of Medical Sciences) from 2018 to 2023.
2. Material and Methods of Research
Clinical data were collected at the Andijan State Medical Institute (Rector: Professor Madazimov M.M., Doctor of Medical Sciences), at the clinical base of the Department of Obstetrics and Gynecology No. 1 (Head: Professor Asrankulova D.B., Doctor of Medical Sciences), and at the Andijan branch of the Republican Specialized Scientific and Practical Medical Center for Mother and Child Health (Director: Ph.D. Nasretdinova D.B.). The study was conducted in the gynecological department of this clinical base, previously known as the Andijan Regional Perinatal Center, between 2018 and 2023. A total of 136 women of reproductive age (21–35 years) were observed, with an average age of 27.8 ± 2.89 years.Between 2018 and 2023, 136 women of reproductive age (21–35 years), with chronic pelvic pain syndrome (CPPS) and chronic salpingo-oophoritis (CSO), were examined at the gynecological department. The average age of the patients was 27.8 ± 2.89 years. The main group (MG) consisted of 54 patients with chronic salpingo-oophoritis, who had a history of 5-10 years and disturbances in the biocenosis of the female reproductive system. The participants' ages ranged from 21 to 35 years, with an average age of 28.2 ± 1.34 years.The comparison group (CG) consisted of 52 women with a history of chronic salpingo-oophoritis (CSO) lasting up to 10 years, without chronic pelvic pain syndrome (CPPS) or disturbances in the biocenosis of the female reproductive system. The participants' ages ranged from 23 to 35 years, with an average age of 28.8 ± 1.17 years.The control group (CG) included 30 women with CSO lasting up to 5 years, also without CPPS, aged 23 to 35 years, with an average age of 28.6 ± 1.25 years.In accordance with the study design, all patients were examined upon admission, again 2 weeks after completing the course of corrective treatment, and 3 months following the treatment.Corrective therapy methods for patients with chronic salpingo-oophoritis The patients in the main group were further divided into two subgroups (A and B) based on the type of corrective therapy they received. Subgroup A received standard corrective therapy, which included the following medications and interventions:All patients experiencing exacerbations of chronic salpingo-oophoritis (CSO) were prescribed standard treatment, consisting of: Antibacterial and anti-infective agents: Fluoroquinolones (e.g., ofloxacin 400 mg twice daily for 10-14 days), azalides (e.g, azithromycin 500 mg once daily for 6 days), and nitroimidazoles (e.g., metronidazole 500 mg intravenously 2-3 times daily, followed by 500 mg orally three times daily for 5-10 days), selected based on identified infectious agents and antibiogram results. Immunomodulators: Cycloferon (12.5% solution, 2ml intramuscular once daily on days 3,5,7,9,11,13,17, and 21 of treatment) or Viferon (rectally, 10 suppositories). Vitamin therapy: as part of general supportive care. Drugs to improve microcirculation aimed at enhancing blood flow and tissue oxygenation. Proteolytic enzymes to assist in the breakdown of fibrin and support tissue healing. Physiotherapy targeted to reduce inflammation and improve circulation [11]. Patients of subgroups B of both groups, in addition to the standard treatment of CSR of subgroups A, received Wobenzym, Saccharomycetes Boulardi (bioterol), a complex of B vitamins and underwent lifestyle modification (normalization of sleep, increased mobility and an elimination diet with the exclusion of inflammatory triggers - fruits, dairy products, sweets and wheat flour). Statistical processing of the research results was carried out using variation statistics using Microsoft Office Excel-2019 with calculation of the mean and mean arithmetic error using the method of moments (M±m), standard deviation (σ). To assess the statistical significance of the obtained measurements, Student's t-test was used to evaluate differences between groups, with the degree of confidence (P) calculated for data that followed a normal distribution. Differences were considered significant at a 95% confidence interval (P ≤ 0.05) [4,7,13]. Statistical significance was categorized into four levels: high (P < 0.001), medium (P < 0.01), low (marginal) (P < 0.05), and insignificant (P > 0.05) [4,7,13]. Additionally, correlation strengths were classified as follows: strong correlation (r > 0.7), moderate correlation (r between 0.3 and 0.7), and weak correlation (r < 0.3) [4,7,13].
3. Research Results
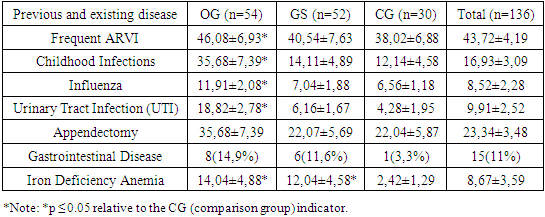
Among the patients in our study, the average age at the onset of sexual activity was 19.75±2.68 years, 72 (67.92%) patient were married, 34 (32.08%) –were single and had 1-2 sexual partners.We observed a high frequency of general infectious pathologies among the patients, including ARVI (43.72±4.19%), childhood infectious disease (16.93±3.09%), viral pathologies caused by influenza and parainfluenza viruses (8.52±2.28%), pyelonephritis (9.91±2.52%). In the OG, childhood infectious diseases were detected in a significantly higher proportion of patients (35.68±7.39%) compared to the GS (14.11±4.89%) and CG (12.14±4.58%), although the differences were not statistically significant (p > 0.05). A similar trend was observed for pyelonephritis, which was present in 18.82±2.78% of the OG, 6.16±1.67% of the GS, and 4.28±1.95% of the CG, with statistically significant differences (p > 0.05). We observed a relatively high incidence of appendicitis (23.34±3.48%) among the study population, which may serve as an auxiliary factor in the development of chronic salpingo-oophoritis (CSO), given its anatomical proximity and the almost inevitable postoperative adhesive process. Appendectomy was performed in 22.04±5.87% of the CG, 22.07±5.69% of the GS patients, and 35.68±7.39% of the cases in the OG, with the incidence in the OG being nearly one and a half times higher, though the differences were not statistically significant (p > 0.05).Table 1. Extragenital Diseases in Patients with Chronic Salpingo-Oophoritis (CSO) (M±m%)
 |
| |
|
Various gastrointestinal pathologies, known contributors to the development of vaginal dysbiosis and facilitators of opportunistic flora growth and CVT recurrence, were identified 11.89±2.68% of participants. Specifically, chronic gastritis was diagnosed in 4.93±1.78% duodenal ulcer (DU) in 2.12±1.18%, chronic cholecystitis in 2.09±1.19%, and chronic pancreatitis 1.42±0.89%. Moderate iron deficiency anemia was observed in 14.04±4.88% of the MG, 12.04±4.58% of the GS, and only 2.42±1.29% in the CG—a statistically significant difference, showing markedly lower rates in the control group (р<0.05). Notably, none of the patients in the study exhibited active infections such as ureaplasmosis, mycoplasmosis, chlamydia, or herpes simplex virus types I and II at the time of examination, nor were any positive for HIV, HBsAg, HCV, toxoplasmosis, or rubella.Clinic visits were predominantly due to exacerbations of CSU, accounting for 91.58±4.79% of cases. In 68.91±4.56% of these cases, CSU presented without an acute onset and was classified as “primarily chronic.” Additionally, 16.22±3.08% of patients were diagnosed with nonspecific vulvovaginitis, while 15.52±3.02% were identified with an infectious disease of the cervix.Additionally, 10.62±2.58% of the patients with CSR had undergone various surgical interventions on reproductive organs. Among the patients studied, 26.72±3.69% showed evidence of specific urogenital infections, with the most common being candidiasis (44.72±9.13%), followed by mycoplasma (23.73±7.84%) and chlamydial infections (21.11±7.43%). These infections are likely due to a suppressed immune response in the host.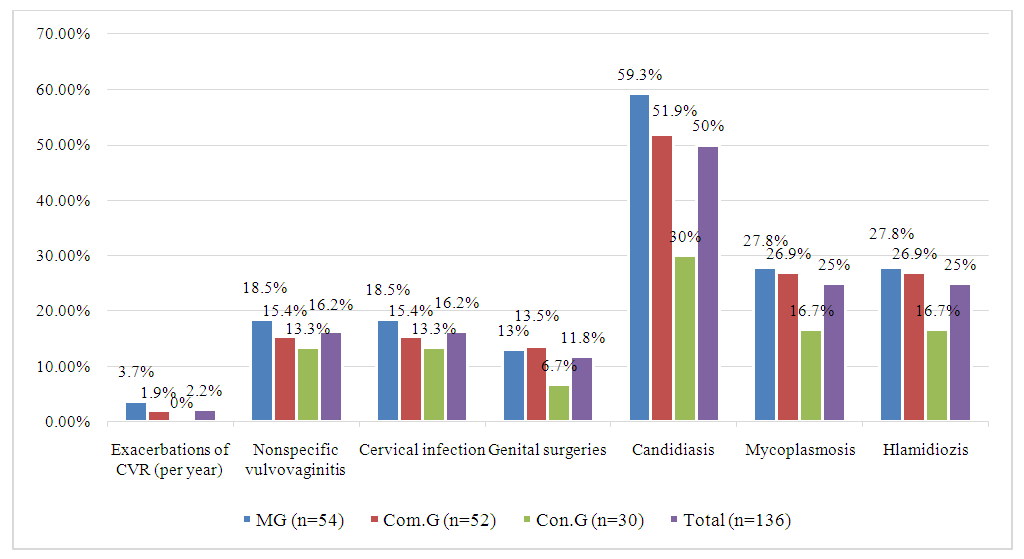 | Figure 1. Genital Pathologies Observed in Patients with CSR |
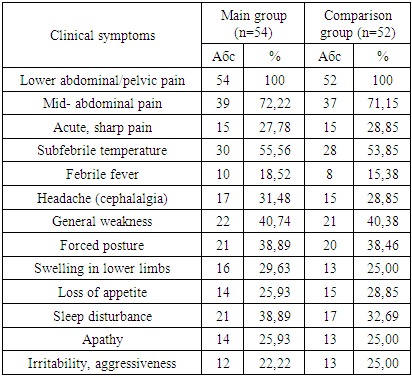
Among the studied women with CSR, 54.43±4.32% reported a history of medical abortion, while 42.77±4.23% had experienced childbirth.Exacerbations of CSR were commonly associated with the onset of menstruation in 16.94±3.13% of cases, while 3.54±1.72% of patients attributed exacerbations to IUD insertion or ARVI, and 43±0.92% linked exacerbations to medical abortion. A gradual onset of CSR exacerbation, progressing over approximately 4-5 days, was observed in 70.75±4.23% of participants. Clinically, all patients experienced pain in the lower abdomen and pelvic area during exacerbation of CSO; of these, 71.70±3.77% described the pain as moderately aching, while 28.30±1.37% reported acute pain. Fever was noted in 71.70±3.77% of patients, with 54.72±4.72% of these cases presenting as low-grade fever.Table 2. Clinical symptoms of patients in the study groups before the treatment complex
 |
| |
|
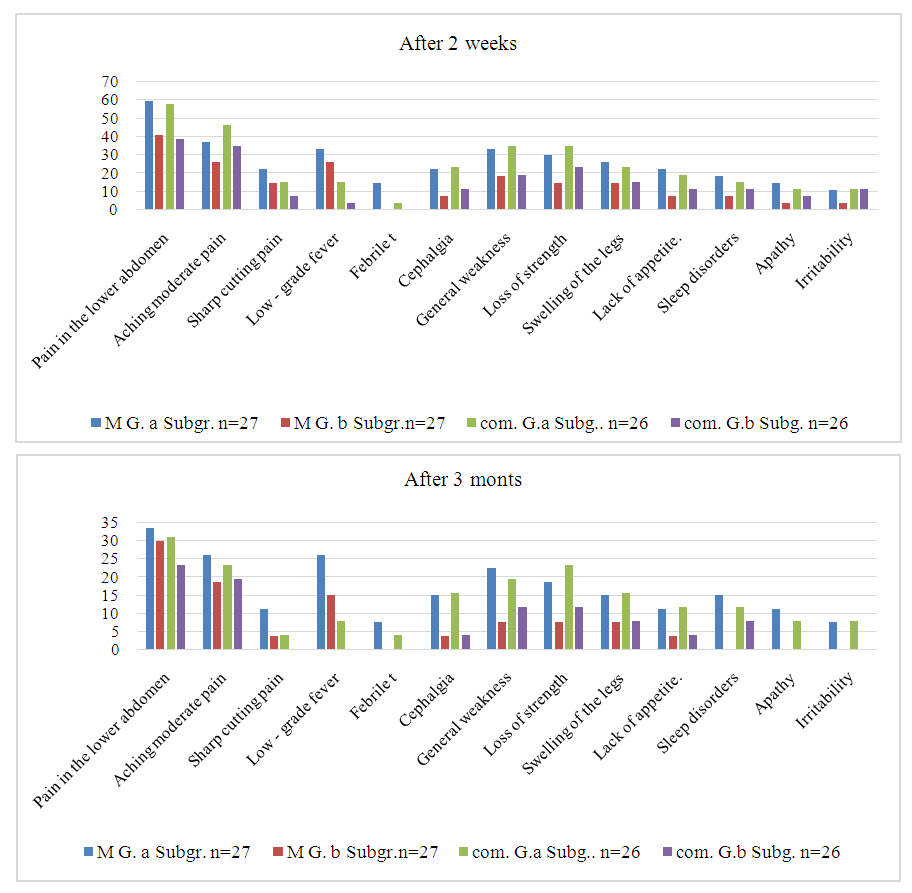 | Figure 2. Dynamics of clinical symptoms of patients in the study groups under the influence of the treatment complex |
After analyzing the results of subjective assessments from our patients, we concluded that chronic salpingo- oophoritis (CSO) should be regarded not only as a medical issue but also as a social one, as it significantly impacts the psychological well-being of patients. The condition notably increases abxiety and depression, as measured by the Hospital Anxiety and Depression Scale (HADS), reaching subclinical levels (р ≤ 0,05). Furthermore, both personal and reactive anxiety, as assessed by the Spielberger State- Trait Anxiety Inventory (STAI), were significantly higher in CSO patients (р ≤ 0,05). The subjective assessments of patients in the main (OG) and comparison (GS) groups, both during exacerbation of chronic pelvic syndrome (CPPS) and during non-exacerbation periods, were significantly different from those of the control group (р ≤ 0,05). Additionally, the perceived severity of their condition during exacerbations was significantly greater in the OG and GS compared to the CG, underscoring the substantial impact of CSO on patient’s quality of life and psychological health (р ≤ 0,05).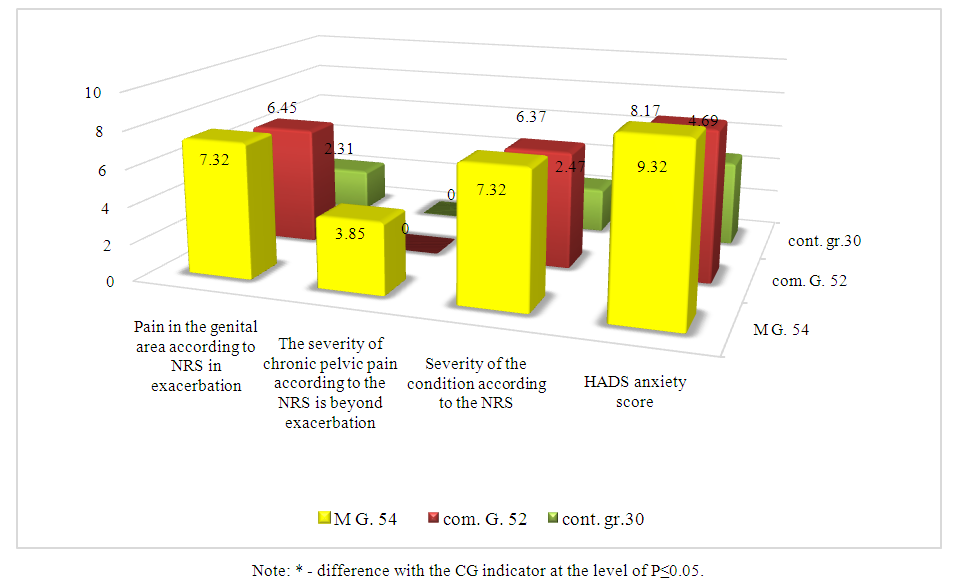 | Figure 3. Subjective assessment of their condition by patients with CSR, as measured by scale scores and questionnaires (M±m) |
General clinical and biochemical analyses of morning urine for participants in all study groups showed no notable differences from the control, group or references norms, so these results were not included in further analysis. Gynecological exams identified ovarian thickening and infiltration in 43.40±4.32% of patients, accompanied by moderate or severe pain on palpation, and a sense of heaviness in the adnexal area in 56.60±6.37%of patients. Blood test results indicated minimal response to pelvic inflammation, suggesting that the inflammation was localized and mild. Moderate leukocytosis was observed in 64.15±4.72% of patients, with a leftward leukocyte shift in 44.34±4.35%. Biochemical blood parameters for CSO patients remained within normal limits. Ultrasound findings showed ovarian enlargement in 20.75±3.45% of patients, thickened ampullae in the fallopian tubes in 26.42±3.77%, and hydrosalpinx in 13.21±2.83% of cases. Additionally, 30.19±3.77% of patients showed hypoechogenic ovaries, and 11,32±3,77% had a thickened ovarian capsule. We categorized all patients in both groups based on the type of CSO exacerbation at the initial treatment, following established criteria, into slow exacerbation and intense exacerbation types [3,11].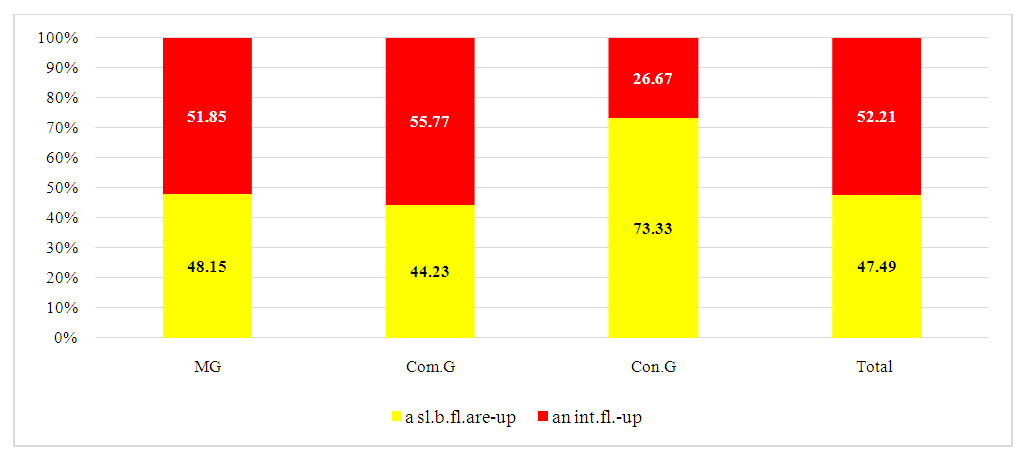 | Figure 4. Distribution of Patients in Study Groups by Type of CSO Exacerbation (%) |
The minimum number of exacerbation per year observed among patients was 3, with an average frequency of 85±0.61 episodes annually. Intense exacerbation-type SCO was more frequently associated with nonspecific vulvovaginitis, occurring in 35.73±7.42% of cases, while in the OG group, this condition was present in 18.43±5.42%, and in the GS group, in 16.12±5.23%. this represents an approximately twofold increase, a different that approach statistical significance (р > 0,05).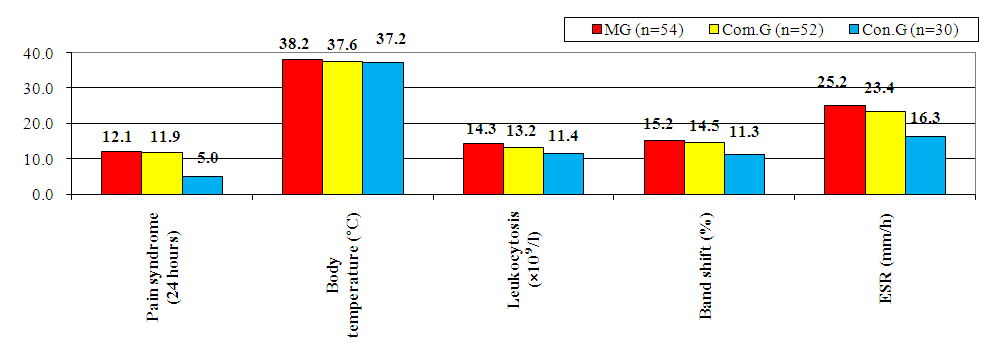 | Figure 5. Clinical and Laboratory Manifestations of Chronic Salpingo-Oophoritis (CSR) |
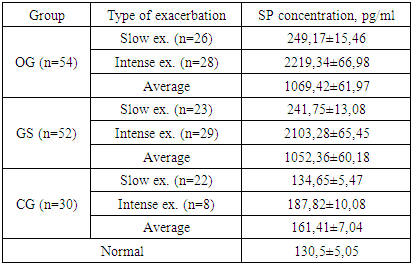
To investigate the nature of chronic pelvic pain (CPP) in our patients with CSO, particularly those intense exacerbation CSO, we assessed serum concentrations of Substance P (SP). SP is well-documented to correlate reliably with the severity of pain experienced by patients, though it does not show a direct relationship with the degree of inflammation. This analysis aimed to clarify the pain mechanisms in CSO, distinguishing pain sensitivity from inflammatory markers, and further understanding the complex presentation of CPP in these patients. Table 3. Serum SP levels in patients of the study groups (M±m)
 |
| |
|
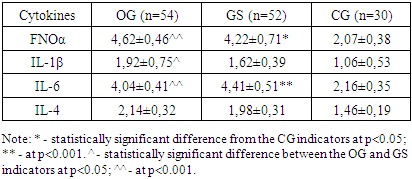
In the subgroups with slow-onset exacerbation of chronic salpingo-oophoritis (CSO), serum Substance P (SP) levels reliably reflected not only pain severity but also associated vasodilation and edema. A serum SP concentration threshold of 2000 pg/ml was identified as diagnostically valuable, with the method’s sensitivity reaching 98% and specificity 88% from this point onward, indicating high predictive accuracy before the onset of neurogenic pain. In patients from both the OG and GS groups experiencing severe pain during exacerbations with SP levels exceeding 2000 pg/ml, pain intensity was disproportionately high relative to the inflammation severity in the uterine appendages. This phenomenon contributes to the formation of chronic pelvic pain syndrome (CPPS) even with minimal CSO exacerbations in the women studied in the OG group. Given the varied clinical presentation of CSR exacerbations, we also investigated the immune status, focusing on the pro- and anti-inflammatory cytokine profile, including FNOα, IL-1β, IL-4, and IL-6. Cytokine profile indicators, however, did not show statistically significant deviations from reference norms (p>0.05), suggesting that inflammation alone may not fully explain the pain intensity in these cases.Table 4. Serum Concentrations of FNOα, IL-1β, IL-6, and IL-4 in Patients with Exacerbation of Chronic Salpingo-Oophoritis (CSO) (pg/ml)
 |
| |
|
The determination of serum concentration of FNOα and IL-6 in patients with intense exacerbation CSO revealed a two-fold increase in these markers compared to both references values (P<0.001) and levels observed in slow exacerbation CSO (p<0.001), indicating that proinflammatory cytokines increase due to prolonged, intense inflammation. In contrast, in slow exacerbation CSO, the serum levels of these cytokines did not differ significantly from those in the control group (CG) (p > 0.05), suggesting that the intensity of inflammation directly correlates with clinical symptoms, except for the severity of pain. Among patients in the GS group, IL-4 concentrations were found to be two times lower than in the CG (p < 0.05), while FNOα levels were two times higher than those of the CG (p < 0.05), indicating that pro-inflammatory cytokines surpass anti-inflammatory ones. Although the levels of IL-1β and IL-6 were lower than in the CG, these differences were not statistically significant (p > 0.05).Thus, the severity of exacerbation of CSO is determined by genital and extragenital pathology, colonization resistance of the mucous membrane of the vagina and genital cervix, as well as the characteristics of the microbiocenosis of the reproductive tract, the level of SP, structural and functional changes in the uterine appendages and the level of imbalance of neuroendocrine regulation. The dynamics of the clinical condition in the studied patients provide insight into the effectiveness of both the standard and the proposed comprehensive treatment approaches for CSO with CPPS, allowing for a comparative evaluation of their outcomes [2,4,9,18].We observed the greatest reduction in clinical symptoms and complaints in the B subgroups of both groups, particularly in the GS, which we attribute to the shorter duration of CSO in this subgroup compared to the OG. In the GS B subgroup, symptoms such as acute cutting pain in the lower abdomen, temperature fluctuations, irritability, aggression, and apathy were completely alleviated. The frequency of pain decreased by more than fourfold, from 100% before treatment to 23.08% after 3 months. Additionally, the prevalence of moderate, aching pain dropped from 71.15% to 19.23%, a reduction of more than 3.5 times. Other associated clinical symptoms also showed significant improvement in this subgroup. A similar trend was observed in the B subgroup of the OG, with changes in clinical symptoms still notable, but less pronounced. We attribute this to the longer duration of CSO and the presence of CPPS, which may have contributed to a more persistent clinical picture that is more challenging to address within the study period. Although positive changes were also observed in both groups receiving standard therapy, the improvement in clinical symptoms was somewhat slower than in the groups receiving the complex treatment. In a comparative analysis of treatment effectiveness using the pain intensity rating scales, the Hospital Anxiety and Depression Scale (HADS), and the Spielberger STAI test, patients assessed the severity of pain during an exacerbation of CSO, their general somatic condition, the severity of CPP exacerbation, and levels of anxiety, depression, personal anxiety, and reactive anxiety both two weeks and three months after treatment. These assessments also considered the number of exacerbations during the follow-up period. The frequency of pain decreased more than fourfold after three months, from 100% before treatment to 23.08%. The frequency of moderate aching pain reduced from 71.15% to 19.23%, a reduction of more than 3.5 times. Additionally, concomitant clinical symptoms showed significant improvement and were most notably alleviated in this subgroup. An identical trend was observed in the B subgroup of the OH group; while the dynamics of improvement were similar, they were somewhat less pronounced. This difference is likely due to the longer duration of CSO and the presence of CPPS, which is a persistent factor that is harder to resolve during the study. Both subgroups, however, showed positive dynamics, with the rate of improvement in clinical symptoms in the standard therapy group lagging slightly behind that of the complex treatment group.In the comparative analysis of therapy effectiveness using the pain intensity rating scales, the Hospital Anxiety and Depression Scale (HADS), and the Spielberger STAI test, patients assessed the severity of pain during an exacerbation of CSP, their general somatic condition, the severity of CPP exacerbation, and levels of anxiety, depression, personal anxiety, and reactive anxiety at two weeks and three months after treatment, accounting for the number of exacerbations during the follow-up period (Fig. 6).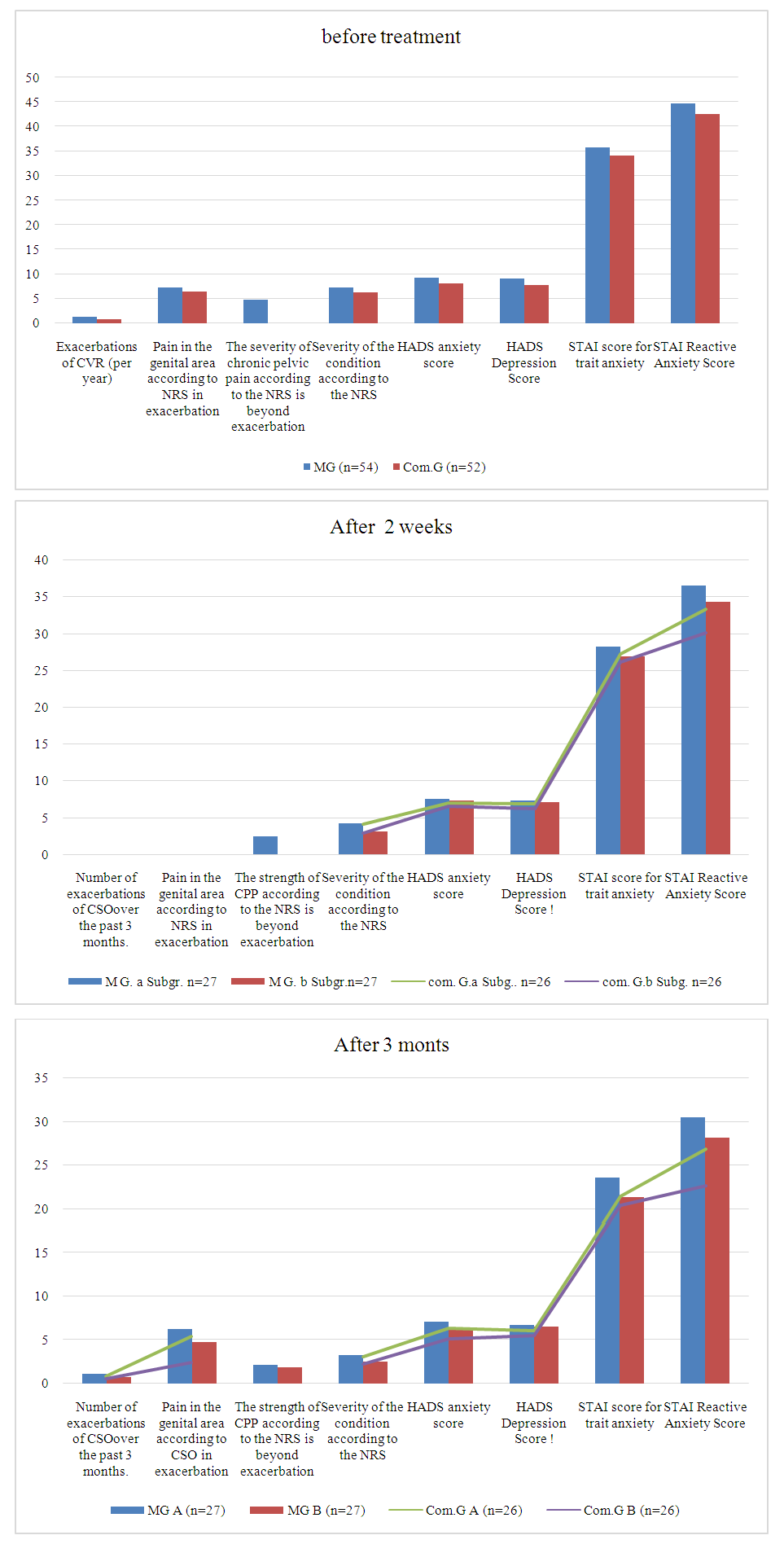 | Figure 6. Comparative analysis of the effectiveness of corrective therapy in patients of the study groups |
The comparative analysis of the results from the scales reveals dynamics in the effectiveness of the therapy that align closely with the clinical symptom changes. We observed the maximum effectiveness in the GS subgroup B, which is naturally attributed to the complexity of the treatment and the shorter duration of the pathology. The number of exacerbations of CSO in the B subgroup GS was 0.52±0.13 cases during the 3-month follow-up period. In comparison, the A subgroup OG had 1.08±0.12 cases, the B subgroup OG had 0.79±0.14 cases, and the GS subgroup had 0.82±0.15 cases (P ≤ 0.05).Pain in the genital area, as measured by the pain intensity rating scales, also decreased statistically significantly 3 months after treatment in the GS subgroup B compared to all other subgroups (P ≤ 0.05). Furthermore, the severity of the general condition, as subjectively assessed by patients 3 months post-treatment, showed a statistically significant difference in the GS B subgroup when compared to the A subgroups of both groups (P ≤ 0.05).Three months after treatment, the GS subgroup showed a statistically significant decrease in the total score on the HADS anxiety scale compared to all other subgroups (P ≤ 0.05). Additionally, there was a significant reduction in the total score on the STAI reactive anxiety questionnaire for the GS subgroup relative to both subgroups of the other group (P ≤ 0.05).It is important to note that the proposed complex therapy for CSR in the B subgroups of both groups was more effective compared to the standard therapy in the A subgroups, although not all indicators showed statistically significant differences.A comparative analysis of peripheral blood demonstrated that by the end of treatment, all indicators had normalized in the majority of patients, both in terms of cell counts and leukocyte formula. No significant changes were observed, and all values remained within age-appropriate reference ranges. However, after 3 months, a few patients with an exacerbation of CSO showed mild leukocytosis (up to 12 × 10⁹/l) and a minor shift to the left in the leukocyte formula, although these findings were not statistically significant. Given the absence of significant deviations from baseline levels, we refrained from drawing conclusions regarding the peripheral blood analysis.We did not conduct a biochemical blood test after treatment, as the pre-treatment values in the study groups were consistent with those in the CG and the established reference values for age and gender.Ultrasound examinations of the uterus and appendages revealed a trend toward a decrease in ovarian size and normalization in 20.75% of patients who had ovarian enlargement prior to treatment. Similarly, the size of the fallopian tube ampoules decreased in the majority (26.42%) of patients who had enlarged ampoules before treatment. Additionally, echogenicity and ovarian capsule thickness normalized in patients with CSO and appendage pathology, although this was not observed in all 30.2% of patients across both subgroups. Ultrasound symptoms were completely resolved in the B subgroup of the GS and in the majority of the B subgroup of the OG [3,5,19].We assessed the effectiveness of the treatment based on the dynamics of serum SP concentration.Table 5. Dynamics of SP level before and after therapy (M±m)
 |
| |
|
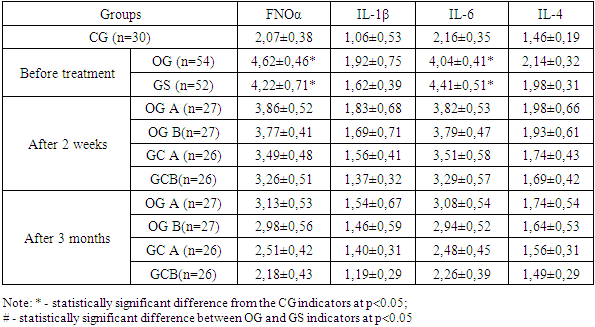
As follows from the presented data, SP concentrations after treatment decreased in both subgroups, this was especially clearly stated 3 months after treatment (P ≤ 0.05). We recorded a greater tendency towards normalization in the B subgroups, and in GS B it was maximally manifested.Based on these data, we can make a preliminary conclusion about the better effect of complex therapy on the body of the studied patients, which confirms its greater effectiveness.In the patients studied with CSO, we assessed the dynamics of spontaneous and induced in vitro serum levels of various laboratory parameters, including FNOα, IL-1β, IL-6, and IL-4. The observed imbalance and suppression of the humoral immune response appear to be related to the duration of the infectious pathology and the necessity for repeated courses of complex therapy.At the same time, it is worth noting a better normalization of the levels of pro-inflammatory cytokines in patients of the B subgroups, particularly in the GS B group.Table 6. Dynamics of serum cytokines in the studied patients with CSO during observation (M±m)
 |
| |
|
Our research led to several important conclusions:The results of the clinical and social examination of patients with CSO suggest that complex treatment is more effective, especially when the duration of CSO is less than 5 years. The therapy demonstrated its highest effectiveness in this group, regardless of the pathology’s duration.A comparative analysis of peripheral blood showed that by the end of treatment, most patients had normalized cell counts and leukocyte formula, with no significant changes, and all values were within age-specific norms. After 3 months, a few patients who had an exacerbation of CSO showed mild leukocytosis (up to 12 × 10⁹/l) and a slight, statistically insignificant shift to the left in the leukocyte formula. These changes were not statistically significant, and thus, no conclusions were drawn regarding peripheral blood analysis.We did not perform biochemical blood tests post-treatment, as pre-treatment levels in the study groups were consistent with the control group and age-specific reference values.Ultrasound examination of the uterus and appendages revealed a trend toward normalization. In 20.75% of patients, the ovaries shrank and returned to normal size, and in 26.42% of patients, the size of the ampoules of the fallopian tubes decreased. Subjectively, echogenicity and ovarian capsule thickness normalized in patients with CSO and appendage pathologies, though not in all 30.2% of patients in both subgroups. However, ultrasound findings were completely normalized in the B subgroup GS and most of the B subgroup OG.
4. Conclusions
The clinical, anamnestic, and instrumental-laboratory studies of the triggering and pathogenetic mechanisms underlying the formation and recurrence of CSO provide valuable insights into the nature of this pathology. Our findings indicate that disturbances in vaginal microbiocenosis and the overgrowth of opportunistic microorganisms contribute to the development of a focal inflammatory process and the clinical manifestation of CSO. This is influenced by both genital and extragenital pathologies, as well as the colonization resistance of the mucous membranes, the dynamics of vaginal and cervical microbiocenosis, excessive production of substance P (SP), and neuroendocrine imbalances.Upon analyzing the results of the subjective assessment of patients’ conditions, we concluded that CSO should be regarded not only as a medical issue but also a social one. This pathology significantly impacts the psychological well-being of patients, leading to a notable increase in anxiety and depression, as measured by the Hospital Anxiety and Depression Scale (HADS), reaching subclinical levels (p ≤ 0.05). Additionally, both personal and reactive anxiety levels, as assessed by the Spielberger STAI test, were significantly elevated (p ≤ 0.05).The subjective assessments of patients in the OG and GS groups, both during exacerbations of CSO and CPPS and during periods without exacerbation, differed significantly from those of the control group (CG) (p ≤0.05). This was also reflected in the patients' assessment of the severity of their condition, with significant differences noted between the OG and GS groups and the CG (p ≤ 0.05).
References
| [1] | Agarkov N.M., Aksenov V.V., Ivanov A.V., Ivanov V.A., Kicha D.I., Subbotina T.I. Diagnostic significance and clustering of parameters of systemic humoral immunity in acute endometritis. Clinical laboratory diagnostics. 2017; 62 (12): 750-753. DOI: http://dx.doi.org/10.18821/0869-2084-2017-62-12-750-753. |
| [2] | Burova N. A. / Acute inflammatory diseases of the pelvic organs. etiology, pathogenesis, clinical picture, diagnosis, treatment and relapse prevention. 01/14/01 – Obstetrics and gynecology // Abstract of the dissertation for the degree of Doctor of Medical Sciences. Volgograd. 2020. |
| [3] | Kuznetsova, I.V. The role of oxidative stress and antioxidant protection in human reproduction // Obstetrics and gynecology. – 2016. – No. 3. – pp. 116–121. |
| [4] | Pestrikova T.Yu., Yurasov I.V., Yurasova E.A. A modern view on the clinical course, diagnosis and treatment of inflammatory diseases of the pelvic organs in women. // Russian Bulletin of Obstetrician-Gynecologist. 2015. - No. 4. – p. 23-28. |
| [5] | Savicheva A.M., Shipitsyna E.V., Vorobyova N.E. Infectious diseases of the vagina and modern approaches to their diagnosis and treatment // Obstetrics and gynecology. – 2016. – No. 2. – pp. 120–126. |
| [6] | Smirnova L.E., Umakhanova M.M., Torchinov A.M. Modern views on the adhesive process in the abdominal cavity in tubo-peritoneal infertility // Obstetrics and Gynecology – 2016. – No. 11. – pp. 148–152. |
| [7] | Shatunova E.P., Lineva O.I., Kaganova M.A. Immune profile and optimization of treatment of patients with chronic salpingoophoritis // Russian Bulletin of the Obstetrician-Gynecologist, 2016 - No6. – p. 83-88. |
| [8] | Shramko S.V., Zorina V.N., Bazhenova L.G. and others. Regulatory transport proteins and cytokines in the blood of patients with uterine diseases // Obstetrics and Gynecology. – 2016. – No. 5. – pp. 104–108. |
| [9] | Chen H, Wu Z, Wu Z, Huang Q. Proximal coil occlusion preceding distal sclerotherapy in patients with pelvic congestion syndrome: A multicenter, retrospective study. // J Vasc Surg Venous Lymphat Disord. 2023 - №11(1) – р. 149-155. doi: 10.1016/j.jvsv.2022.08.010. |
| [10] | Sutcliffe S, Newcomb C, Bradley CS, Clemens JQ, Erickson B. Associations Between Urological Chronic Pelvic Pain Syndrome Symptom Flares, Illness Impact, and Health Care Seeking Activity: Findings From the Multidisciplinary Approach to the Study of Chronic Pelvic Pain Symptom Patterns Study. // J Urol. 2023 - №11 – р. 39-55. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML