-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(11): 2998-3001
doi:10.5923/j.ajmms.20241411.71
Received: Nov. 2, 2024; Accepted: Nov. 21, 2024; Published: Nov. 27, 2024

Determination of Aetiological Factors Causing Upper Jaw Protrussions and Treatment Measures in Age-Dependent Cases
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFozilov Uktam Abdurazzokovich1, Badriddinov Bakhrom Bakhtiyorovich2
1DSc, Associate Professor, Department of Orthopedic Dentistry and Orthodontics, Bukhara State Medical Institute, Bukhara, Uzbekistan
2Assistant, Department of Orthopedic Dentistry and Orthodontics, Bukhara State Medical Institute, Bukhara, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study investigated the prevalence of maxillary protrusions and its etiological factors. In particular, the main causes of upper jaw protrusions are heredity, bad habits, functional disorders and aesthetic problems, and the need for early diagnosis of the factors affecting the disease and the mechanism of their development was emphasized. In a study of 184 children, different modern orthodontic appliances such as aligners, braces, and Twin-Block appliances were shown to be effective.
Keywords: Upper jaw protrusion, Orthodontics, Dentition system, Aligner, Bracket, Twin block, Aesthetics, Functional disorders, Genetic factors, Harmful habits
Cite this paper: Fozilov Uktam Abdurazzokovich, Badriddinov Bakhrom Bakhtiyorovich, Determination of Aetiological Factors Causing Upper Jaw Protrussions and Treatment Measures in Age-Dependent Cases, American Journal of Medicine and Medical Sciences, Vol. 14 No. 11, 2024, pp. 2998-3001. doi: 10.5923/j.ajmms.20241411.71.
Article Outline
1. Introduction
- Today, maxillary protrusions make up 36.8% of tooth-jaw system deformations according to the sources of scientific literature. Early diagnosis and effective treatment of these pathologies in the practice of orthodontic dentistry is one of the urgent problems awaiting a solution. In recent years, there has been an increase in the number of class II deformations and a decrease in class III deformations according to the Engel classification, which is related to the change in the chewing pressure load. E. N. Julev by foreign and local scientists, 2000; V.N. Trezubov, 2001; Mwakatobe D. Ambege, E. Yu. Nikolaeva, 2014; Nasimov E.E., 2019, highlights other forms of maxillary protrusions, that is, information on types of maxillary growth. Objective vision in the examination of maxillary protrusions is a complete analysis of cephalometric indicators, taking into account the growth component of the jaws [1]. According to the current research, deformations of the tooth-jaw system occur in the postnatal period in 25-80% of cases [2]. According to scientific sources, the incidence rate of tooth-jaw system deformations of adult patients is increasing among young children and adolescents [3]. The reason for this is that the improvement of the living conditions and the cultural level of the population indicate that the need to improve facial aesthetics is higher in older patients. Currently, significant progress is being made in improving the methods of treatment and rehabilitation of patients with upper jaw protrusions. The high level of these results is due to the increase in the quality of orthodontic care and the high level of early diagnosis and prevention of tooth-jaw system deformations in school and pre-school educational institutions. [5,6]. According to the knowledge of orthodontists all over the world, as a result of early diagnosis and effective treatment of deformations of the tooth-jaw system, restoration and normalization of the morphological and functional optimality of the tooth-jaw system, therefore, helps to increase the achieved results of their treatment.
2. Research Material and Method
- In 2021-2023, 184 children under the age of 18 with upper jaw protrusion were taken in the orthodontic department of the specialized children's dental center of Bukhara region. Children with upper jaw protrusions were examined objectively, subjectively and through a questionnaire. In our research, the patient children were divided into 3 groups.
3. Research Result
- Eliminating the etiological factors that cause protrusions of the upper jaw and studying the age-related condition can be caused by a number of etiological factors. In this study, they were divided into the following groups.Genetic predisposition. Heredity plays an important role in the development of high protrusions. Genetic studies show that children with this problem are often high in certain genes that affect the development of the upper and lower jaw. In 47% of our patients participating in our study, the origin of upper jaw protrusions as a result of genetic factors was studied.Harmful habits. 23% of our patients developed upper jaw protrusions as a result of harmful habits such as finger sucking, long-term use of pacifiers, or mouth breathing.Functional disorders. Atypical position of the tongue, nasal breathing disorders, improper swallowing and lack of proper chewing were observed in 11% of our study group patients.Early teething. Absence of teeth during permanent bite period was found in 6% of 14-17 year old patients.Disorders of the skull and brain. The forward position of the head causes excessive tension and contraction of the neck muscles, which causes the lower jaw to move back. Congenital muscular dystrophy also affects the development and function of muscles (cerebral palsy and Down syndrome) in children. In our research group, these patients were 0.6.Bone skeleton ratio. When the lower jaw is behind the upper jaw. This occurs as a result of insufficient growth of the lower jaw, excessive growth of the upper jaw, or a combination of both factors, which occurred in 14% of patients in the study.Teeth ratio. High front teeth bottom teeth significant level covers. This condition most of the time deep bite is also high of the teeth forward out to go take will come This condition in our study participating observed in 7% of our patients.Aesthetic problems. The face is unbalanced appearance can be extended high jaw and "sunk." gone " chin with is evaluated.Functional disorders. Cheynov and in speaking difficulty, mouth space to diseases inclination Sleep apnea and in sleep snoring. High jaw protrusions and bottom jaw distal in the situation very common signs. Jaws lack of development because of high breath of the ways volume decreases, this mouth through breath get, sleep during pathological circumstances observed.
|
 | Figure 1. Application of aligners in maxillary protrusion |
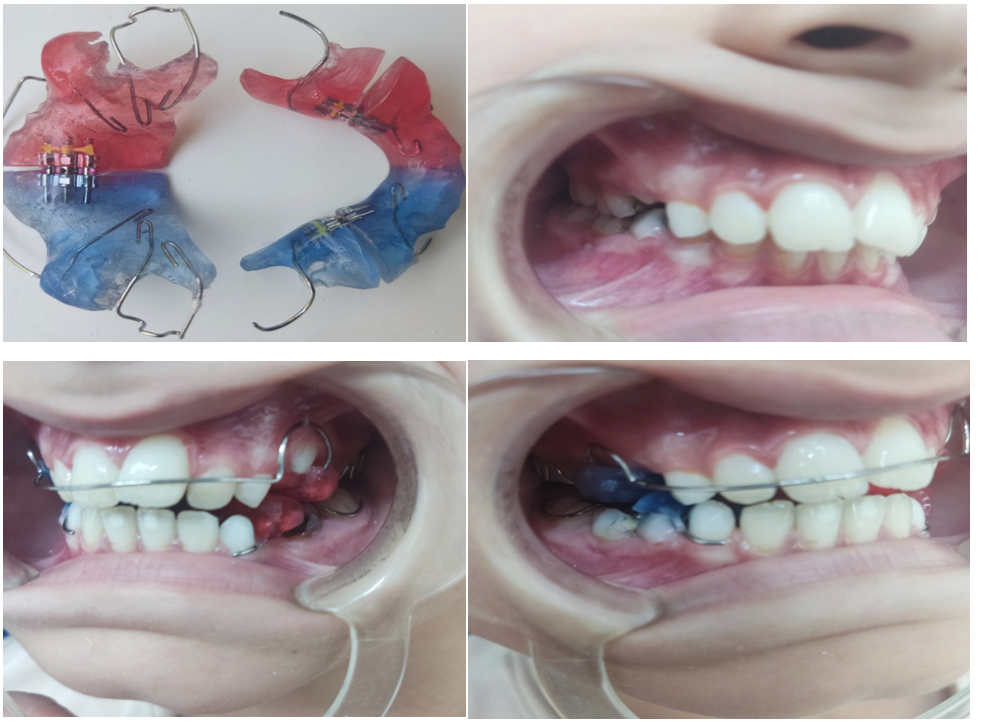 | Figure 2. Twin block hardware modification form used in comparison group patients |
 | Figure 3. Application of Bracket device in the treatment of maxillary protrusions during permanent pricus |
 | Figure 4. Combined use of Bracket Trainer V in patients with stage III sleep |
4. Research Results and Discussion
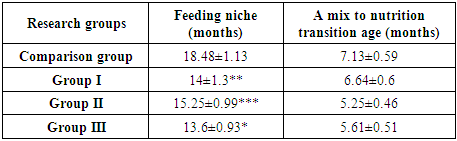
- When patients with upper jaw protrusion were examined through additional orthodontic examination methods, it was found that the incidence rate was higher in girls than in boys. Information on treatment methods, duration of treatment and the number of relapses in the three groups of patients being treated is presented in table 2.
|
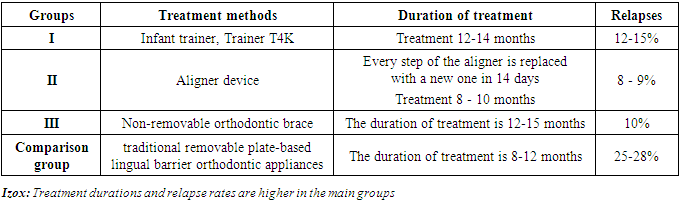
5. Conclusions
- Maxillary protrusions represent 36.8% of the total number of deformities in dentistry, and this problem needs early diagnosis and effective treatment. Factors such as harmful habits, genetic predisposition, early or incorrect eruption of teeth, and functional disorders cause this disease. Treatment methods between bracket, aligner and Twin block devices different forms used. Patients to his age looking selected orthodontic equipment different the results showed, including braces use treatment efficiency in raising important and aligners are aesthetically and functionally it is convenient. Treatment term and relapses indicators selected method depends respectively difference made, relapses while more of the teeth wrong output with depends was Treatment own in time execution and preventive measures organize to be done high jaw to the protrusion against in the struggle efficient measures as recommendation will be done.