-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(11): 2993-2997
doi:10.5923/j.ajmms.20241411.70
Received: Nov. 6, 2024; Accepted: Nov. 23, 2024; Published: Nov. 27, 2024

The Role of a Diet Composed of National Dishes in the Metaphylaxis of Calcium Oxalate Urolithiasis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLErmatov N. J.1, Gaybullaev A. A.2, Kuchkarov A. K.2
1Tashkent Medical Academy, Department of Hygiee of Children and Adolescents and Hygiene of Nutrition, Tashkent, Uzbekistan
2Center for the Development of Professional Qualifications of Medical Workers under the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article presents information on calcium excretion in daily urine in 154 patients over 18 еars of age. All patients were examined at the 1st city clinical hospital named after Ibn Sina in Tashkent. All patients were diagnosed with calcium oxalate urolithiasis. The patients were prescribed diet therapy for the purpose of metaphylaxis of calcium oxalate urolithiasis, a month after the spontaneous passage of the stone or its surgical removal. Over the course of 65 days, the patients' calcium excretion in daily urine was measured over time.
Keywords: Urinary stone disease, Urolithiasis, Calcium oxalate, Metabolic syndrome, Metaphylaxis
Cite this paper: Ermatov N. J., Gaybullaev A. A., Kuchkarov A. K., The Role of a Diet Composed of National Dishes in the Metaphylaxis of Calcium Oxalate Urolithiasis, American Journal of Medicine and Medical Sciences, Vol. 14 No. 11, 2024, pp. 2993-2997. doi: 10.5923/j.ajmms.20241411.70.
Article Outline
1. Introduction
- The urgency of the problem of urolithiasis (STK) occupies one of the leading places among urological diseases. In 2015, the average number of STD patients per 100,000 population in the Russian Federation was 586.4, and in 2020, this figure was 443.2. The main cause of stone formation is metabolic lithogenic disorders. They determine the characteristics of the chemical composition of urinary stones [1].Evaluation of the chemical composition of the stone, in turn, allows to obtain diagnostic information about metabolic diseases that can lead to stone formation in a particular patient. However, only a comprehensive study of the biochemical parameters of blood and urine, as well as the chemical composition of the stone, makes it possible to fully assess the patient's metabolism and determine the processes responsible for stone formation [2].One of the most important social aspects of urolithiasis is its reproducibility. The recurrence rate of urolithiasis within 5 years after the onset of the disease reaches 40% in men and 25% in women [3]. However, at present, treatment against the recurrence of urolithiasis is not yet widely used in urological practice. Many patients do not receive appropriate metaphylactic measures. In turn, the non-wide application of measures to prevent the recurrence of urolithiasis in practice leads to the deterioration of the quality of life of these patients and the need for repeated surgical manipulation of the urinary tract. There are still no generally accepted standards for conducting the necessary examinations and prescribing appropriate therapy for patients with urolithiasis.In recent years, the attention of researchers is increasingly focused on the study of metabolic disorders in STK. This, in turn, provides an opportunity to determine the pathophysiology of urolithiasis, diagnose the disease, and create a metaphylactic algorithm for urethritis. STK is often observed to recur in the body due to the continuation of the metabolic disorder. According to statistical results, the recurrence of urolithiasis is 30-40% within 5 years and 50% after 10 years [5,6].About 80% of kidney stones are composed of calcium inorganic compounds, 60-70% of oxalates, 15-20% of phosphates, and 1-5% of carbonates are found. Most less occurring protein stones in 0.4-0.6% of cases occurs (cystine, xanthine and others) [8,12,20].All urine ways stones between Calcium oxalate stones the most a lot occurs. Theirs to the composition Calcium oxalate hydrates (monohydrate and dihydrate calcium oxalate), sometimes they are urine acid or phosphates with together meeting can [4,6,7] Calcium oxalate minerals harvest to be process passing mattress, organic to the base have Urolith of minerals development and of growth known one at the point this process stops. Mineral layer on thin organic film harvest to be it starts process repetition, as a result harvest happening of the stone internal structure rhythmic - periodic color have will be [9,23]. Such stones density high that it was due to, UTT and X-ray on inspection to determine opportunity high Radial - concentric to the structure have, composition in terms of one character and edges arose stones and hyperuricemia because of harvest strangled of stones crushing usually difficulty gives birth [10].Crystalluria - with urolithiasis in patients of my body metabolic situation pointer and stone harvest of being joint is considered [11,12,13,14]. Stone harvest in being in my body substances exchange correction for ordered conservative cure in effectiveness stone harvest doer of substances in the blood and in the kidney excretion has been amount only not perhaps in the urine of crystals presence too importance occupation and [15,16,17].Calcium oxalate and calcium phosphate shaped in urolithiasis substances of exchange common and spec in their breakdowns in the urine of crystalluria existence of the disease to himself that shows [18,19,20].in STK of a person eating habits stone harvest to be frequency effect does of animals proteins, milk products, soup salt, calcium, sodium or oxalates own into received preparations too much except consumption to do stone formation processes provoke can. Animal proteins too much except consumption to do in the urine Calcium and urine acid level increases in urine ts itrate kon ts entr ati yasini reduces. Some researchers, animals proteins consumption to do idiopathic Calcium with urolithiasis in patients in the urine oxalate concentrate to increase take that he will come are calculated [21].Other of the authors to his opinion than, on the contrary, low protein diet stone harvest to be 5.6 times the risk to increase take kel case is proved [22].Calcium own into received additions acceptance who does in patients urine stones appear to be danger too there is Calcium own into received drugs apply and of urolithiasis spreading between directly dependence observed [5].Sodium consumption of doing increase urine with of calcium release increases and that's it with stone appear to be risk increases. Sodium in the diet amount up to 100 mmol increase of calcium release to 1 mmol to increase possible [10].Calcium oxalate urolithiasis metaphylaxis still own the solution complete It's clear that he didn't find it one approach and don't show lack of urine stone of baldness to be repeated prevention in getting medicine is one of the urgent problems facing the employees of the industry.The purpose of the study is to evaluate the role of the diet made of local products in the metaphylaxis of calcium oxalate urolithiasis.
2. Materials and Methods of Research
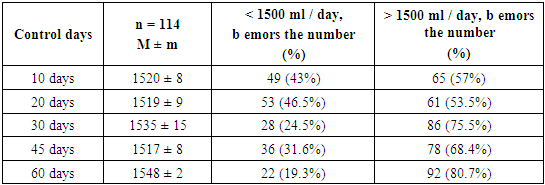
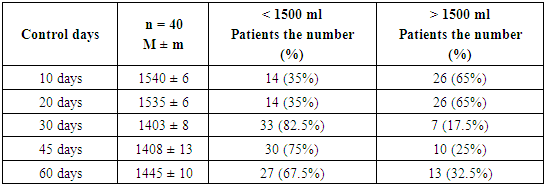
- From January 2022 to December 2022, 154 patients over the age of 18 who were treated with the diagnosis of calcium oxalate urolithiasis at the 1st city clinical hospital named after Ibn Sino, base of the Department of Urology and Andrology of the Moscow State University, were examined.Inclusion criteria: patients aged 18 years or older with a diagnosis of calcium oxalate urolithiasis, independent ureteral stone passage or minimally invasive ureteral stone removal were recruited.Exclusion criteria: under 18 years of age, residual kidney and urinary tract stones, urinary tract infection, urinary tract malformation, chronic kidney disease (glomerulonephritis, chronic kidney disease), gastrointestinal tract disease, diabetes, gout, patients with persistent arterial hypertension.General clinical examination methods: study of complaints, current medical history, collection of information about life history, objective examination, diuresis diaries. Instrumental methods: ultrasound, x-ray (interpretive, excretory urography, radioisotope renography and, if necessary, CT);Laboratory diagnostic methods: general and biochemical blood analysis, measurement of urine pH, studies of urinary metabolic changes (Ca, Ox), determination of crystalluria (CU), study of the mineral composition of stones.Blood Ca was measured to rule out primary hyperparathyroidism (BGPT) before enrolling patients in the study. In case of hypercalcemia (serum Ca above 2.5 mmol/l), the concentration of inorganic phosphorus (Pi) and the content of parathyroid hormone (PTG) in the blood are additionally checked. Patients with symptoms of hyperparathyroidism and elevated parathyroid hormone levels were not included in this study.Urine calcium (Ca) was measured in biochemical analyzers using standard kits.154 patients with uncomplicated calcium stone formation participated in the study. Patients were divided into observation and control groups, 114 patients were included in the observation group and 40 patients in the control group. The observation and control groups were those who underwent kidney stones for the first time and again during their lifetime, stones were detected in the urinary system using UTT, X-ray or MSCT, calcium oxalate urolithiasis (KOU) was detected by laboratory methods, stones fell out of the urinary tract independently or after minimally invasive stone removal. patients with a follow-up period of at least 1 month were included.114 patients were prescribed diet therapy for 65 days based on a diet developed on the basis of national dishes. 40 patients under control were given a recommendation for use in calcium oxalate stones in the standard of diagnosis and treatment of urological diseases approved by the Ministry of Health of the Republic of Uzbekistan.
3. Statistical Analysis of Research Results
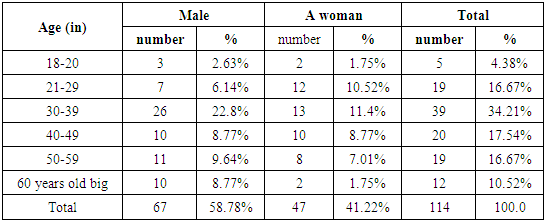
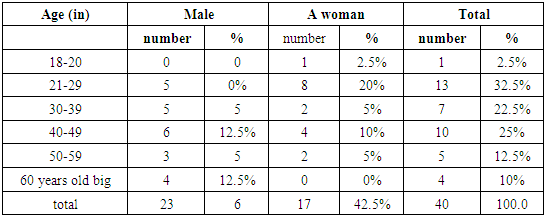
- Principles and methods of evidence-based medicine and variational statistics were used to process and analyze research materials.Statistical processing was carried out on an Intel core i5 personal computer with the help of generally recognized " Microsoft Excel 2020" statistical programs. Arithmetic mean (M), standard deviation (σ) and relative values (frequency,%) were calculated. The statistical significance of the measurements obtained in the comparison of mean values was determined using the Student (t) test (with normal distribution) and the Windows test (in the analysis of non-normally distributed and non-parametric data). The confidence interval (CI) given in the work was constructed for the confidence level p = 95% (in this study, the critical level of significance was taken as 0.05).Analysis of the obtained results. The age and gender distribution of the patients under control is presented in Table 1.
|
|
|

|

|
|
4. Conclusions
- 1. In the daily diet of patients with calcium oxalate urolithiasis, one of the risk factors for the formation of urinary crystals in the urine as a result of weekly diet therapy developed from national dishes for the purpose of metaphylaxis, the average indicator of daily diuresis in the dynamics remained at the normal level of 4.76 ± 0.16 mmol/l 24 hours.2. In the control group, the average value during diet therapy was 6.0 ± 0.16 mmol/l 24 hours showed the result.3. The effectiveness of the diet made from national foods to prevent the recurrence of urolithiasis with calcium oxalate compared to the recommendation given in the standard of diagnosis and treatment of urological diseases was determined.